
KADCYLA® (Ado-Trastuzumab Emtansine, T-DM1) is an antibody-drug conjugate (ADC) comprised of the antibody HERCEPTIN® (Trastuzumab) and a chemotherapy agent Emtansine, linked together. Upon binding to the HER2 receptor, KADCYLA® not only inhibits the HER2 signaling pathways but also delivers Emtansine, a microtubule inhibitor, directly inside the tumor cells and destroys them. In the TH3RESA trial, treatment with KADCYLA® significantly improved Progression Free Survival compared to physicians choice, for those patients who had previously received HERCEPTIN® and TYKERB® (Lapatinib) and this therefore makes KADCYLA® the treatment of choice, for this patient population.
Category: Hem/Onc Updates
Results of a prospective, randomized, open-label phase 3 study of ruxolitinib (RUX) in polycythemia vera (PV) patients resistant to or intolerant of hydroxyurea (HU) the RESPONSE trial
SUMMARY: Polycythemia Vera (P. Vera) is a clonal myeloproliferative neoplasm characterized by isolated Erythrocytosis in a majority of the patients, with the remaining demonstrating Erythrocytosis, Leukocytosis and/or Thrombocytosis along with Erythrocytosis. Patients usually present with this disorder in their sixth decade and are often asymptomatic, with the diagnosis made incidentally on routine laboratory evaluation. About 30% of the patients however, may initially present with a thrombotic episode, whereas a small percentage of patients may present with disease related symptoms such as pruritus and fatigue.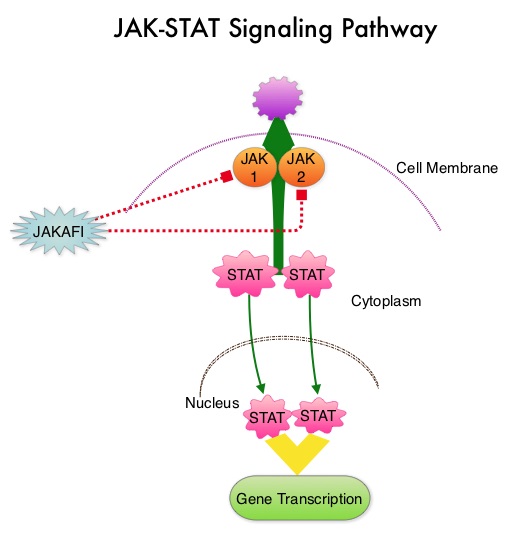 Over activation of the JAK-STAT signal transduction pathway caused by V617F mutation, has been implicated in majority of the patients with P. Vera. This pathway normally is responsible for passing information from outside the cell through the cell membrane to the DNA in the nucleus for gene transcription. Janus Kinase (JAK) family of tyrosine kinases are cytoplasmic proteins and include JAK1, JAK2, JAK3 and TYK2. JAK1 helps propagate the signaling of inflammatory cytokines whereas JAK2 is essential for growth and differentiation of hematopoietic stem cells. These tyrosine kinases mediate cell signaling by recruiting STAT’s (Signal Transducer and Activator of Transcription), with resulting modulation of gene expression. In patients with P. Vera, the aberrant myeloproliferation is the result of dysregulated JAK2-STAT signaling as well as excess production of inflammatory cytokines associated with this abnormal signaling. JAK2 mutations such as JAK2 V617F are seen in approximately 95% of patients with P. Vera. The goals of therapy in P. Vera are to maintain the hematocrit at less than 45% and decrease the risk of thrombosis and bleeding. P. Vera is presently managed with periodic phlebotomies, cytoreductive therapy with oral antimetabolite, Hydroxyurea and antiplatelet agents such as low dose aspirin. However, a significant number of patients on these therapies become intolerant or resistant to these treatments, leading to an increased risk of progression. JAKAFI® is a potent JAK1 and JAK2 inhibitor and exerts its mechanism of action by targeting and inhibiting the dysregulated JAK2-STAT signaling pathway.
Over activation of the JAK-STAT signal transduction pathway caused by V617F mutation, has been implicated in majority of the patients with P. Vera. This pathway normally is responsible for passing information from outside the cell through the cell membrane to the DNA in the nucleus for gene transcription. Janus Kinase (JAK) family of tyrosine kinases are cytoplasmic proteins and include JAK1, JAK2, JAK3 and TYK2. JAK1 helps propagate the signaling of inflammatory cytokines whereas JAK2 is essential for growth and differentiation of hematopoietic stem cells. These tyrosine kinases mediate cell signaling by recruiting STAT’s (Signal Transducer and Activator of Transcription), with resulting modulation of gene expression. In patients with P. Vera, the aberrant myeloproliferation is the result of dysregulated JAK2-STAT signaling as well as excess production of inflammatory cytokines associated with this abnormal signaling. JAK2 mutations such as JAK2 V617F are seen in approximately 95% of patients with P. Vera. The goals of therapy in P. Vera are to maintain the hematocrit at less than 45% and decrease the risk of thrombosis and bleeding. P. Vera is presently managed with periodic phlebotomies, cytoreductive therapy with oral antimetabolite, Hydroxyurea and antiplatelet agents such as low dose aspirin. However, a significant number of patients on these therapies become intolerant or resistant to these treatments, leading to an increased risk of progression. JAKAFI® is a potent JAK1 and JAK2 inhibitor and exerts its mechanism of action by targeting and inhibiting the dysregulated JAK2-STAT signaling pathway. 