
The FDA on March 30, 2020 approved IMFINZI® in combination with Etoposide and either Carboplatin or Cisplatin as first-line treatment of patients with Extensive-Stage Small Cell Lung Cancer (ES-SCLC). IMFINZI® is a product of AstraZeneca.
Author: RR
OPDIVO® and YERVOY®
The FDA on March 10, 2020 granted accelerated approval to the combination of OPDIVO® (Nivolumab) and YERVOY® (Ipilimumab) for patients with Hepatocellular Carcinoma (HCC), who have been previously treated with NEXAVAR® (Sorafenib). Both OPDIVO® and YERVOY® are products of Bristol-Myers Squibb Co.
NERLYNX® (Neratinib)
The FDA on February 25, 2020 approved NERLYNX® in combination with XELODA® (Capecitabine) for adult patients with advanced or metastatic HER2-positive Breast Cancer, who have received two or more prior anti-HER2 based regimens in the metastatic setting. NERLYNX® is a product of Puma Biotechnology, Inc.
SARCLISA® (Isatuximab-irfc)
The FDA on March 2, 2020 approved SARCLISA® in combination with POMALYST® (Pomalidomide) and Dexamethasone for adult patients with Multiple Myeloma, who have received at least two prior therapies including REVLIMID® (Lenalidomide) and a Proteasome Inhibitor. SARCLISA® is a product of Sanofi-Aventis U.S. LLC.
TAZVERIK® (Tazemetostat)
The FDA on January 23, 2020 granted accelerated approval to TAZVERIK® for adults and pediatric patients aged 16 years and older with metastatic or locally advanced epithelioid sarcoma, not eligible for complete resection. TAZVERIK® is a product of Epizyme, Inc.
AYVAKIT® (Avapritinib)
The FDA on January 9, 2020 approved AYVAKIT® for adults with unresectable or metastatic GastroIntestinal Stromal Tumor (GIST) harboring a Platelet-Derived Growth Factor Receptor Alpha (PDGFRA) exon 18 mutation, including D842V mutations. AYVAKIT® is a product of Blueprint Medicines Corporation.
KEYTRUDA® (Pembrolizumab)
he FDA on January 8, 2020 approved KEYTRUDA® for the treatment of patients with Bacillus Calmette-Guerin (BCG)-unresponsive, high-risk, Non-Muscle Invasive Bladder Cancer (NMIBC) with Carcinoma In Situ (CIS), with or without papillary tumors, who are ineligible for or have elected not to undergo cystectomy. KEYTRUDA® is a product of Merck & Co. Inc.
ENHERTU® Highly Effective in Heavily Pretreated HER2-Positive Advanced Breast Cancer
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (13%) will develop invasive breast cancer during their lifetime. Approximately 276,480 new cases of invasive female breast cancer will be diagnosed in 2020 and about 42,170 women will die of the disease. The HER or erbB family of receptors consist of HER1, HER2, HER3 and HER4. Approximately 15-20% of invasive breast cancers overexpress HER2/neu oncogene, which is a negative predictor of outcomes without systemic therapy. Patients with HER2-positive metastatic breast cancer are often treated with anti-HER2 targeted therapy along with chemotherapy, irrespective of hormone receptor status, and this has resulted in significantly improved treatment