
Biomarkers May Predict Response to BRAF and MEK inhibitors in Malignant Melanoma
SUMMARY: It is estimated that in the US, approximately 100,350 new cases of malignant melanoma will be diagnosed in 2020 and about 6850 patients are expected to die of the disease. The incidence of melanoma has been on the rise for the past three decades. Surgical resection with a curative intent is the standard of care for patients with early stage melanoma, with a 5-year survival rate of 98% for Stage I disease and 90% for Stage II disease. Patients with locally advanced or metastatic melanoma historically have had poor outcomes. With the development and availability of immune checkpoint inhibitors and BRAF and MEK inhibitors, this patient group now has significantly improved outcomes. In treatment naïve patients receiving anti-PD-1 therapies such as KEYTRUDA® (Pembrolizumab) or OPDIVO® (Nivolumab) in Phase III trials, the Progression Free Survival (PFS) rates have ranged from 27-31%, with an Overall Survival (OS) rate of 46% at 4 years. The 5-year OS among patients receiving KEYTRUDA® was 43%, and in those treated with a combination of OPDIVO® plus YERVOY® (Ipilimumab), 4-year PFS and OS rates were 37% and 53%, respectively.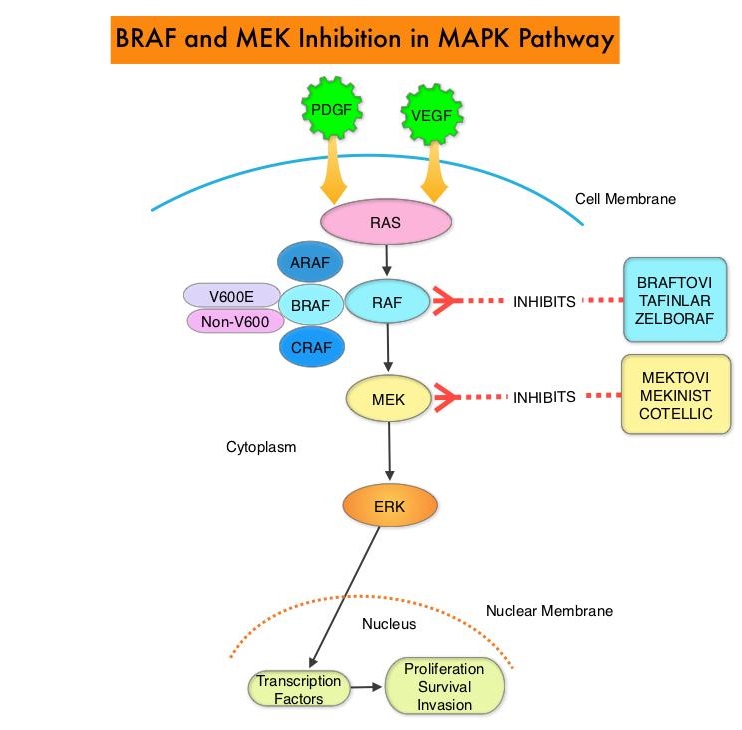
The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. BRAF mutations have been detected in 6-8% of all malignancies. The most common BRAF mutation in melanoma is at the V600E/K site and is detected in approximately 50% of melanomas, and result in constitutive activation of the MAPK pathway.
TAFINLAR® (Dabrafenib), is a selective oral BRAF inhibitor and MEKINIST® (Trametinib) is a potent and selective inhibitor of MEK gene, which is downstream from RAF in the MAPK pathway. Long term survival data pooled from two randomized Phase III COMBI-d and COMBI-v trials, which involved previously untreated, unresectable or metastatic melanoma patients, with BRAFV600E or V600K mutation who had received TAFINLAR® along with MEKINIST® showed PFS rates of 21% at 4 years and 19% at 5 years. The OS rates were 37% at 4 years and 34% at 5 years. The 5-year OS rate was 71% among patients who had a Complete Response and 55% among those who had a normal LDH level plus fewer than three metastatic organ sites at baseline.
With the approval of multiple therapeutic options for the management of patients with BRAF-mutant melanoma, treatment decisions have become increasingly complex. In patients with limited disease burden, immunotherapy with checkpoint inhibitors is favored by most clinicians based on the long term data supporting the durability of responses with immunotherapies. On the contrary, BRAF-targeted agents are utilized in patients with extensive, symptomatic disease and active brain metastases. The optimal sequence of these therapeutic strategies in order to improve long-term patient outcome, has remained unclear.
COMBI-AD is an international, multi-center, randomized, double-blind, placebo-controlled, Phase III trial, in which 870 patients with completely resected, Stage III melanoma and with BRAF V600E or V600K mutations were enrolled. Patients were randomly assigned in a 1:1 to receive TAFINLAR® 150 mg orally twice daily in combination with MEKINIST® 2 mg orally once daily (N=438) or two matched placebos (N=432). Treatment was given for 12 months. At a median follow up of 2.8 years, the estimated 3-year Relapse Free Survival (RFS) rate was 58% with a combination of TAFINLAR® and MEKINIST® and 39% in the placebo group (HR=0.47; P<0.001), and this represented a 53% lower risk of relapse. The risk of distant metastases or death was reduced by 49% with the combination therapy versus placebo (HR=0.51; P<0.001). A prespecified exploratory outcome of this trial was assessment of biomarkers. The authors assessed intrinsic tumor genomic features in 368 patients using Next-Generation DNA sequencing, and tumor microenvironment characteristics were assessed in 507 patients by use of a NanoString RNA assay, in an attempt to provide prognostic and predictive information. Median follow up at data cutoff was 44 months in the TAFINLAR® plus MEKINIST® group and 42 months in the placebo group.
Baseline MAPK pathway genomic alterations did not affect treatment benefit or outcomes in either treatment groups. An Interferon Gamma gene expression signature higher than the median was prognostic for prolonged RFS in both treatment groups. Tumor Mutational Burden (TMB) was independently associated with better RFS in the placebo group (HR for top third versus bottom third of TMB values=0.56; P=0.0056), but this benefit was not seen in the TAFINLAR® plus MEKINIST® group (HR= 0.83; P=0.44). However, patients with TMB in the lower two terciles who received TAFINLAR® plus MEKINIST® combination had improved RFS compared to those who received placebo (HR=0.49: P<0.0001). Patients with high TMB appeared to have a less pronounced benefit with TAFINLAR® plus MEKINIST® targeted therapy, compared to placebo, especially if they had an Interferon Gamma gene expression signature lower than the median.