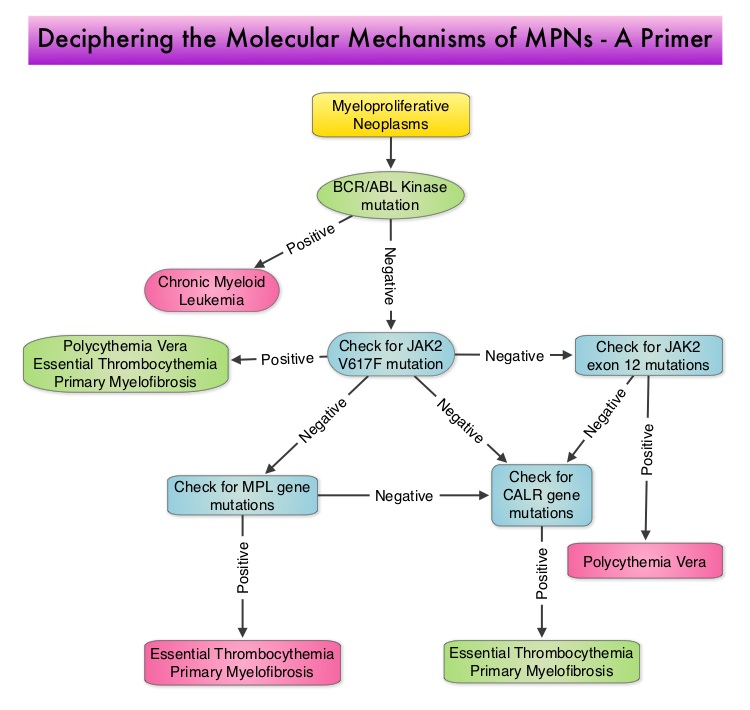 The RESPONSE trial is a phase III prospective randomized study in which patients with P. Vera, who were refractory or intolerant of Hydroxyurea were randomized to receive JAKAFI® 10 mg PO, bid (N=110) or Best Available Therapy (BAT), which consisted of investigator choice of monotherapy or observation only (N=112). Eligible patients were phlebotomy dependent patients with splenomegaly (> 450 cubic cm). Patients receiving BAT were allowed to cross over to JAKAFI® group from week 32 onwards. The primary endpoint of this study (composite primary endpoint) was the proportion of patients whose hematocrit was controlled without phlebotomy and whose spleen volume was reduced by 35% or more from baseline, as assessed by MRI imaging at 32 weeks. Secondary endpoints included durable response, Complete Hematological Remission and safety. The primary analysis was conducted when all patients reached week 48 or discontinued therapy. The proportion of patients in the JAKAFI® group who achieved the composite primary endpoint was 21% compared to 1% in the BAT group (P < 0.0001). Seventy seven percent (77%) of the patients in the JAKAFI® group achieved at least one of the two major components of the composite primary endpoint. Put another way, 60% of the patients in the JAKAFI® arm were able to achieve the target hematocrit level in the absence of phlebotomy, compared to 20% in the BAT group. Reduction in the spleen volume by 35% or more was noted in 38% of the patients in the JAKAFI® group compared to 1% in the BAT group. Complete Hematological Remission defined as continuous hematocrit below 45%, as well as normal white blood cells and platelets counts, was achieved in 24% and 9% of patients in JAKAFI® and BAT group respectively (P=0.003). More patients assigned to JAKAFI® group also demonstrated 50% or more improvement in the Myeloproliferative Neoplasm Symptom Assessment Form (MPN-SAF) 14-item total symptom score, at week 32 compared to BAT (49% vs 5%). Thromboembolic events occurred in one patient assigned to the JAKAFI® group as compared to six patients in the BAT group. The authors concluded that JAKAFI® may represent a new option for treating high risk patients with Polycythemia Vera, who are refractory or intolerant of Hydroxyurea. Jakafi® is superior to Best Available Therapy (BAT) in controlling hematocrit without phlebotomies as well as Splenic Volume. Further, JAKAFI® is also effective in improving P. Vera associated symptoms. Verstovsek S, Kiladjian J, Griesshammer M, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7026)
The RESPONSE trial is a phase III prospective randomized study in which patients with P. Vera, who were refractory or intolerant of Hydroxyurea were randomized to receive JAKAFI® 10 mg PO, bid (N=110) or Best Available Therapy (BAT), which consisted of investigator choice of monotherapy or observation only (N=112). Eligible patients were phlebotomy dependent patients with splenomegaly (> 450 cubic cm). Patients receiving BAT were allowed to cross over to JAKAFI® group from week 32 onwards. The primary endpoint of this study (composite primary endpoint) was the proportion of patients whose hematocrit was controlled without phlebotomy and whose spleen volume was reduced by 35% or more from baseline, as assessed by MRI imaging at 32 weeks. Secondary endpoints included durable response, Complete Hematological Remission and safety. The primary analysis was conducted when all patients reached week 48 or discontinued therapy. The proportion of patients in the JAKAFI® group who achieved the composite primary endpoint was 21% compared to 1% in the BAT group (P < 0.0001). Seventy seven percent (77%) of the patients in the JAKAFI® group achieved at least one of the two major components of the composite primary endpoint. Put another way, 60% of the patients in the JAKAFI® arm were able to achieve the target hematocrit level in the absence of phlebotomy, compared to 20% in the BAT group. Reduction in the spleen volume by 35% or more was noted in 38% of the patients in the JAKAFI® group compared to 1% in the BAT group. Complete Hematological Remission defined as continuous hematocrit below 45%, as well as normal white blood cells and platelets counts, was achieved in 24% and 9% of patients in JAKAFI® and BAT group respectively (P=0.003). More patients assigned to JAKAFI® group also demonstrated 50% or more improvement in the Myeloproliferative Neoplasm Symptom Assessment Form (MPN-SAF) 14-item total symptom score, at week 32 compared to BAT (49% vs 5%). Thromboembolic events occurred in one patient assigned to the JAKAFI® group as compared to six patients in the BAT group. The authors concluded that JAKAFI® may represent a new option for treating high risk patients with Polycythemia Vera, who are refractory or intolerant of Hydroxyurea. Jakafi® is superior to Best Available Therapy (BAT) in controlling hematocrit without phlebotomies as well as Splenic Volume. Further, JAKAFI® is also effective in improving P. Vera associated symptoms. Verstovsek S, Kiladjian J, Griesshammer M, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7026)
NCCN Guidelines for Survivorship Expanded to Address Two Common Conditions