outcomes. HER2-targeted therapies include HERCEPTIN® (Trastuzumab), TYKERB® (Lapatinib), PERJETA® (Pertuzumab) and KADCYLA® (ado-Trastuzumab emtansine). Dual HER2 blockade with HERCEPTIN® and PERJETA®, given along with chemotherapy (with or without endocrine therapy), as first line treatment, in HER2 positive metastatic breast cancer patients, was shown to significantly improve Progression Free Survival (PFS) as well as Overall Survival (OS). The superior benefit with dual HER2 blockade has been attributed to differing mechanisms of action and synergistic interaction between HER2 targeted therapies. Patients progressing on Dual HER2 blockade often receive KADCYLA® which results in an Objective Response Rate (ORR) of 44% and a median PFS of 9.6 months, when administered after HERCEPTIN® and a taxane. There is however no standard treatment option for this patient population following progression on KADCYLA®.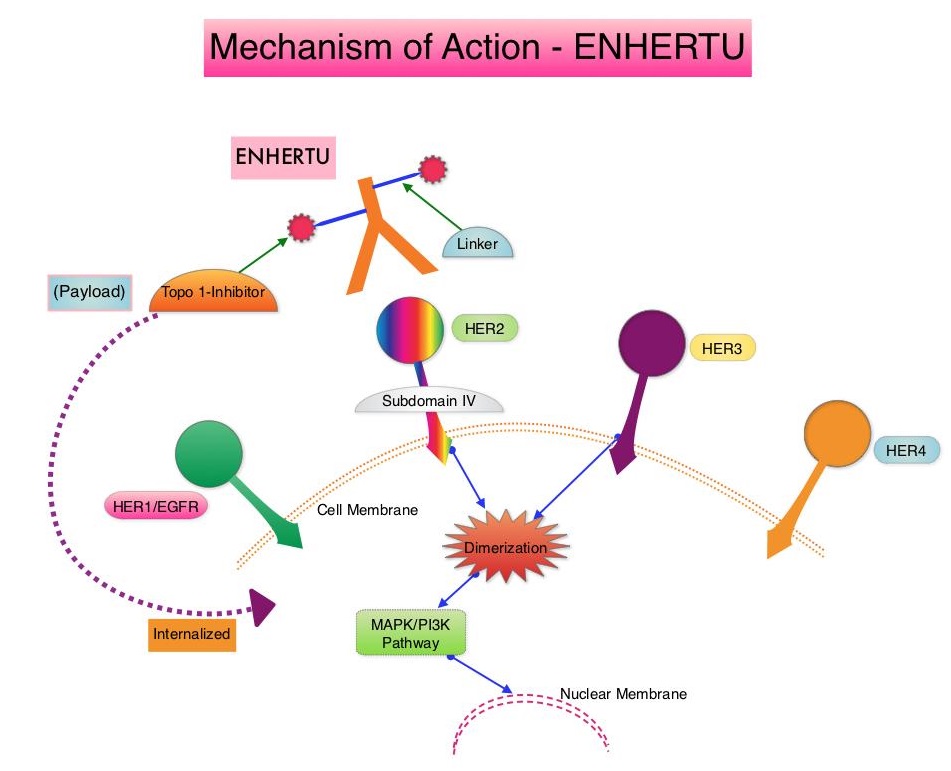
ENHERTU® (Trastuzumab Deruxtecan) is an Antibody-Drug Conjugate (ADC) composed of a humanized monoclonal antibody specifically targeting HER2, with the amino acid sequence similar to Trastuzumab, a cleavable tetrapeptide-based linker, and a potent cytotoxic Topoisomerase I inhibitor as the cytotoxic drug (payload). ENHERTU® has a favorable pharmacokinetic profile and the tetrapeptide-based linker is stable in the plasma and is selectively cleaved by cathepsins that are up-regulated in tumor cells. Unlike KADCYLA®, ENHERTU® has a higher drug-to-antibody ratio (8 versus 4), released payload easily crosses the cell membrane with resulting potent cytotoxic effect on neighboring tumor cells regardless of target expression, and the released cytotoxic agent (payload) has a short half-life, minimizing systemic exposure. In a Phase 1 dose-finding study involving patients with advanced HER2-positive breast cancer, treatment with ENHERTU® resulted in a confirmed response rate was 59.5%, and the median response duration was 20.7 months. However, the efficacy of ENHERTU® in patients with HER2-positive metastatic breast cancer, previously treated with KADCYLA® remained unclear.
DESTINY-Breast 01 study is a multicenter, single-arm, Phase II registration trial, in which 184 patients with HER2-positive, metastatic breast cancer, who had received two or more prior HER2 targeted therapies including KADCYLA®, were enrolled. Patients received ENHERTU® 5.4 mg/kg IV every 3 weeks until disease progression or unacceptable toxicity. The median age was 55 years, 53% had Hormone Receptor-positive tumors and the median number of previous lines of therapy for metastatic disease was SIX and included KADCYLA® (100%), Trastuzumab (100%), Pertuzumab (66%), and other anti-HER2 therapies (54%). The Primary end point was Objective Response Rate (ORR) assessed by Independent Central Review and Secondary endpoints included Duration of Response, Progression Free Survival (PFS) and Overall Survival (OS). The median follow up was 11.1 months.