It was concluded from this biomarker analysis that high Tumor Mutational Burden was independently associated with better Relapse Free Survival in the placebo group but not in the TAFINLAR® plus MEKINIST® combination group, and an Interferon Gamma gene expression signature higher than the median was prognostic for prolonged RFS in both treatment groups. Adjuvant dabrafenib plus trametinib versus placebo in patients with resected, BRAFV600-mutant, stage III melanoma (COMBI-AD): exploratory biomarker analyses from a randomised, phase 3 trial. Dummer R, Brase JC, Garrett J, et al. The Lancet Oncology. Published:January 30, 2020DOI:https://doi.org/10.1016/S1470-2045(20)30062-0
Author: RR
KISQALI® plus FASLODEX® Improve Overall Survival in Advanced Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease. Approximately 70% of breast tumors express Estrogen Receptors and/or Progesterone Receptors. The most common subtype of metastatic breast cancer is Hormone Receptor-positive (HR-positive), HER2-negative breast cancer (65% of all metastatic breast tumors), and these patients are often treated with anti-estrogen therapy as first line treatment. However, resistance to hormonal therapy occurs in a majority of the patients, with a median Overall Survival (OS) of 36 months. Cyclin Dependent Kinases (CDK) play a very important role to facilitate orderly and controlled progression of the cell cycle. Genetic alterations in these kinases and their regulatory proteins have been implicated in various malignancies.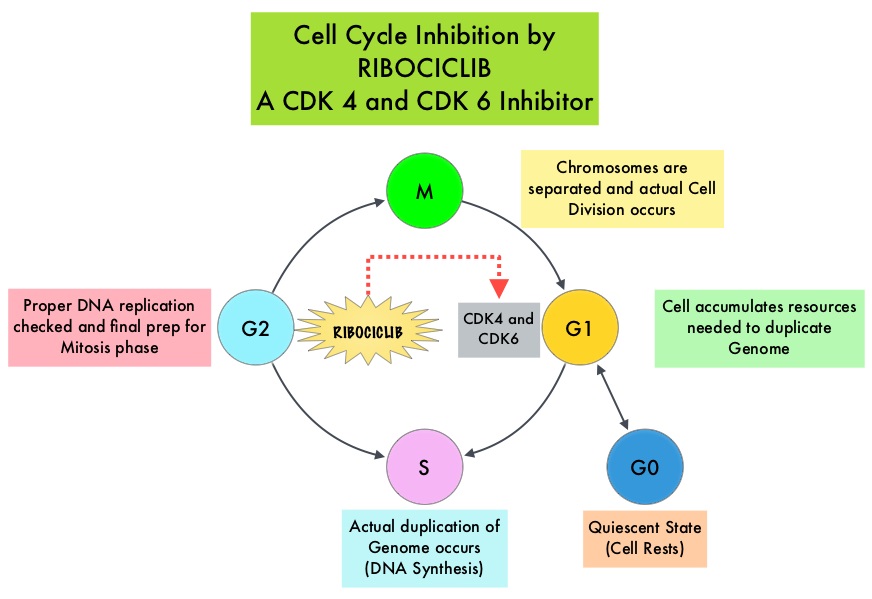
Cyclin Dependent Kinases 4 and 6 (CDK4 and CDK6) phosphorylate RetinoBlastoma protein (RB), and initiate transition from the G1 phase to the S phase of the cell cycle. RetinoBlastoma protein has antiproliferative and tumor-suppressor activity and phosphorylation of RB protein nullifies its beneficial activities. CDK4 and CDK6 are activated in hormone receptor positive breast cancer, promoting breast cancer cell proliferation. Further, there is evidence to suggest that endocrine resistant breast cancer cell lines depend on CDK4 for cell proliferation. The understanding of the role of Cyclin Dependent Kinases in the cell cycle, has paved the way for the development of CDK inhibitors.
KISQALI® (Ribociclib) is an orally bioavailable, selective, small-molecule inhibitor of CDK4/6, that blocks the phosphorylation of RetinoBlastoma protein, thereby preventing cell-cycle progression and inducing G1 phase arrest. KISQALI® in combination with an Aromatase Inhibitor has been approved by the FDA for pre and perimenopausal women with HR (Hormone Receptor)-positive, HER2-negative advanced or metastatic breast cancer, as initial endocrine-based therapy. The efficacy of KISQALI® was evaluated in two prior randomized Phase III studies. In the MONALEESA-2 trial which evaluated KISQALI® in combination with FEMARA® (Letrozole) compared to FEMARA® alone, in postmenopausal women with HR-positive, HER2-negative advanced breast cancer, who received no prior therapy for their advanced breast cancer, the addition of KISQALI® to FEMARA® significantly prolonged Progression Free Survival (PFS) compared to FEMARA® alone. In the MONALEESA-7 study, KISQALI® in combination with Tamoxifen or a Non-Steroidal Aromatase Inhibitor plus ZOLADEX® (Goserelin) was compared with Tamoxifen or an Aromatase Inhibitor plus ZOLADEX®, in premenopausal or perimenopausal women with HR-positive, HER2- negative advanced breast cancer, who had not previously received endocrine therapy for advanced disease. In this study of premenopausal women, KISQALI® plus endocrine therapy significantly improved PFS and OS, compared with placebo plus endocrine therapy.
MONALEESA-3 is a randomized, double-blind, placebo-controlled Phase III study which compared the efficacy of KISQALI® in combination with FASLODEX® with FASLODEX® alone, among postmenopausal women with HR-positive, HER2-negative advanced breast cancer, who received no prior or only one line of prior endocrine therapy for advanced disease. In this trial, 726 women were randomized, of whom 367 were treatment-naïve and 345 patients had received up to one line of prior endocrine therapy for advanced disease. . Patients were randomized 2:1 to receive KISQALI® plus FASLODEX® (N=484) or placebo plus FASLODEX® (N=242). Treatment consisted of KISQALI® 600 mg orally daily 3 weeks on and 1 week off and FASLODEX® 500 mg IM on day 1 of each 28-day cycle, with an additional dose given on day 15 of cycle 1. Patients were stratified by the presence or absence of lung or liver metastases and prior endocrine therapy (first-line versus second-line). The median age in both groups was 63 years. The Primary endpoint was Progression Free Survival (PFS). Secondary end points included Overall Survival (OS), Overall Response Rate (ORR), and Safety.
In the primary analysis of the trial, the median PFS in the KISQALI® plus FASLODEX® group was 20.5 months compared to 12.8 months in the FASLODEX® plus placebo group (HR= 0.59; P<0.001). This represented a 41% reduction in the risk of disease progression. The authors now report the results of the second interim analysis of Overall Survival and an updated analysis of Progression Free Survival. The median duration of follow up for all patients was 39.4 months, and the median duration of treatment was 15.8 months in the KISQALI® group and 12.0 months in the placebo group.
There was a significant Overall Survival benefit with KISQALI® plus FASLODEX® compared to placebo plus FASLODEX®. The estimated Overall Survival at 42 months was 57.8% in the KISQALI® group compared to 45.9% in the placebo group, and this represented a 28% reduction in the relative risk of death with the KISQALI® combination (HR=0.72; P=0.00455). The survival benefit was consistent across most subgroups. The median PFS among patients receiving first line treatment was 33.6 months (95% CI, 27.1 to 41.3) in the KISQALI® group and 19.2 months in the placebo group. No new safety signals were observed during this longer follow up period.
It was concluded that KISQALI® plus FASLODEX® significantly improved Overall Survival compared to placebo plus FASLODEX® in patients with HR-positive, HER2-negative advanced breast cancer, regardless of whether they received their treatment in the frontline setting or subsequently. Overall Survival with Ribociclib plus Fulvestrant in Advanced Breast Cancer. Slamon DJ, Neven P, Chia S, et al. N Engl J Med 2020;382:514-524
NELSON Trial Confirms that Low-Dose CT Screening Reduces Lung Cancer Mortality
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2020, about 228, 820 new cases of lung cancer will be diagnosed and 135,720 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer.