SUMMARY: The National Comprehensive Cancer Network (NCCN) has expanded its Survivorship Guidelines to include cancer-associated cognitive impairment and Chemotherapy Induced Peripheral Neuropathy. The later is a component of the Adult Cancer Pain section. Dr. Urba discussed the management of Chemotherapy Induced Peripheral Neuropathy at the NCCN 19th annual conference. Approximately 20%-40% of the patients suffer from Chemotherapy Induced Peripheral Neuropathy, which can result in premature discontinuation of treatment. Further, this adverse event in a significant number of patients can persist indefinitely and can be disabling, thus impacting their activities of daily living.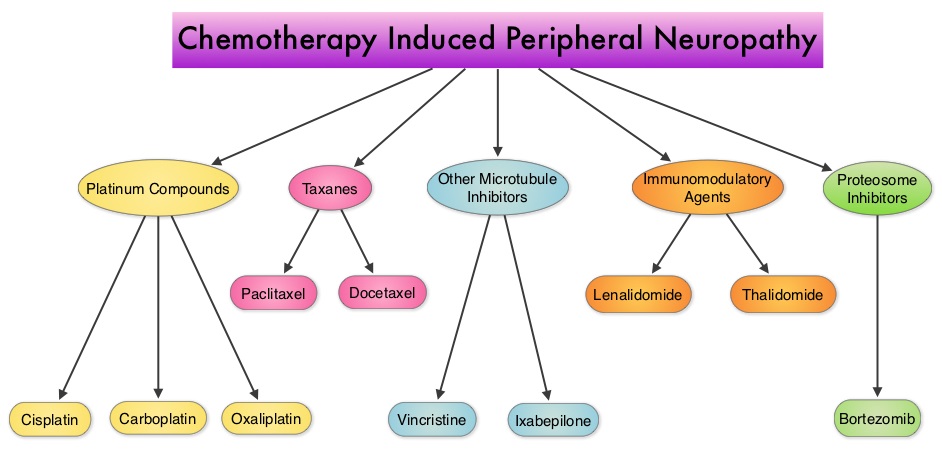 The following chemotherapeutic agents are associated with varying degrees of peripheral neuropathy – Platinum compounds (Cisplatin, Carboplatin and Oxaliplatin), Taxanes (Paclitaxel, Docetaxel), Immunomodulatory agents (Thalidomide, Lenalidomide), Other Microtubule inhibitors (Vincristine, Ixabepilone) and Proteosome Inhibitors (Bortezomib). It may be necessary to screen and rescreen patients for neuropathic pain, as patients may not be forthcoming with this complaint. Management of Neuropathic pain may include systemic treatment with adjuvant analgesics, topical therapies and psychosocial support. The management of Chemotherapy Induced Peripheral Neuropathy has mostly been extrapolated from validated studies on diabetic neuropathy. The first line treatment for Chemotherapy Induced Neuropathic Pain includes antidepressants and anticonvulsants, which if not effective on their own, can be combined with opioids. TriCyclic Antidepressants (TCA’s) such as Amitriptyline and Nortriptyline (PAMELOR®) can be considered as first line choice for appropriate patients, although its mechanism of action is uncertain and 20% of the patients discontinue therapy because of adverse effects.
The following chemotherapeutic agents are associated with varying degrees of peripheral neuropathy – Platinum compounds (Cisplatin, Carboplatin and Oxaliplatin), Taxanes (Paclitaxel, Docetaxel), Immunomodulatory agents (Thalidomide, Lenalidomide), Other Microtubule inhibitors (Vincristine, Ixabepilone) and Proteosome Inhibitors (Bortezomib). It may be necessary to screen and rescreen patients for neuropathic pain, as patients may not be forthcoming with this complaint. Management of Neuropathic pain may include systemic treatment with adjuvant analgesics, topical therapies and psychosocial support. The management of Chemotherapy Induced Peripheral Neuropathy has mostly been extrapolated from validated studies on diabetic neuropathy. The first line treatment for Chemotherapy Induced Neuropathic Pain includes antidepressants and anticonvulsants, which if not effective on their own, can be combined with opioids. TriCyclic Antidepressants (TCA’s) such as Amitriptyline and Nortriptyline (PAMELOR®) can be considered as first line choice for appropriate patients, although its mechanism of action is uncertain and 20% of the patients discontinue therapy because of adverse effects.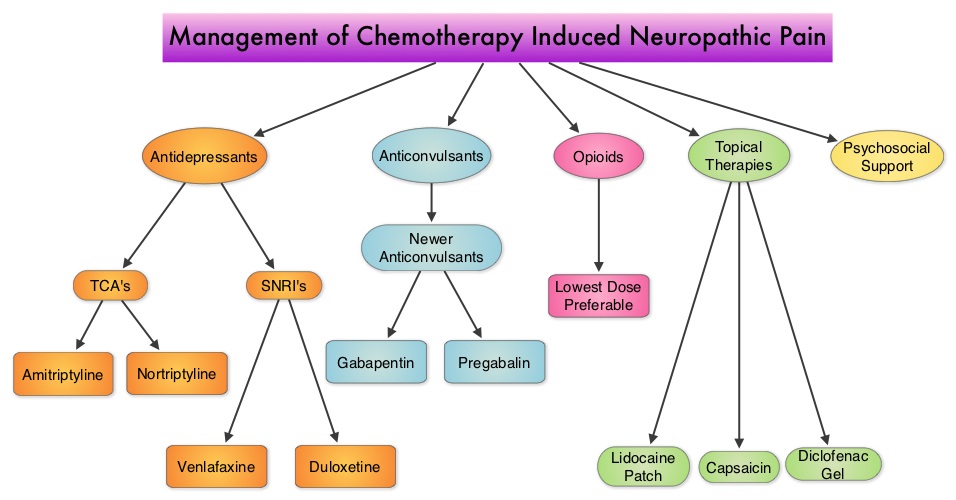 Patients may be able to better tolerate these agents if started at a lower dose and dose titrated slowly every three to five days. Peripheral neuropathic pain has been attributed to an unbalanced release of norepinephrine and serotonin from the neurons. Serotonin-Norepinephrine Reuptake Inhibitors (SNRI’s), including Venlafaxine (EFFEXOR®) and Duloxetine (CYMBALTA®), are better tolerated and have fewer drug interactions than TCA’s. EFFEXOR® in one study significantly relieved Oxaliplatin induced neuropathic pain in more than two thirds of the patients when compared to placebo and a third of the patients had complete pain relief. There is however limited evidence showing a beneficial role of Selective Serotonin Reuptake Inhibitors (SSRI’s) such as Citalopram (CELEXA®) and Paroxetine (PAXIL®) for neuropathic pain. As a note of caution, SNRI’s such as EFFEXOR® and CYMBALTA®, can interact with Tamoxifen, prescribed to patients with breast cancer, preventing Tamoxifen from converting to its active form. The dose of antidepressants needed to alleviate neuropathic pain is not dependent on antidepressant activity and may be lower than that recommended for treatment of depression. The newer anticonvulsants such as Gabapentin (NEURONTIN®), Pregabalin (LYRICA®) are preferable first line agents for the treatment of neuropathic pain rather than traditional, older agents such as Carbamazepine (TEGRETOL®), Phenytoin (DILANTIN®) and Valproate (DEPAKOTE®), as the newer agents are associated with fewer drug interactions. The newer agents bind to the alpha2-delta subunit of the calcium-sensitive channels, modulating neurotransmitter release. Of the newer agents, NEURONTIN® (Gabapentin) is not protein bound and is excreted unchanged in the urine and therefore has fewer drug interactions. If opioids are a consideration for neuropathic pain relief, the lowest dose is recommended. Topical therapies for neuropathic pain have the advantage of controlling pain without systemic side effects. It therefore can be combined with systemic treatment. Lidocaine 5% patches (LIDODERM®) block neuronal sodium channels whereas Capsaicin cream (ZOSTRIX®) stimulates the C fibers to release and subsequently deplete substance P, there by blocking pain signaling to the brain. Diclofenac gel 1% when applied once a day, concentrates in the dermis and has less gastrointestinal side effects and may be beneficial for neuropathic pain. A combination of Ketamine 1% and Amitriptyline 2% cream applied topically has also been promising in a small study. Patients experiencing refractory pain may benefit with the use of Transcutaneous Electrical Nerve Stimulation (TENS), although referral to the pain clinic may be appropriate. Psychosocial support utilizing a team of specialists and social workers/counsellors, should be an integral part of pain management. Kvale E and Urba SG. National Comprehensive Cancer Network (NCCN) 19th Annual Conference, March 13 – 15, 2014; Hollywood, Florida
Patients may be able to better tolerate these agents if started at a lower dose and dose titrated slowly every three to five days. Peripheral neuropathic pain has been attributed to an unbalanced release of norepinephrine and serotonin from the neurons. Serotonin-Norepinephrine Reuptake Inhibitors (SNRI’s), including Venlafaxine (EFFEXOR®) and Duloxetine (CYMBALTA®), are better tolerated and have fewer drug interactions than TCA’s. EFFEXOR® in one study significantly relieved Oxaliplatin induced neuropathic pain in more than two thirds of the patients when compared to placebo and a third of the patients had complete pain relief. There is however limited evidence showing a beneficial role of Selective Serotonin Reuptake Inhibitors (SSRI’s) such as Citalopram (CELEXA®) and Paroxetine (PAXIL®) for neuropathic pain. As a note of caution, SNRI’s such as EFFEXOR® and CYMBALTA®, can interact with Tamoxifen, prescribed to patients with breast cancer, preventing Tamoxifen from converting to its active form. The dose of antidepressants needed to alleviate neuropathic pain is not dependent on antidepressant activity and may be lower than that recommended for treatment of depression. The newer anticonvulsants such as Gabapentin (NEURONTIN®), Pregabalin (LYRICA®) are preferable first line agents for the treatment of neuropathic pain rather than traditional, older agents such as Carbamazepine (TEGRETOL®), Phenytoin (DILANTIN®) and Valproate (DEPAKOTE®), as the newer agents are associated with fewer drug interactions. The newer agents bind to the alpha2-delta subunit of the calcium-sensitive channels, modulating neurotransmitter release. Of the newer agents, NEURONTIN® (Gabapentin) is not protein bound and is excreted unchanged in the urine and therefore has fewer drug interactions. If opioids are a consideration for neuropathic pain relief, the lowest dose is recommended. Topical therapies for neuropathic pain have the advantage of controlling pain without systemic side effects. It therefore can be combined with systemic treatment. Lidocaine 5% patches (LIDODERM®) block neuronal sodium channels whereas Capsaicin cream (ZOSTRIX®) stimulates the C fibers to release and subsequently deplete substance P, there by blocking pain signaling to the brain. Diclofenac gel 1% when applied once a day, concentrates in the dermis and has less gastrointestinal side effects and may be beneficial for neuropathic pain. A combination of Ketamine 1% and Amitriptyline 2% cream applied topically has also been promising in a small study. Patients experiencing refractory pain may benefit with the use of Transcutaneous Electrical Nerve Stimulation (TENS), although referral to the pain clinic may be appropriate. Psychosocial support utilizing a team of specialists and social workers/counsellors, should be an integral part of pain management. Kvale E and Urba SG. National Comprehensive Cancer Network (NCCN) 19th Annual Conference, March 13 – 15, 2014; Hollywood, Florida
A Less Intense Schedule of ZOMETA® for Patients with Metastatic Breast Cancer
Bisphosphonates inhibit osteoclast-mediated bone resorption and both oral and IV bisphosphonates reduce the risk of developing Skeletal Related Events (SRE’s) and delay the time to SRE’s in patients with Breast Cancer with bone metastases. In a study presented at ASCO 2014 meeting, continuing ZOMETA® (Zoledronic acid) for an additional year at the every 12 week schedule was non-inferior to ZOMETA® given every 4 weeks, among patients who had initially received IV bisphosphonates monthly, for one year or longer. This less frequent dosing of ZOMETA® compared with the standard monthly dosing, may be more convenient for the patients and result in less toxicities without compromising efficacy. More information at www.oncoprescribe.com
Continuous treatment (CT) versus fixed duration of therapy (FDT) in newly diagnosed myeloma patients PFS1, PFS2, OS endpoints