The ORR was 60.9%, with 6% Complete Responses and 54.9% Partial Responses. The median time to response was 1.6 months and the median response duration was 14.8 months. The median PFS was 16.4 months the median OS was not reached at the time of this publication. The efficacy results were consistent across all key subgroups, including patients who had received previous PERJETA® (Pertuzumab) therapy. The most Grade 3 or higher adverse events were cytopenias, nausea, diarrhea and Interstitial Lung Disease.
It was concluded that ENHERTU® has a high level of clinical efficacy with a durable antitumor activity in a heavily pretreated patient population with HER2-positive metastatic breast cancer. The FDA in December 2019, granted accelerated approval to ENHERTU® (Trastuzumab deruxtecan) for patients with unresectable or metastatic HER2-positive breast cancer, who have received two or more prior anti-HER2-based regimens in the metastatic setting. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast Cancer. Modi S, Saura C, Yamashita T, et al. for the DESTINY-Breast01 Investigators. N Engl J Med 2020;382:610-621.
Bone-Targeting Radioisotope, XOFIGO® Improves Overall Survival in CRPC Patients with Bone Metastases
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer, and 1 in 9 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, about 191,930 new cases of prostate cancer will be diagnosed in 2020 and 33,330 men will die of the disease. The skeletal system is the most common site for distant metastases among patients with prostate cancer and over 90% of patients with advanced prostate cancer develop bone metastases, which are osteoblastic (or sclerotic), characterized by deposition of new bone. Bone scan is the most common and cost effective modality for the diagnosis of bone metastases and Technetium (Tc) 99m-labeled methylene diphosphonate is the most widely used bone scanning agent. Agents such as ZOMETA® (Zoledronic acid) and XGEVA® (Denosumab) can prevent or delay Skeletal Related Events (SRE’s) and External Beam Radiation Therapy (EBRT) is often utilized to treat symptomatic SRE’s. EBRT can however damage the bone marrow in the radiated field, resulting in cytopenias, and consequently can potentially preclude patients from receiving cytotoxic chemotherapy.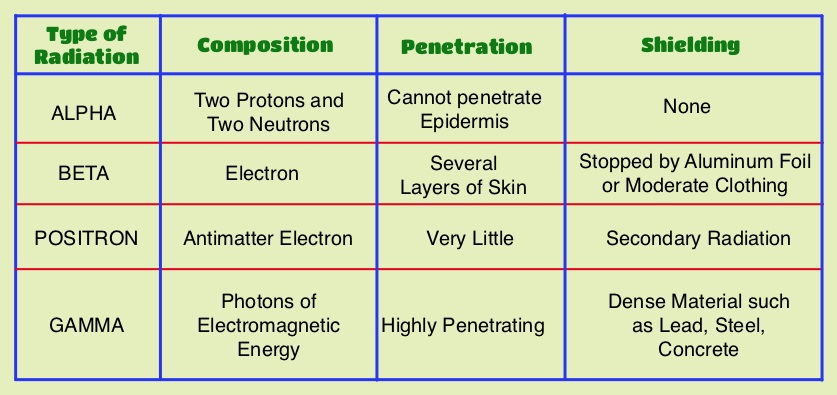
Radium Ra 223 dichloride (XOFIGO®) is a bone seeking alpha particle emitter and by virtue of its chemical similarity to calcium is preferentially taken up by the bone and forms complexes with bone mineral, hydroxyapatite, in areas where there is increased bone turnover, such as bone metastases. XOFIGO® induces double stranded DNA breaks resulting in antitumor effects and has a very short range in tissues (around 2 and 10 cells), quickly losing energy, compared to beta or gamma radiation. The end result is less damage to the adjacent healthy tissues. Further, unlike Ra-226 which was first isolated by Madame Curie, XOFIGO® has a short half life of 11.4 days and rapidly decays, preventing significant radiation exposure.