In the National Lung Screening Trial (NLST) with Low Dose CT (LDCT) screening for lung cancer, there was a 20% reduction in mortality. Following the publication of the results of NLST and NCCN issued guideline in 2011, the United States Preventive Services Task Force (USPSTF) recommended Lung Cancer screening with Low Dose CT scan in high risk patients. CMS in 2015 determined that there was sufficient evidence to reimburse for this preventive service.
Despite the evidence and recommendation along with supportive public policies, screening with LDCT has not been adequately implemented in the US healthcare system. Low Health Care Provider knowledge of the Lung Cancer Screening (LCS) guidelines represents a potential barrier to implementation. Additionally, despite the unequivocal findings from the NLST, several countries have not adopted this guideline due to early publication of inconclusive results from a number of smaller trials in Europe. Further, there are limited data from randomized trials regarding whether nodule volume-based, low-dose CT screening can reduce lung cancer mortality among male former and current smokers.
The Dutch-Belgian lung cancer screening trial, NELSON (Nederlands–Leuvens Longkanker Screenings Onderzoek ) is a population-based, randomized, controlled trial initiated in 2000. The goal of the study was to show a 25% or more reduction in lung cancer mortality, in high-risk male participants at 10 years of follow-up, utilizing volume-based, low-dose CT lung cancer screening. The authors in this publication reported the incidence of lung cancer, associated mortality, and the performance of the four rounds of low-dose CT screening for lung cancer in the this trial, among male participants (main analysis) and female participants (subgroup analyses).
In this study, a total of 13,195 men aged 50-74 years were randomly assigned to undergo CT screening at baseline, year 1, year 3, and year 5.5 (N = 6,583) or no screening (N=6,612). At the time of initiation of this trial, only a small number of women were eligible, as smoking was much less prevalent and intense among women, than among men. Because of the relevance and importance of the inclusion of women in this study, high-risk women were later allowed to participate (N=2594). Participants were current or former smokers who had quit 10 or fewer years ago, who had smoked more than 15 cigarettes a day for more than 25 years, or more than 10 cigarettes a day for more than 30 years. About 45% of the male participants were former smokers.
At 10 years of follow up, lung cancer mortality among men was 24% lower in the screening group than in the control group (Rate Ratio=0.76; P=0.01), and 33% lower among women (Rate Ratio=0.67). The CT screening compliance among men was 90% and approximately 9.2% of the screened participants underwent at least one additional CT scan due to an indeterminate screening test. Screening-detected lung cancers were substantially more often diagnosed in Stage IA or IB (58.6%) and were Adenocarcinomas (52.0% in the screening group and 43.8% in the control group).
It was concluded that in this trial involving high-risk individuals, lung cancer mortality was significantly lower among those who underwent CT screening with determination of nodule volume, than among those who underwent no screening. Adherence to CT screening was very high, with low rates of follow up procedures for results suggestive of lung cancer. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. de Koning H.J., van der Aalst C.M., de Jong P.A., et al. N Engl J Med 2020;382:503-513
Assessment of Molecular Relapse Detection in Early Stage Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease. Majority of the breast cancer patients present with early stage disease without macroscopic metastatic disease. Several small proof of principle studies have shown that detection of circulating tumor DNA (ctDNA) in the peripheral blood may identify patients at risk of relapse following definitive therapy. ctDNA refers to DNA fragments that are shed into the bloodstream by cancer cells after apoptosis or necrosis. ctDNA can detect almost all molecular alterations present in cancer cells and the proportion of ctDNA that originates from a tumor depends on the anatomic location, tumor burden and cell turnover. ctDNA allows real-time monitoring for treatment response and resistance.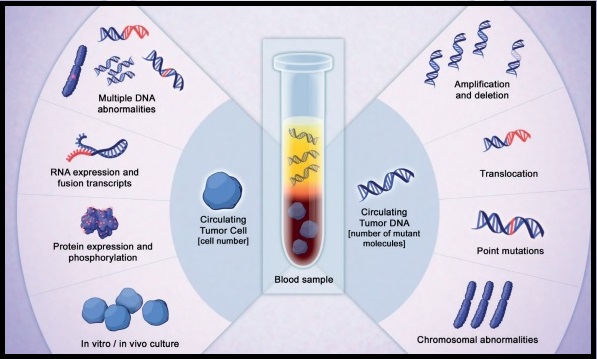
To assess the clinical validity of molecular relapse detection with circulating tumor DNA (ctDNA) analysis in early-stage breast cancer, the authors conducted a multicenter, prospective study in the UK over a 5 year period, and included patients, irrespective of their hormone receptor or HER2 status, who were receiving neoadjuvant chemotherapy followed by surgery or surgery before adjuvant chemotherapy. All patients had primary breast cancer without evidence of distant metastatic disease and patients scheduled to receive standard neoadjuvant chemotherapy followed by surgery consented for plasma sample collection before chemotherapy, and patients scheduled to receive adjuvant chemotherapy consented for plasma sample collection after surgery and before chemotherapy. This study enrolled 170 women, and somatic mutations were identified in 101 patients, and this formed the primary analysis cohort and secondary analyses were conducted on a combined cohort of 144 patients, including 43 patients previously analyzed in a proof of principle study (N=101+43). Tumor DNA extracted from the primary tumor was sequenced to identify somatic mutations to track in plasma, and personalized tumor-specific digital Polymerase Chain Reaction (dPCR) assays were designed to monitor these somatic mutations in serial plasma samples collected from patients every 3 months during the first year of follow up, and subsequently every 6 months for 5 years. ctDNA testing can identify genetic alterations unrelated to the lesion of interest (Clonal Hematopoiesis of Indeterminate Potential- CHIP). The authors analyzed buffy coat DNA to control for CHIP, which is common with increasing age and can potentially cause false-positive results in ctDNA analysis. The mean patient age was 54 years and the median follow up was 35.5 months. The Primary objective of the study was to assess whether patients with ctDNA detected in follow-up blood samples had worse Relapse Free Survival than patients without detectable ctDNA. Secondary end points included lead time between ctDNA detection and relapse, and association between detection of ctDNA in the diagnosis sample before neoadjuvant chemotherapy and relapse.
Results from the combined cohort of 144 patients showed that detection of ctDNA during follow up was associated with relapse (88.4% of patients who experienced relapse had antecedent ctDNA detection- P<0.001). Detection of ctDNA at diagnosis, before any treatment, was associated with larger tumor size and higher tumor grade, and patients with Triple Negative Breast Cancer (TNBC) had the highest level of ctDNA, likely due to high proliferative rates and cell turnover. This patient group was at a higher risk to relapse. Further, ctDNA detection had a median lead time of 10.7 months before clinical relapse and was associated with relapse in all breast cancer subtypes. Distant extracranial metastatic relapse was detected by ctDNA in 96% of patients. Brain-only metastasis however was less commonly detected by ctDNA, suggesting that cranial metastases are less readily detectable by ctDNA analysis.
It was concluded that detection of ctDNA during follow up of early-stage breast cancer is associated with a high risk of future relapse. A clinical trial is underway evaluating the benefit of treatment initiation at molecular relapse, before clinical development of metastatic disease. Assessment of Molecular Relapse Detection in Early-Stage Breast Cancer. Garcia-Murillas I, Chopra N, Comino-Méndez I, et al. JAMA Oncol.2019;5:1473-1478.