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, 24,050 new cases will be diagnosed in 2014 and 11,090 will die of the disease. Maintenance or Continuous Treatment in patients with newly diagnosed multiple myeloma following induction and consolidation can result in significantly longer Progression Free Survival (PFS) and Overall Survival (OS), compared to those patients who receive therapy for a fixed duration of time. Not all studies however, have shown Overall Survival benefit. It has been hypothesized that Continuous Treatment could result in resistance to therapy which in turn could reduce the duration of subsequent remission after first relapse and negatively impact overall survival.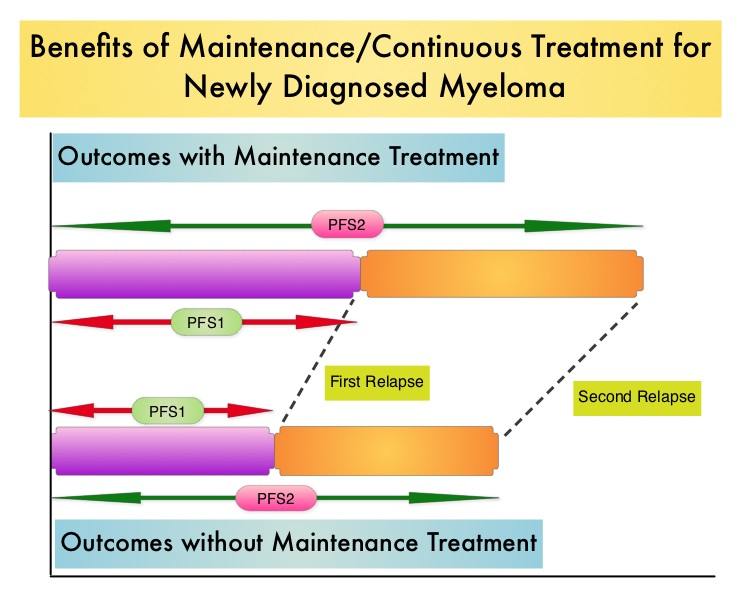 To address this controversy, the authors conducted a pooled analysis of the outcomes of two randomized phase III trials, designed to compare Continuous Treatment to Fixed Duration Therapy. In trail RVMM209, patients were randomized to either induction with Lenolidomide (REVLIMID®), followed by consolidation and subsequent maintenance with REVLIMID® (Continuous Treatment) or Fixed Duration Therapy which entailed REVLIMID® based induction followed by consolidation but no maintenance therapy. In Trial GIMEMA0305, the randomization was between Bortezomib (VELCADE®) based induction followed by maintenance treatment (Continuous Treatment) and VELCADE® induction, with no maintenance treatment (Fixed Duration Therapy). The trial investigators assessed PFS1 as the time from diagnosis to the occurrence of 1st relapse, PFS2 as time from diagnosis to the occurrence of 2nd relapse and Overall Survival as time from diagnosis to death , incorporating the duration of both 1st and 2nd remission. They then evaluated, both PFS1, PFS2 and OS in newly diagnosed multiple myeloma patients who received Continuous Therapy or Fixed Duration Therapy. In this pooled analysis 452 patients received Continuous Treatment and 461 patients received Fixed Duration Therapy .The median follow up was 52 months. Patients receiving Continuous Treatment had significantly prolonged PFS1 (median 35 months vs 24 months, HR 0.58; P<0.0001), PFS2 (median 63 months vs 47 months, HR 0.69, P=0.0001) and OS (median not reached [NR] vs 70 months, HR 0.70, P=0.0019), when compared with Fixed Dose Therapy. The authors evaluated the PFS and OS from first relapse to second relapse and from first relapse to death respectively, and they noted that the outcomes were similar among patients who received Continuous Treatment or Fixed Dose Therapy following initial diagnosis. The authors concluded that Continuous Treatment significantly improved PFS1, PFS2, and OS and findings from this pooled analysis suggested that the clinical benefit observed during first remission was not negated by a shorter second remission and Continuous Treatment did not induce tumor resistance. Continuous Treatment may be essential, as patients with multiple myeloma will always have some residual disease. It should be noted that certain institutions including the Mayo Clinic cap Continuous/Maintenance treatment at approximately 2 years, due to the lack of randomized comparative data, on the value of prolonged maintenance beyond 2 years. Palumbo A, Gay F, Musto P, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 8515)
To address this controversy, the authors conducted a pooled analysis of the outcomes of two randomized phase III trials, designed to compare Continuous Treatment to Fixed Duration Therapy. In trail RVMM209, patients were randomized to either induction with Lenolidomide (REVLIMID®), followed by consolidation and subsequent maintenance with REVLIMID® (Continuous Treatment) or Fixed Duration Therapy which entailed REVLIMID® based induction followed by consolidation but no maintenance therapy. In Trial GIMEMA0305, the randomization was between Bortezomib (VELCADE®) based induction followed by maintenance treatment (Continuous Treatment) and VELCADE® induction, with no maintenance treatment (Fixed Duration Therapy). The trial investigators assessed PFS1 as the time from diagnosis to the occurrence of 1st relapse, PFS2 as time from diagnosis to the occurrence of 2nd relapse and Overall Survival as time from diagnosis to death , incorporating the duration of both 1st and 2nd remission. They then evaluated, both PFS1, PFS2 and OS in newly diagnosed multiple myeloma patients who received Continuous Therapy or Fixed Duration Therapy. In this pooled analysis 452 patients received Continuous Treatment and 461 patients received Fixed Duration Therapy .The median follow up was 52 months. Patients receiving Continuous Treatment had significantly prolonged PFS1 (median 35 months vs 24 months, HR 0.58; P<0.0001), PFS2 (median 63 months vs 47 months, HR 0.69, P=0.0001) and OS (median not reached [NR] vs 70 months, HR 0.70, P=0.0019), when compared with Fixed Dose Therapy. The authors evaluated the PFS and OS from first relapse to second relapse and from first relapse to death respectively, and they noted that the outcomes were similar among patients who received Continuous Treatment or Fixed Dose Therapy following initial diagnosis. The authors concluded that Continuous Treatment significantly improved PFS1, PFS2, and OS and findings from this pooled analysis suggested that the clinical benefit observed during first remission was not negated by a shorter second remission and Continuous Treatment did not induce tumor resistance. Continuous Treatment may be essential, as patients with multiple myeloma will always have some residual disease. It should be noted that certain institutions including the Mayo Clinic cap Continuous/Maintenance treatment at approximately 2 years, due to the lack of randomized comparative data, on the value of prolonged maintenance beyond 2 years. Palumbo A, Gay F, Musto P, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 8515)