Strontium-89 (METASTRON®) is a pure beta emitter and imitates the bio-distribution of calcium in vivo, and is avidly taken up into bony metastases where it has a biological half-life of about 50 days. The biological half-life in the normal bone is approximately 14 days. METASTRON® in two Phase III studies significantly reduced the appearance of new painful metastases, analgesic requirements, and serum PSA levels, compared with radiotherapy alone, among patients with metastatic prostate cancer, suggesting that METASTRON® is an effective systemic radiopharmaceutical for the palliation of bony metastases.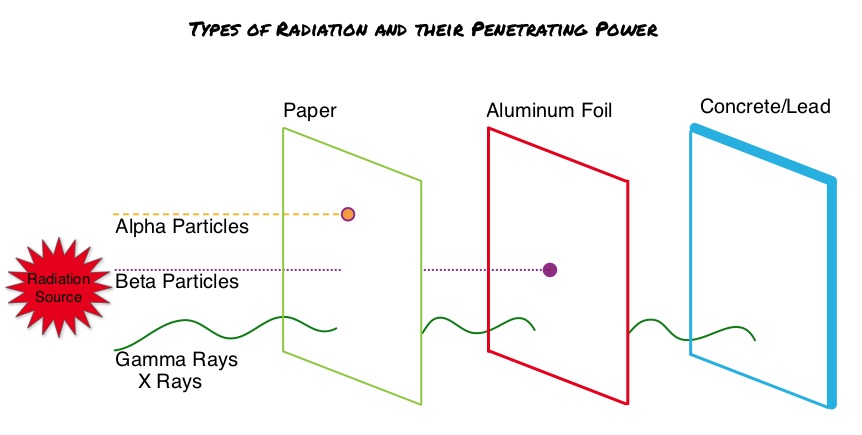
In this publication, the authors assessed the Overall Survival (OS) benefit of both alpha emitting and beta emitting bone-targeted RadioIsotopes (RIs) in men with bone metastases from CRPC (Castrate Resistant Prostate Cancer), treated with bone-targeted RIs, and further compared the effects of alpha emitting RIs with beta emitting RIs. This meta-analysis included Individual Patient Data of 2081 patients with CRPC and bone metastases from 6 randomized clinical trials, conducted between January 1993 and June 2013, and data was collected via PubMed, Cochrane Library, ClinicalTrials.gov, and meeting proceedings. Patients included in this study had histologically proven diagnosis of prostate cancer and disease progression after both, surgical or chemical castration, and have evidence of bone metastasis. The median age of patients was 70 years and the proportion of patients with more than 6 bone metastases ranged from 67% to 86%. The median follow up was 26.7 months. The Primary end point of the study was Overall Survival (OS), and Secondary end points included Symptomatic Skeletal Event (SSE)-Free Survival and adverse events.
This analysis showed that an alpha emitting bone- targeted RI (XOFIGO®) was associated with a significantly higher Overall Survival and higher symptomatic Skeletal Event-Free Survival, whereas a beta emitting RI (METASTRON®) was not associated with these significant outcomes. Treatment with the alpha emitter (XOFIGO®) was associated with a significant 30% decreased risk of death when compared with no radioisotope use, whereas use of the beta emitter (METASTRON®) did not confer a significant survival benefit. Further, treatment with XOFIGO® was associated with a significant 35% decreased risk of symptomatic Skeletal Event-Free Survival, whereas treatment with METASTRON® was not associated with such benefit. In the subgroup analyses, men with the lowest serum PSA values appeared to benefit significantly more with the use of bone-targeted RI therapy compared with those with the highest serum PSA values. Hematological toxicities were more frequently observed in patients treated by RI compared with those treated without RI, and the type of radiation did not result in significant differences.