H. pylori Eradication Treatment Reduces the Risk of Gastric Cancer in High Risk Population
SUMMARY: The American Cancer Society estimates that in the US, about 27,600 new cases of stomach cancer will be diagnosed in 2020 and about 11,010 people will die of the disease. It is one of the leading causes of cancer-related deaths in the world. The incidence of gastric cancer in the US has been on the decline and has been attributed to increased use of refrigeration for food storage, making fresh fruits and vegetables more available, and decreased the use of salted and smoked foods. In the United States, Asians and Hispanics have a much higher incidence of gastric cancer.
Several hereditary syndromes such as Hereditary Diffuse Gastric Cancer (HDGC), Lynch syndrome (Hereditary Nonpolyposis Colorectal Cancer) and Familial Adenomatous Polyposis (FAP) have been associated with a predisposition for stomach cancer. HDGC however, is the most common genetic predisposing syndrome for gastric cancer, with germline mutations of the E-cadherin gene (CDH1), detected in 30-50% of diffuse-type gastric cancers. Women with CDH1 mutations are also at an increased risk for breast cancer, and the follow up is similar to BRCA1/BRCA2 mutation carriers. A family history of gastric cancer in a first-degree relative is associated with double to triple the risk of gastric cancer. Gastric cancer overall has a poor prognosis and the 5 year Overall Survival rate is about 25%.
The strongest risk factor for gastric adenocarcinoma is infection with Helicobacter pylori (H.pylori), which is a gram-negative, spiral-shaped microaerophilic bacterium. This bacterial species colonizes the stomach and the overall estimate of H. pylori prevalence in adults is 76% in developing countries and 58% in developed countries. The association between H.pylori and gastric cancer has been shown in observational and case-control studies. In a recently published randomized trial (NEJM 2018;378:1085-1095), treatment of H. pylori infection in patients with early gastric cancer reduced the risk of metachronous gastric cancer by 50%.
It has been unclear whether treatment to eradicate H. pylori can reduce the risk of gastric cancer in individuals with a family history of gastric cancer in first-degree relatives. To address this question, the authors in this single-center, double-blind, placebo-controlled trial, randomly assigned 1838 participants with H. pylori infection and at least one first-degree relative with gastric cancer, in a 1:1 ratio to receive either H.pylori eradication therapy with Amoxicillin 1000 mg, Clarithromycin 500 mg, and Proton-Pump Inhibitor Lansoprazole 30 mg, each taken twice daily for 7 days or placebo. Eligible participants were 40-65 years of age and key exclusion criteria included a history of gastric cancer, peptic ulcer, or other malignancy, and previous eradication therapy for H. pylori. Surveillance endoscopies were performed every 2 years and suspicious lesions were biopsied for gastric cancer. A closeout endoscopy, with H. pylori evaluation, was performed at the end of the trial period. The Primary outcome was development of gastric cancer. A prespecified Secondary outcome was development of gastric cancer according to H. pylori eradication status, assessed during the follow-up period after receipt of H. pylori treatment or placebo. A total of 1676 participants (832 in the treatment group and 844 in the placebo group) were included in the primary outcome analysis.
During a median follow up of 9.2 years, the risk of gastric cancer was 55% lower among those who received H. pylori eradication treatment than among those who received placebo (HR=0.45; P=0.03). Among those who received treatment for H. pylori, the risk of gastric cancer was 73% lower among persons in whom H. pylori eradication was achieved than among those in whom infection was persistent (HR=0.27). Adverse events were common in the treatment group than in the placebo group (53% versus 19.1%; P<0.001), but were mild.
It was concluded that among individuals with H. pylori infection and a family history of gastric cancer in first-degree relatives, H. pylori eradication treatment significantly reduced the risk of gastric cancer. Family History of Gastric Cancer and Helicobacter pylori Treatment. Choi IJ, Kim CG, Lee JY, et al. N Engl J Med 2020;382:427-436
Multigene Testing for All Patients with Breast Cancer Could Identify Many More Mutation Carriers
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately 279,100 new cases of invasive breast cancer will be diagnosed in 2020 and about 42,690 individuals will die of the disease. DNA can be damaged due to errors during its replication or as a result of environmental exposure to ultraviolet radiation from the sun or other toxins. The tumor suppressor genes such as BRCA1 (Breast Cancer 1) and BRCA2 help repair damaged DNA and thus play an important role in maintaining cellular genetic integrity, failing which these genetic aberrations can result in malignancies. The BRCA1 gene is located on the long (q) arm of chromosome 17 whereas BRCA2 is located on the long arm of chromosome 13. These mutations can be inherited from either of the parents in an Autosomal Dominant pattern and a child has a 50% chance of inheriting this mutation, and the deleterious effects of the mutations are seen even when an individual’s second copy of the gene is normal.
It is estimated that BRCA1/2 gene mutations occur in approximately 1 in 400 women in the general population and account for 20-25% of hereditary breast cancers, about 5-10% of all breast cancers and 15% of ovarian cancers. Mutations in the BRCA1/2 genes increase breast cancer risk 45-65% by age 70 years. The risk of ovarian, fallopian tube, or peritoneal cancer, increases to 39% for BRCA1 mutations, and 10-17% for BRCA2 mutations. PALB2 (Partner And Localizer of BRCA2) gene provides instructions to make a protein that works along with the BRCA2 protein, to repair damaged DNA. PALB2 mutation is rare in sporadic breast cancer, and is considered a high-penetrance breast cancer predisposing gene associated with 14% risk of developing breast cancer by age 50 and a 35% risk of developing breast cancer by age 70. Women with a PALB2 mutation face an increased risk of triple negative breast cancer and higher risk of death from breast cancer. PALB2 gene mutations have also been implicated in ovarian, pancreatic and other malignancies.
Current guidelines recommend genetic testing in women with breast cancer who fulfill recognized or established family history or clinical criteria. However, patients with breast cancer and genetic pathogenic variants do not always have a positive family history, and these criteria miss approximately 50% of pathogenic variant carriers. Further, genetic testing based on family history or clinical criteria depends on the awareness and understanding both by the health care providers and patients, and appropriate referrals to genetic counselors. Because of limited awareness and restricted access to genetic testing and counseling services, only 20-30% of eligible patients undergo genetic testing, and 97% of estimated carriers in the general population remain unidentified, thereby missing substantial opportunities for primary prevention.
Knowledge of a patient’s genetic pathogenic variant status has important therapeutic and prognostic implications. Identifying unaffected relatives carrying pathogenic variants enables early diagnosis and cancer prevention by offering risk management options such as enhanced MRI imaging and mammography screening, risk-reducing surgeries such as prophylactic mastectomy, salpingo-oopherectomy and chemoprevention with Selective Estrogen Receptor Modulators.
The authors in this study estimated the downstream health effects, costs and cost-effectiveness of multigene testing for all patients with breast cancer, compared with current practice of BRCA testing based on clinical criteria or family history alone. In this modeling study, data was incorporated from four large breast cancer clinical trials and/or research cohorts in the United States, United Kingdom, and Australia. This analysis included 11,836 women with invasive breast cancer, regardless of the family history, and compared lifetime costs and effects of high-risk BRCA1/BRCA2/PALB2 (multigene) testing of all unselected patients with breast cancer (Strategy A) with BRCA1/BRCA2 testing based on family history or clinical criteria (Strategy B), in UK and US populations, from January 1, 2018, through June 8, 2019.