Immediate versus deferred initiation of androgen deprivation therapy in prostate cancer patients with PSA-only relapse
SUMMARY:Prostate cancer is the most common cancer in American men, excluding skin cancer and 1 in 7 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, over 230,000 new cases of prostate cancer will be diagnosed in 2014 and close to 30,000 men will die of the disease. The major source of PSA (Prostate Specific Antigen) is the prostate gland and the PSA levels are therefore undetectable within 6 weeks after Radical Prostatectomy. Similarly, following Radiation Therapy, there is a gradual decline in PSA before reaching a post treatment nadir. A detectable PSA level after Radical Prostatectomy, or a rising PSA level following Radiation Therapy, is considered PSA failure or biochemical recurrence.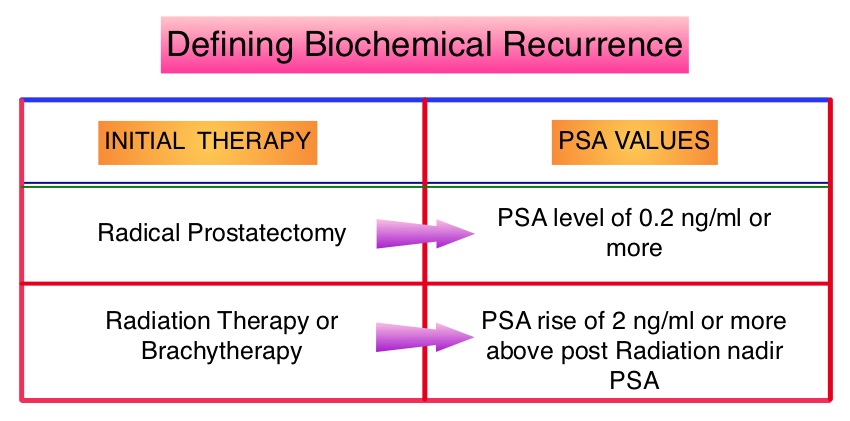 The American Urological Association suggested that a PSA of 0.2 ng/mL or higher defines PSA failure or relapse, after Radical Prostatectomy. A PSA rise of 2 ng/ml or more above post Radiation Therapy nadir, is considered PSA failure or relapse. Approximately 35% of the patients with prostate cancer will experience PSA only relapse within 10 years of their primary treatment and a third of these patients will develop documented metastatic disease within 8 years following PSA only relapse. Prostate cancer patients who had thought that they were cured, consequently can experience considerable mental anguish and anxiety, based on these laboratory findings. Androgen Deprivation Therapy (ADT) is often initiated following PSA only relapse with the intent of delaying disease progression although the role of ADT and optimal timing to start ADT (Immediate vs deferred ADT) in this patient population is unknown. Further, ADT can be associated with side effects such as fatigue, loss of muscle mass, impotence, anemia, osteoporosis, etc., which in turn can have a significant negative impact on an individual’s quality of life. In order to determine the significance of benefit if any, with starting ADT while patients are asymptomatic, the authors analyzed data on more than 14,000 patients included in a prospective registry called CaPSURE (Cancer of the Prostate Strategic Urologic Research Endeavor) and of them studied 2,022 men, who had experienced a PSA only relapse following curative surgery or radiation. These patients had clinical stage T3a,N0M0 or lower stage prostate cancer and experienced PSA only relapse (defined as PSA of 0.2 ng/mL or higher after Radical Prostatectomy or three rising PSA values one month apart following radiation treatment. Patients with symptoms, documented metastatic disease by CT scan or bone scan and ADT in the previous 12 months were excluded. Patients in the” Immediate treatment group” initiated ADT within 3 months of PSA relapse and those in the “Deferred treatment group” initiated ADT, 2 or more years after PSA relapse or when they presented with metastasis, symptoms or had a short PSA doubling time. The median age was 69 years, 34% had a Gleason score >7 and 32% received radiotherapy as primary treatment. The median time from primary treatment to PSA relapse was 27 months. Patients were followed for a median of 52.3 months after PSA relapse. The Five-year survival rate for Patients in the” Immediate treatment group” was 85.1% and for those in the “Deferred treatment group” was 87.2% with no significant difference in the all cause mortality. The 10 year survival was identical in both groups at 71.6%. The authors concluded that there is little or no survival benefit for Immediate ADT initiation compared with Deferred ADT initiation (at clinical progression or at least two years after PSA relapse) among prostate cancer patients with PSA only relapse. Therefore delaying ADT for at least 2 years after PSA relapse, following curative therapy for prostate cancer does not worsen overall survival. The findings from this large observational study will need further validation and a randomized phase III trial is underway to confirm these findings. Garcia-Albeniz X, Chan JM, Paciorek AT, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 5003)