It was concluded from this meta-analysis that among patients with metastatic CRPC, a significant improvement of Overall Survival and symptomatic Skeletal Event-Free Survival was noted with bone-targeted alpha emitting bone- targeted RI (XOFIGO®), but not beta emitting RIs (METASTRON®). Overall Survival in Men With Bone Metastases From Castration-Resistant Prostate Cancer Treated With Bone-Targeting Radioisotopes: A Meta-analysis of Individual Patient Data From Randomized Clinical Trials. Terrisse S, Karamouza E, Parker CC, et al. for the MORPHEP Collaborative Group. JAMA Oncol. 2020;6:206-216
Antibiotic Use Significantly Decreases Efficacy of Checkpoint Inhibitors in Patients with Advanced Cancer
SUMMARY: The American Cancer Society estimates that in 2020, there will be an estimated 1.8 million new cancer cases diagnosed and 606,520 cancer deaths in the United States. Immunotherapy with Immune Checkpoint Inhibitors (ICIs) has revolutionized cancer care and has become one of the most effective treatment options by improving Overall Response Rate and prolongation of survival across multiple tumor types. These agents target Programmed cell Death protein-1 (PD-1), Programmed cell Death Ligand-1 (PD-L1), Cytotoxic T-Lymphocyte-Associated protein-4 (CTLA-4), and many other important regulators of the immune system. Biomarkers predicting responses to ICI’s include Tumor Mutational Burden (TMB), Mismatch Repair (MMR) status, and Programmed cell Death Ligand 1 (PD‐L1) expression. Other biomarkers such as Tumor Infiltrating Lymphocytes (TILs), TIL‐derived Interferon‐γ, Neutrophil‐to‐Lymphocyte ratio, and peripheral cytokines, have also been proposed as predictors of response. It has been postulated that concomitant medications during therapy with ICIs such as baseline steroid use as well as treatment with antibiotics may negate or lessen the efficacy of ICIs.
Preclinical studies have suggested that immune-based therapies for cancer may have a very complex interplay with the host’s microbiome and there may be a relationship between gut bacteria and immune response to cancer. The crosstalk between microbiota in the gut and the immune system allows for the tolerance of commensal bacteria (normal microflora) and oral food antigens and at the same time enables the immune system to recognize and attack opportunistic bacteria. Immune Checkpoint Inhibitors strongly rely on the influence of the host’s microbiome, and the gut microbial diversity enhances mucosal immunity, dendritic cell function, and antigen presentation. Broad-spectrum antibiotics can potentially alter the bacterial composition and diversity of our gut microbiota, by killing the good bacteria. It has been postulated that this may negate the benefits of immunotherapy and influence treatment outcomes.
This present study was conducted to assess the impact of antibiotic use at the time of ICI treatment, on the outcomes for patients with advanced or metastatic solid tumors. This United Kingdom single institution retrospective analysis included 291 (N=291) patients with advanced cancer, treated with ICI (Melanoma N=179, Non‐Small Cell Lung Cancer N=64, and Renal Cell Carcinoma N=48), who received an ICI agent between January 1, 2015, and April 1, 2017. Antibiotic use (both single and multiple courses as well as prolonged use) during the periods 2 weeks before and 6 weeks after ICI treatment was investigated and data collected. The authors chose this time period, because the potential duration of modification of gut microbiota following antibiotic therapy can vary, for different classes of antibiotics.
Ninety two (N=92) patients in the analyzed cohort had antibiotic therapy during ICI treatment. The use of antibiotics during treatment with ICIs was significantly associated with shorter Progression Free Survival (median PFS 3.1 versus 6.3 months; P=0.003) and Overall Survival (median OS 10.4 versus 21.7 months; P=0.002). Administration of a single course of antibiotics was associated with a non-significant reduction in PFS and OS, whereas patients who had received cumulative courses of antibiotics had significantly worse PFS (median PFS, 2.8 months; P=0.026) and OS (median OS, 6.3 months; P=0.009). Cumulative use of antibiotics was an independent significant prognostic factor for clinical outcomes among patients treated with ICIs.
It was concluded from this large, multivariate analysis that antibiotic use is an independent negative predictor of PFS and OS in patients with advanced cancer treated with Immune Checkpoint Inhibitors, with worse treatment outcomes among patients who had received multiple or prolonged courses of antibiotics. The authors added that this is the first study to suggest an adverse effect of cumulative antibiotic use, in patients receiving treatment with Immune Checkpoint Inhibitors for advanced cancer. Cumulative Antibiotic Use Significantly Decreases Efficacy of Checkpoint Inhibitors in Patients with Advanced Cancer. Tinsley N, Zhou C, Tan G, et al. Oncologist. 2020;25:55-63.