Affected patients with BRCA/PALB2 mutations could undertake contralateral preventive mastectomy and BRCA carriers could choose Risk-Reducing Salpingo-Oophorectomy (RRSO). If patients had a BRCA1/BRCA2/PALB2 pathogenic variant, their first-degree relatives undergo testing for the familial pathogenic variant. If the first-degree relative had a BRCA1/BRCA2/PALB2 pathogenic variant, second-degree relatives undergo testing. Unaffected relative carriers could undergo MRI or mammography screening, chemoprevention, or risk-reducing mastectomy for breast cancer risk and RRSO for ovarian cancer risk. This analysis incorporated lifetime risks and long-term consequences to provide a lifetime horizon. Incidence of ovarian cancer, breast cancer, excess deaths due to heart disease, and the overall population effects were estimated.
Multigene testing was restricted to BRCA1/BRCA2/PALB2, to comply with the ACCE framework for genetic testing, which was advocated for clinical applicability of genetic testing. The ACCE framework includes Analytic validity which is technical test performance, Clinical validity which is the ability of a genetic test to identify or predict accurately and reliably the clinically defined disorder or phenotype of interest, Clinical utility which is evidence that a genetic test improves clinical outcomes measurably and that it adds value for patient management decision making compared with current management without genetic testing, and ELSI which are the complex Ethical, Legal, and Social Implications associated with genetic tests.
This study showed that unselected BRCA1/BRCA2/PALB2 testing for all patients at breast cancer diagnosis was extremely cost-effective compared with BRCA1/BRCA2 testing based on clinical criteria or family history for both UK and US health systems, with incremental cost-effectiveness ratios of £10,464 or £7,216 and $65,661 or $61,618 per Quality-Adjusted Life-Year, respectively. Quality-Adjusted Life-Year (QALY) is a measurement of health outcomes in economic evaluations recommended by NICE (National Institute of Health and Clinical Excellence). This is well below UK and US cost-effectiveness thresholds. The authors estimated that one year’s unselected panel genetic testing could prevent 1142 cases of breast cancer, 959 cases of ovarian cancer, and 633 deaths related to breast or ovarian cancer in the UK. In the US, one year’s unselected panel genetic testing could prevent 5478 cases of breast cancer, 4255 cases of ovarian cancer, and 2406 deaths related to breast or ovarian cancer.
It was concluded from this analysis that unselected, high-risk multigene testing for all women with breast cancer is extremely cost-effective, compared with testing based on family history or clinical criteria, and could identify many more mutation carriers who can benefit from precision prevention. The authors added that these findings support changing current policy to expand genetic testing to all women with breast cancer. A Cost-effectiveness Analysis of Multigene Testing for All Patients with Breast Cancer. Sun L, Brentnall A, Patel S, et al. JAMA Oncol. 2019;5:1718-1730
Late Breaking Abstract – ASH 2019: DARZALEX®, KYPROLIS® and Dexamethasone Combination Improves PFS in Relapsed or Refractory Multiple Myeloma
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, 32, 270 new cases will be diagnosed in 2020 and 12,830 patients are expected to die of the disease. Multiple Myeloma (MM) in 2020 remains an incurable disease. The therapeutic goal therefore is to improve Progression Free Survival (PFS) and Overall Survival (OS). Multiple Myeloma is a disease of the elderly, with a median age at diagnosis of 69 years and characterized by intrinsic clonal heterogeneity. Almost all patients eventually will relapse, and patients with a high-risk cytogenetic profile or refractory disease have the worst outcomes. The median survival for patients with Myeloma is over 10 years.
REVLIMID® (Lenalidomide) in combination with VELCADE® (Bortezomib) and Dexamethasone is the preferred regimen according to the NCCN guidelines, for both transplant and non-transplant candidates with newly diagnosed Multiple Myeloma, and when given continuously or with maintenance therapy, has improved survival outcomes. Nonetheless, a significant number of patients progress while on these agents or discontinue therapy due to toxicities. There is therefore a need for effective and tolerable regimens for patients who are exposed or refractory to REVLIMID® or VELCADE®.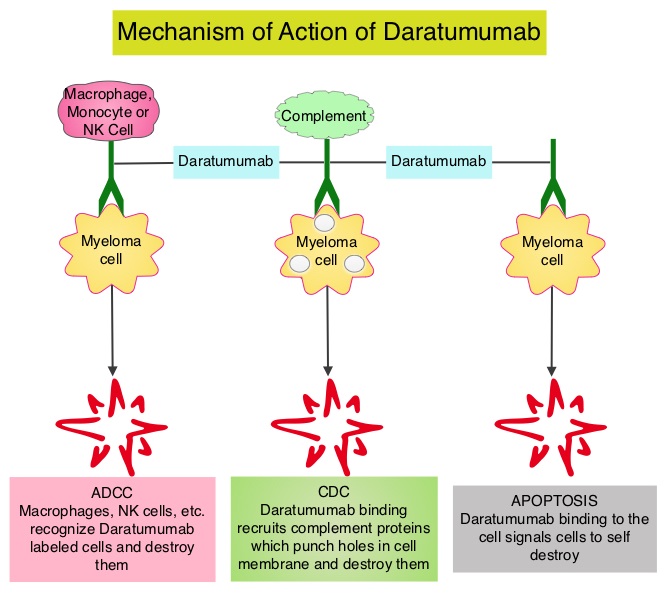
KYPROLIS® (Carfilzomib) is a second generation selective, epoxyketone Proteasome Inhibitor and unlike VELCADE®, proteasome inhibition with KYPROLIS® is irreversible. DARZALEX® (Daratumumab) is a human IgG1 antibody that targets CD38, a transmembrane glycoprotein abundantly expressed on malignant plasma cells and with low levels of expression on normal lymphoid and myeloid cells. DARZALEX® exerts its cytotoxic effect on myeloma cells by multiple mechanisms, including Antibody Dependent Cellular Cytotoxicity (ADCC), Complement Dependent Cytotoxicity (CDC) and direct Apoptosis. Additionally, DARZALEX® may play a role in immunomodulation, by depleting CD38-positive regulator immune suppressor cells, and thereby expanding T cells, in patients responding to therapy. Both KYPROLIS® and DARZALEX® are approved as single agents, as well as in combination with other drugs, for the treatment of patients with Relapsed/Refractory Multiple Myeloma. In a Phase I study, KYPROLIS® in combination with Dexamethasone and DARZALEX® demonstrated safety and efficacy in patients Relapsed/Refractory Multiple Myeloma.
CANDOR is a multicenter, open-label, Phase III trial, which included Relapsed/Refractory Multiple Myeloma patients with measurable disease who had received 1-3 prior lines of therapy, with Partial Response or better to one or more lines of therapy. A total of 466 patients were randomly assigned 2:1 to receive triplet of KYPROLIS®, Dexamethasone, and DARZALEX® (KdD)- N=312 or KYPROLIS® and Dexamethasone (Kd) alone- N=154. All patients received KYPROLIS® as a 30 minute IV infusion on days 1, 2, 8, 9, 15, and 16 of each 28-day cycle (20 mg/m2 on days 1 and 2 during cycle 1 and 56 mg/m2 thereafter). DARZALEX® 8 mg/kg was administered IV on days 1 and 2 of cycle 1 and at 16 mg/kg once weekly for the remaining doses of the first 2 cycles, then every 2 weeks for 4 cycles (cycles 3-6), and every 4 weeks thereafter. All patients received Dexamethasone 40 mg oral or IV weekly (20 mg for patients over 75 years of age). The median age was 64 years, 42% and 90% received prior REVLIMID® and VELCADE® (Bortezomib) containing regimens respectively, and a third of patients were refractory to REVLIMID®. The Primary endpoint was Progression Free Survival (PFS) and Secondary endpoints including Overall Response Rate (ORR), Minimal Residual Disease (MRD)-negative status, Complete Response (CR) rate at 12 months, Overall Survival (OS), Duration of Response, and Safety.