The American Urological Association suggested that a PSA of 0.2 ng/mL or higher defines PSA failure or relapse, after Radical Prostatectomy. A PSA rise of 2 ng/ml or more above post Radiation Therapy nadir, is considered PSA failure or relapse. Approximately 35% of the patients with prostate cancer will experience PSA only relapse within 10 years of their primary treatment and a third of these patients will develop documented metastatic disease within 8 years following PSA only relapse. Prostate cancer patients who had thought that they were cured, consequently can experience considerable mental anguish and anxiety, based on these laboratory findings. Androgen Deprivation Therapy (ADT) is often initiated following PSA only relapse with the intent of delaying disease progression although the role of ADT and optimal timing to start ADT (Immediate vs deferred ADT) in this patient population is unknown. Further, ADT can be associated with side effects such as fatigue, loss of muscle mass, impotence, anemia, osteoporosis, etc., which in turn can have a significant negative impact on an individual’s quality of life. In order to determine the significance of benefit if any, with starting ADT while patients are asymptomatic, the authors analyzed data on more than 14,000 patients included in a prospective registry called CaPSURE (Cancer of the Prostate Strategic Urologic Research Endeavor) and of them studied 2,022 men, who had experienced a PSA only relapse following curative surgery or radiation. These patients had clinical stage T3a,N0M0 or lower stage prostate cancer and experienced PSA only relapse (defined as PSA of 0.2 ng/mL or higher after Radical Prostatectomy or three rising PSA values one month apart following radiation treatment. Patients with symptoms, documented metastatic disease by CT scan or bone scan and ADT in the previous 12 months were excluded. Patients in the” Immediate treatment group” initiated ADT within 3 months of PSA relapse and those in the “Deferred treatment group” initiated ADT, 2 or more years after PSA relapse or when they presented with metastasis, symptoms or had a short PSA doubling time. The median age was 69 years, 34% had a Gleason score >7 and 32% received radiotherapy as primary treatment. The median time from primary treatment to PSA relapse was 27 months. Patients were followed for a median of 52.3 months after PSA relapse. The Five-year survival rate for Patients in the” Immediate treatment group” was 85.1% and for those in the “Deferred treatment group” was 87.2% with no significant difference in the all cause mortality. The 10 year survival was identical in both groups at 71.6%. The authors concluded that there is little or no survival benefit for Immediate ADT initiation compared with Deferred ADT initiation (at clinical progression or at least two years after PSA relapse) among prostate cancer patients with PSA only relapse. Therefore delaying ADT for at least 2 years after PSA relapse, following curative therapy for prostate cancer does not worsen overall survival. The findings from this large observational study will need further validation and a randomized phase III trial is underway to confirm these findings. Garcia-Albeniz X, Chan JM, Paciorek AT, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 5003)
Final results of a randomized phase 2 study showing the clinical benefit of quizartinib (AC220) in patients with FLT3-ITD positive relapsed or refractory acute myeloid leukemia
SUMMARY: Acute Myeloid Leukemia (AML) is generally a disease of the elderly and the average age of a patient at the time of diagnosis is about 66 years. According to the American Cancer Society, approximately 18,860 new cases of AML will be diagnosed in 2014 and 10,460 patients will die of the disease. AML can be considered as a group of heterogeneous diseases with different clinical behavior and outcomes. Even though cytotoxic chemotherapy may lead to long term remission and cure in a minority of patients with favorable cytogenetics, patients with high risk features such as unfavorable cytogenetics, molecular abnormalities, prior myelodysplasia and advanced age, have poor outcomes with conventional chemotherapy. 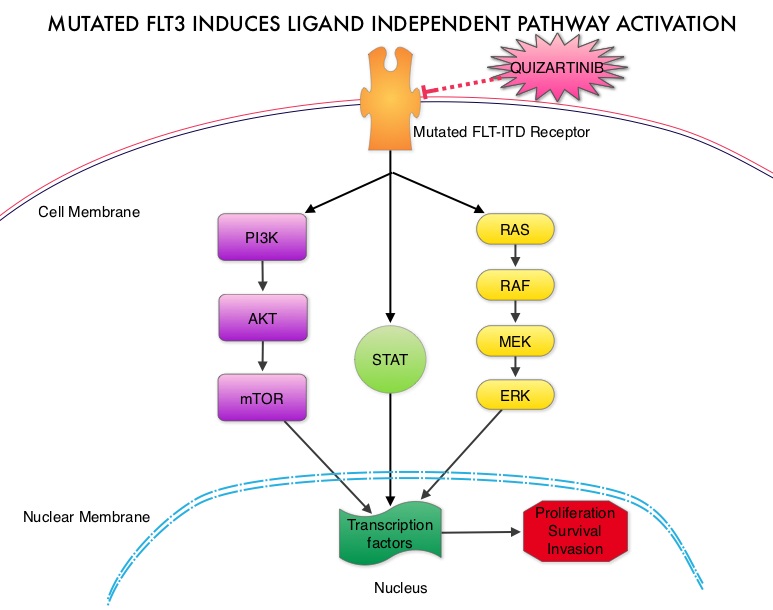 The fms-like tyrosine kinase 3 (FLT3) is a receptor tyrosine kinase in the PDGF family of growth factor receptors located on the cell surface (transmembrane) and plays an important role in both normal and malignant hematopoiesis by activating key signaling pathways. Activating mutations in the FLT3 receptor is the most common genetic abnormality in AML and is detected in approximately 30% of the patients. The most common FLT3 mutation is the FLT3-ITD (Internal Tandem Duplication) mutation caused by a tandem duplication within the coding region of the gene. The presence of FLT3-ITD mutations can negate the benefit of any other favorable molecular and cytogenetic features. Patients with FLT3-ITD mutations have poor outcomes with shorter remission duration and significantly decreased leukemia free and overall survival. These mutations are detected using Polymerase Chain Reaction (PCR) based molecular diagnostic DNA testing. Several therapeutic agents are being developed to target FLT3 mutations. Quizartinib (AC220) is an oral tyrosine kinase inhibitor, which has demonstrated activity in patients with both wild type FLT3 as well as those with FLT3-ITD mutations. In this randomized, open label