After a median follow up of 17 months, the study met its Primary endpoint and the median PFS was not reached for the KdD arm and was 15.8 months for the Kd arm (HR=0.63; P=0014). This represented a 37% reduction in the risk of progression or death in the KdD group. The PFS benefit of KdD was maintained across prespecified subgroups, particularly among REVLIMID®-exposed and REVLIMID®-refractory patients. The ORR was 84.3% in the KdD group versus 74.7% in the Kd group (P=0.004), with a CR rate or better of 28.5% versus 10.4% respectively. The median time to first response was one month in both treatment groups. Patients treated with KdD achieved deeper responses which was nearly 10 times higher, with a MRD-negative Complete Response rate at 12 months of 12.5% for KdD versus 1.3% for Kd (P<0.0001). The median treatment duration was longer in the KdD group compared to the Kd group (70.1 versus 40.3 wks). The median OS was not reached in either groups, at a median follow up time of 17 months. Toxicities were generally manageable and the incidence of Adverse Events leading to treatment discontinuation was similar in both treatment groups.
It was concluded that a combination of KYPROLIS® along with Dexamethasone and DARZALEX® resulted in a significant PFS benefit over KYPROLIS® and Dexamethasone alone, with deeper responses, and the PFS benefit of KdD was maintained across prespecified, clinically important subgroups, particularly REVLIMID®-exposed and REVLIMID®-refractory patients. The authors added that KdD regimen should be considered as a novel, efficacious, and tolerable immunomodulatory-free treatment option for Relapsed/Refractory Multiple Myeloma patients. Carfilzomib, Dexamethasone, and Daratumumab Versus Carfilzomib and Dexamethasone for the Treatment of Patients with Relapsed or Refractory Multiple Myeloma (RRMM): Primary Analysis Results from the Randomized, Open-Label, Phase 3 Study Candor (NCT03158688). Usmani SZ, Quach H, Mateos M-V, et al. Presented at the 61st American Society of Hematology Annual Meeting and Exposition; Orlando, Florida; December 7-10, 2019; Abstract LBA-6.
Lung Immune Prognostic Index (LIPI) is an Important Prognostic Biomarker for Patients with Advanced Non Small Cell Lung Cancer
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2020, about 228, 820 new cases of lung cancer will be diagnosed and 135,720 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer.
Immunotherapy with PD-1/PD-L1 (Programmed Death-1/Programmed Death-Ligand 1) inhibitors, also called Immune Checkpoint Inhibitors (ICIs), has changed the treatment paradigm for patients with advanced NSCLC. In previously treated patients with NSCLC, the Overall Response Rates (ORR) with single agent Immune Checkpoint Inhibitors (ICIs) range from 14-20%, with median Overall Survival (OS) of 10 to 12 months. In those with PD-L1 expression of 50% or more by ImmunoHistoChemical (IHC) analysis, the ORR can reach up to 30% with a median OS of 20 months. However, in patients with negative or weak PD-L1 expression (1%-49% positive tumor cells), who account for approximately two thirds of the NSCLC population, the response rates range from 8-19% with a median OS slightly below 10 months. Even among those with tumors expressing PD-L1 expression of 50% or more, not all patients benefit from Immunotherapy with ICIs. Therefore identifying biomarkers for patients likely to respond to ICI therapy, and predicting resistance is important and relevant in selecting the appropriate patients for treatment with ICIs.
There is growing evidence on the role of inflammation in cancer biology and systemic inflammatory response may have prognostic significance in different cancer types. Inflammatory process in various cancers imparts immunoresistance to ICIs, by activating oncogenic signaling pathways, there by promoting cancer growth and dissemination, with resulting poor outcomes. Derived Neutrophil-to-Lymphocyte ratio (dNLR) and serum Lactate DeHydrogenase (LDH) level have been investigated as potential inflammatory biomarkers in patients with cancer. The dNLR is calculated using a formula dNLR= Absolute Neutrophil Count/(White Blood Count minus Absolute Neutrophil Count). These ratios are simple and easy to calculate from routine blood tests. Both these biomarkers have been correlated with Immune Checkpoint Inhibitor outcomes, in patients with melanoma. In two large studies involving patients with advanced melanoma treated with Ipilimumab and Pembrolizumab, dNLR of 3 or more and LDH of at least 2.5 times Upper Limit of Normal (ULN), reflected a pro-inflammatory status and resulted in poor outcomes.
Based on this important finding in malignant melanoma, Mezquita L and colleagues (JAMA Oncol. 2018;4:351-357) conducted a multicenter, retrospective study involving 466 patients treated with ICIs, to determine whether combining the two factors – pretreatment dNLR and LDH (Lung Immune Prognostic Index-LIPI), was associated with resistance to ICIs in patients with advanced NSCLC. In this study, LIPI was developed on the basis of dNLR (derived Neutrophil-to-Lymphocyte Ratio) of greater than 3 and LDH greater than Upper Limit of Normal (ULN). LIPI was used to stratify patients with NSCLC into 3 groups (Good= 0 factors; Intermediate= 1 of 2 factors, Poor= 2 factors). The authors based on this study concluded that pretreatment LIPI, combining derived Neutrophil-to-Lymphocyte ratio (dNLR) greater than 3 and serum LDH level greater than Upper Limit of Normal, correlated with worse outcomes for Immune Checkpoint Inhibitors (ICIs).
To determine whether LIPI score provides prognostic information for patients with metastatic NSCLC, the authors in this publication performed an exploratory retrospective analysis of the LIPI on pooled clinical trial data from 11 randomized multinational studies (5 ICI trials and 6 targeted therapy trials), and in the final analysis included 3987 patients treated with ICIs, targeted therapy, or cytotoxic chemotherapy, between January 1, 2013, and December 31, 2017. In the 5 ICI trials (N = 2440), 1368 patients received ICIs and 1072 received cytotoxic chemotherapy. In the 6 targeted therapy trials (N = 1547), 53% of EGFR mutant and 47.1% of ALK positive patients received targeted therapy 32.0% of EGFR mutant and 68% of ALK positive patients received cytotoxic chemotherapy. Baseline demographics and disease characteristics were relatively balanced between groups. Lung Immune Prognostic Index (LIPI) scores were calculated based on the dNLR and the LDH level, as mentioned elsewhere in this document.
For patients receiving ICIs, a good LIPI score was associated with longer Overall Survival (OS) compared with a poor LIPI score, with an estimated median survival of 15.6 versus 4.5 months (HR=0.34). A similar prognostic association was observed for patients who received cytotoxic chemotherapy, with patients having a good LIPI score having a longer survival than patients with a poor score, with an estimated median survival of 10.4 versus 5.3 months (HR=0.49). Similar associations were also noted between good LIPI scores and longer Progression Free Survival (PFS). As expected, PD-L1 expression of 1% or more, as well as higher albumin levels was independently associated with improved outcomes.
Among patients with tumors harboring either ALK alterations or EGFR-activating mutations who received targeted therapy, those with a good LIPI score had an estimated median survival of 46.5 months compared with 16.6 months for those with a poor score (HR=0.28). A similar prognostic association was observed in this patient group receiving cytotoxic chemotherapy, with patients having a good LIPI score experiencing a longer survival than patients with a poor score (estimated median survival of 33.4 months versus 17.1 months (HR=0.41). Further, similar associations between LIPI score and PFS were observed. For patients enrolled in these studies, regardless of receiving targeted therapy or cytotoxic chemotherapy, multivariable analysis consistently showed that LIPI score was independently associated with OS and PFS.
It was concluded from this analysis that pretreatment LIPI risk score may be an important prognostic biomarker, irrespective of pharmacologic class of treatment, for patients with metastatic NSCLC. Prognostic Value of the Lung Immune Prognostic Index for Patients Treated for Metastatic Non–Small Cell Lung Cancer. Kazandjian D, Gong Y, Keegan P, et al. JAMA Oncol. 2019;5:1481-1485.
REBLOZYL® Reduces Blood Transfusion Requirements in Patients with Lower-Risk Myelodysplastic Syndromes
SUMMARY: It is estimated that in the United States approximately 13,000 people are diagnosed with MyeloDysplastic Syndromes (MDS) each year. MyeloDysplastic Syndromes are a heterogenous group of stem cell disorders characterized by marrow failure resulting in cytopenias with associated cytogenetic abnormalities, and abnormal cellular maturation with morphologic changes in clonal cells. Majority of the individuals diagnosed with MDS are aged 65 years and older and die as a result of infection and/or bleeding consequent to bone marrow failure. About a third of patients with MDS develop Acute Myeloid Leukemia (AML).
Patients with Lower-risk MDS (Revised IPSS-Very Low, Low, or Intermediate risk ) often present with symptomatic anemia and these patients are in chronic need for RBC transfusions which in turn can result in iron overload and can have a negative impact on quality of life and Overall Survival. These patients are treated with Erythropoiesis Stimulating Agents (ESAs) as first line therapy. ESAs such as Darbepoetin alfa and Epoetin alfa are re-engineered and recombinant DNA technology products of Erythropoietin (EPO), and they stimulate erythropoiesis by binding and activating the EPO receptor. However, transfusion-dependent patients with serum EPO levels above 200 U per liter are less likely to respond to ESAs. Additionally, patients with MDS with ring sideroblasts have a shorter median duration of response to ESAs, than those who do not have ring sideroblasts. Patients with Lower-risk MDS with chromosome 5q deletion (del 5q) who are transfusion dependent are treated with Lenalidomide, regardless of previous treatment with ESAs. In contrast, only 39% of patients with non-del(5q) Lower-risk MDS receive second line therapy besides RBC transfusions, and there are few treatment options for patients who are refractory to, unresponsive to, or ineligible for ESAs. There is therefore an unmet clinical need for safe and effective treatment options, to reduce the RBC transfusion burden in these patients.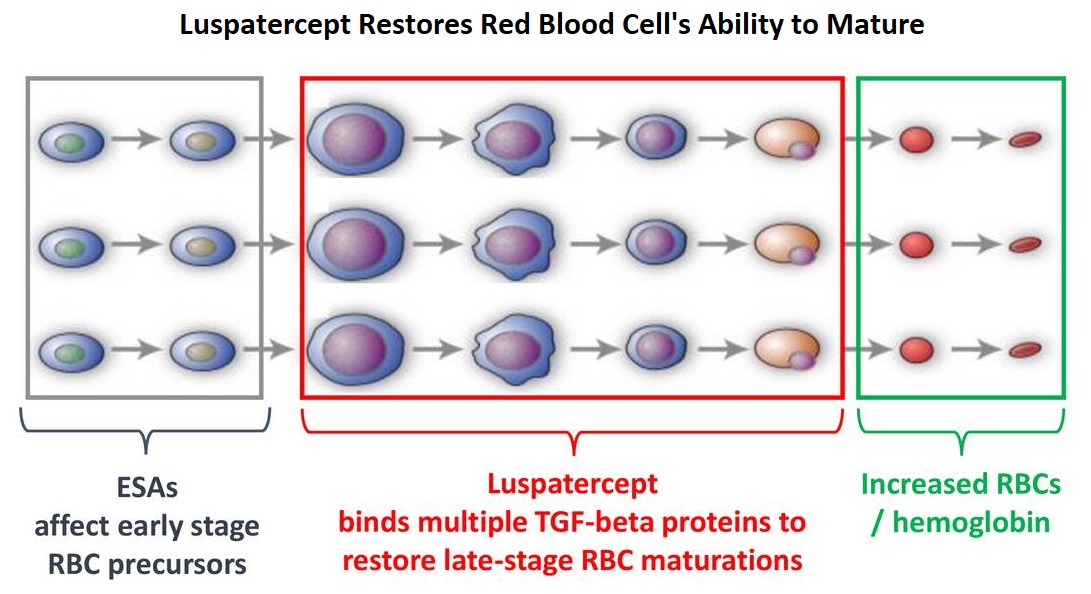
Signaling by the SMAD2 and SMAD3 pathway exerts an inhibitory effect on red cell maturation. This pathway is constitutively activated in the bone marrow cells of patients with MDS and diseases associated with ineffective erythropoiesis such as β-thalassemia. REBLOZYL® (Luspatercept) is a recombinant soluble fusion protein and is first-in-class erythroid maturation agent that enhances erythropoiesis by promoting late-stage Red Blood Cell precursor differentiation and maturation. It targets select Transforming Growth Factor (TGF)-β superfamily ligands such as GDF11, that regulate late-stage erythropoiesis. This results in a reduction in aberrant SMAD2 and SMAD3 signaling, thereby promoting late-stage RBC precursor differentiation and maturation. In a Phase II study, treatment of Lower-risk MDS patients with REBLOZYL® resulted in 38% of patients being transfusion independent for 8 weeks or longer and this benefit was even more so among patients with 15% or more ring sideroblasts.
The MEDALIST trial is a randomized, double-blind, placebo-controlled Phase III study which evaluated the efficacy and safety of REBLOZYL® in patients with anemia secondary to MDS, defined as Very Low-Risk, Low-Risk, or Intermediate-Risk with Ring Sideroblasts, according to the Revised International Prognostic Scoring System (R-IPSS). Eligible patients were refractory, intolerant, or ineligible to receive ESAs and required RBC transfusions. A total of 229 patients (N=229) were randomized 2:1 to receive either REBLOZYL® at a starting dose level of 1mg/kg SC with titration up to 1.75 mg/kg if needed (N=153), or placebo SC (N=76), every 3 weeks for 24 weeks or more. The median age was 71 years and median time from diagnosis was 41.8 months. Approximately 95% of patients had previously received ESAs and 90% had an SF3B1 mutation. The Primary endpoint was RBC transfusion independence for 8 weeks or more between week 1 and 24. A key Secondary endpoint was RBC transfusion independence for 12 weeks or more between week 1 and 24.
Among those receiving REBLOZYL®, 38% achieved the Primary endpoint of RBC transfusion independence for 8 weeks or more, compared with 13% receiving placebo (P<0.001). Further among those receiving REBLOZYL®, 28% achieved the key Secondary endpoint of RBC transfusion independence for 12 weeks or more compared with 8% receiving placebo (P<0.001). The median duration of the longest, single continuous period of response to REBLOZYL® was 30.6 weeks, and 13.6 weeks in the placebo group. Among patients who had a baseline transfusion burden of 4 to less than 6 units per 8 weeks, 37% of those in the REBLOZYL® group and 4% of those in the placebo group had a response. Additionally, patients receiving REBLOZYL® were more likely to achieve an mHI-E (modified Hematologic Improvement-Erythroid) response, (defined as a reduction in transfusion of 4 or more RBC units per 8 weeks or a mean hemoglobin increase of 1.5 g/dL or more per 8 weeks, in the absence of transfusions), compared with patients receiving placebo (53% versus 12% during weeks 1-24; P<0.0001). A mean increase in hemoglobin level of at least 1 g/dL during weeks 1 to 24 was noted in 35% of patients who received REBLOZYL® and in 8% of patients who received placebo. The most common adverse events of any grade associated with REBLOZYL® included fatigue, diarrhea, asthenia, nausea and dizziness, and the incidence of adverse events decreased over time.
It was concluded that treatment with REBLOZYL® significantly reduced the severity of anemia in patients with Lower-risk MDS with ring sideroblasts, who had been RBC transfusion-dependent, and who had disease that was refractory to or unlikely to respond to ESAs. Luspatercept in Patients with Lower-Risk Myelodysplastic Syndromes. Fenaux P, Platzbecker U, Mufti GJ, et al. N Engl J Med 2020; 382:140-151
Neoadjuvant KEYTRUDA® Plus Chemotherapy Improves Pathological Complete Response in Triple Negative Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (13%) will develop invasive breast cancer during their lifetime. Approximately 276,480 new cases of invasive female breast cancer will be diagnosed in 2020 and about 42,170 women will die of the disease.
Triple Negative Breast Cancer (TNBC) is a heterogeneous, molecularly diverse group of breast cancers and are ER (Estrogen Receptor), PR (Progesterone Receptor) and HER2 (Human Epidermal Growth Factor Receptor-2) negative. TNBC accounts for 15-20% of invasive breast cancers, with a higher incidence noted in young patients. It is usually aggressive, and tumors tend to be high grade and patients with TNBC are at a higher risk of both local and distant recurrence. Those with metastatic disease have one of the worst prognoses of all cancers with a median Overall Survival of 13 months. The majority of patients with TNBC who develop metastatic disease do so within the first 3 years after diagnosis, whereas those without recurrence during this period of time have survival rates similar to those with ER-positive breast cancers. The lack of known recurrent oncogenic drivers in patients with metastatic TNBC, presents a major therapeutic challenge. Nonetheless, patients with TNBC often receive chemotherapy in the neoadjuvant, adjuvant or metastatic settings and approximately 30-40% of patients achieve a pathological Complete Response (pCR) in the neoadjuvant setting. In addition to increasing the likelihood of tumor resectability and breast preservation, patients achieving a pCR following neoadjuvant chemotherapy have a longer Event Free Survival (EFS) and Overall Survival (OS). Those who do not achieve a pathological Complete Response tend to have a poor prognosis. For all these reasons, pCR is considered a valid endpoint for clinical testing of neoadjuvant therapy in patients with early stage TNBC. It appears that there are subsets of patients with TNBC who may be inherently insensitive to cytotoxic chemotherapy. Three treatment approaches appear to be promising and they include immune therapies, PARP inhibition and inhibition of PI3K pathway. Previously published studies have shown that presence of tumor-infiltrating lymphocytes was associated with clinical benefit, when treated with chemotherapy and immunotherapy, in patients with TNBC, and improved clinical benefit was observed in patients with immune-enriched molecular subtypes of metastatic TNBC.
KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2. It thereby reverses the PD-1 pathway-mediated inhibition of the immune response and unleashes the tumor-specific effector T cells. Cytotoxic chemotherapy releases tumor-specific antigens and immune checkpoint inhibitors such as KEYTRUDA® when given along with chemotherapy can enhance endogenous anticancer immunity. Preliminary results from Phase I and II trials have shown that in patients with TNBC, KEYTRUDA® given along with chemotherapy in a neoadjuvant setting resulted in a high rate of pCR.
KEYNOTE-522 is an international, placebo controlled Phase III trial, conducted to evaluate the safety and efficacy of neoadjuvant KEYTRUDA® plus chemotherapy followed by adjuvant KEYTRUDA® or placebo, in patients with early stage TNBC. In this study, 1,174 patients were randomly assigned in a 2:1 ratio to receive neoadjuvant KEYTRUDA® 200 mg IV every 3 weeks (N=784) or placebo (N=390). All patients received 4 cycles of Carboplatin plus Paclitaxel, followed by 4 cycles of Doxorubicin or Epirubicin plus Cyclophosphamide, in the neoadjuvant setting. Following definitive surgery, adjuvant KEYTRUDA® or placebo was continued every 3 weeks for 9 cycles or until disease recurrence or unacceptable toxicity. Enrolled TNBC patients were newly diagnosed, treatment naïve, and included both node-negative and node-positive patients with nonmetastatic disease (Tumor Stage T1c, Nodal Stage N1-N2 or Tumor Stage T2-T4, Nodal Stage N0-N2, per AJCC criteria). Treatment groups were well balanced and patients were stratified according to nodal status, tumor size, and Carboplatin schedule (weekly versus every 3 weeks). The two Primary endpoints were pathological Complete Response (pCR) at the time of definitive surgery and Event Free Survival (EFS). The median follow up was 15.5 months.
At the first interim analysis, the pCR among the first 602 patients who underwent randomization was 64.8% in the KEYTRUDA® plus chemotherapy group, compared with 51.2% in the placebo plus chemotherapy group (P<0.001). This pCR benefit was consistent across subgroups including PD-L1 expresssion subgroups. In the PD-L1-positive population, the pCR was 68.9% in the KEYTRUDA® plus chemotherapy group compared with 54.9% in the placebo plus chemotherapy group. In the PD-L1 negative group, the pCR in the KEYTRUDA® plus chemotherapy group was 45.3% and 30.3% in the placebo plus chemotherapy group. Neoadjuvant KEYTRUDA® plus chemotherapy followed by adjuvant KEYTRUDA® showed a favorable trend for Event Free Survival compared with chemotherapy alone, although these data are still premature. Across all treatment phases, Grade 3 or higher treatment-related toxicities were 78.0% in the KEYTRUDA® plus chemotherapy group and 73.0% in the placebo plus chemotherapy group.
It was concluded that among patients with early stage Triple Negative Breast Cancer, the addition of KEYTRUDA® to neoadjuvant chemotherapy significantly increased the pathological Complete Response rate, compared to those who received placebo plus neoadjuvant chemotherapy, with a favorable trend in Event Free Survival. Pembrolizumab for Early Triple-Negative Breast Cancer. Schmid P, Cortés J, Pusztai L, et al. for the KEYNOTE-522 Investigators. N Engl J Med 2020;382:810-821