phase II study, the authors evaluated the efficacy and safety of two different, lower dosages of Quizartinib, in patients 18 years of age or older, with FLT3-ITD positive, relapsed or refractory AML. Seventy six patients (N=76) were randomized to receive either Quizartinib 30 mg/day (Group A) or Quizartinib 60 mg/day (Group B), given orally and continuously, during a 28 day treatment cycle. Treatment was continued until relapse, intolerance or Hematopoietic Stem Cell Transplantation (HSCT). Both groups were well balanced except for age over 60 years (42% Group A, 26% Group B) and the percentage with secondary AML (8% Group A, 18% Group B). The composite Complete Remission (CRc) rate included Complete Remission (CR), Complete Remission with incomplete platelet recovery (CRp), and Complete Remission with incomplete hematologic recovery (CRi). The CRc rate in both groups A and B was 47% and the Overall Response Rate (CRc + Partial Response (PR)) was 61% in Group A and 71% in Group B. Further, 32% of patiens in Group A and 42% in Group B were able to undergo HSCT, after achieving CRc or PR. The most common treatment related adverse events were diarrhea (18%), febrile neutropenia (16%), and QT prolongation (15%). The QT prolongation rate was significantly less with lower doses of Quizartinib, as was used in this study, compared to what was noted with higher doses of Quizartinib utilized in other trials. The authors concluded that Quizartinib is highly effective in relapsed and refractory AML patients with FLT3-ITD mutations, with an acceptable safety profile. Schiller GJ, Tallman MS, Goldberg SL, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7100)
The fms-like tyrosine kinase 3 (FLT3) is a receptor tyrosine kinase in the PDGF family of growth factor receptors located on the cell surface (transmembrane) and plays an important role in both normal and malignant hematopoiesis by activating key signaling pathways. Activating mutations in the FLT3 receptor is the most common genetic abnormality in AML and is detected in approximately 30% of the patients. The most common FLT3 mutation is the FLT3-ITD (Internal Tandem Duplication) mutation caused by a tandem duplication within the coding region of the gene. The presence of FLT3-ITD mutations can negate the benefit of any other favorable molecular and cytogenetic features. Patients with FLT3-ITD mutations have poor outcomes with shorter remission duration and significantly decreased leukemia free and overall survival. These mutations are detected using Polymerase Chain Reaction (PCR) based molecular diagnostic DNA testing. Several therapeutic agents are being developed to target FLT3 mutations. Quizartinib (AC220) is an oral tyrosine kinase inhibitor, which has demonstrated activity in patients with both wild type FLT3 as well as those with FLT3-ITD mutations. In this randomized, open label phase II study, the authors evaluated the efficacy and safety of two different, lower dosages of Quizartinib, in patients 18 years of age or older, with FLT3-ITD positive, relapsed or refractory AML. Seventy six patients (N=76) were randomized to receive either Quizartinib 30 mg/day (Group A) or Quizartinib 60 mg/day (Group B), given orally and continuously, during a 28 day treatment cycle. Treatment was continued until relapse, intolerance or Hematopoietic Stem Cell Transplantation (HSCT). Both groups were well balanced except for age over 60 years (42% Group A, 26% Group B) and the percentage with secondary AML (8% Group A, 18% Group B). The composite Complete Remission (CRc) rate included Complete Remission (CR), Complete Remission with incomplete platelet recovery (CRp), and Complete Remission with incomplete hematologic recovery (CRi). The CRc rate in both groups A and B was 47% and the Overall Response Rate (CRc + Partial Response (PR)) was 61% in Group A and 71% in Group B. Further, 32% of patiens in Group A and 42% in Group B were able to undergo HSCT, after achieving CRc or PR. The most common treatment related adverse events were diarrhea (18%), febrile neutropenia (16%), and QT prolongation (15%). The QT prolongation rate was significantly less with lower doses of Quizartinib, as was used in this study, compared to what was noted with higher doses of Quizartinib utilized in other trials. The authors concluded that Quizartinib is highly effective in relapsed and refractory AML patients with FLT3-ITD mutations, with an acceptable safety profile. Schiller GJ, Tallman MS, Goldberg SL, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7100)
Belinostat, a novel pan-histone deacetylase inhibitor (HDACi), in relapsed or refractory peripheral T-cell lymphoma (R/R PTCL) Results from the BELIEF trial
SUMMARY: Non-Hodgkin lymphoma (NHL) is one of the most common cancers in the United States and the American Cancer Society estimates that in 2014, about 70,800 people will be diagnosed with NHL in the US and close to 19,000 people will die of the disease. T cell Lymphomas are a heterogenous group of lymphoid malignancies representing less than 15% of all Non-Hodgkin Lymphomas.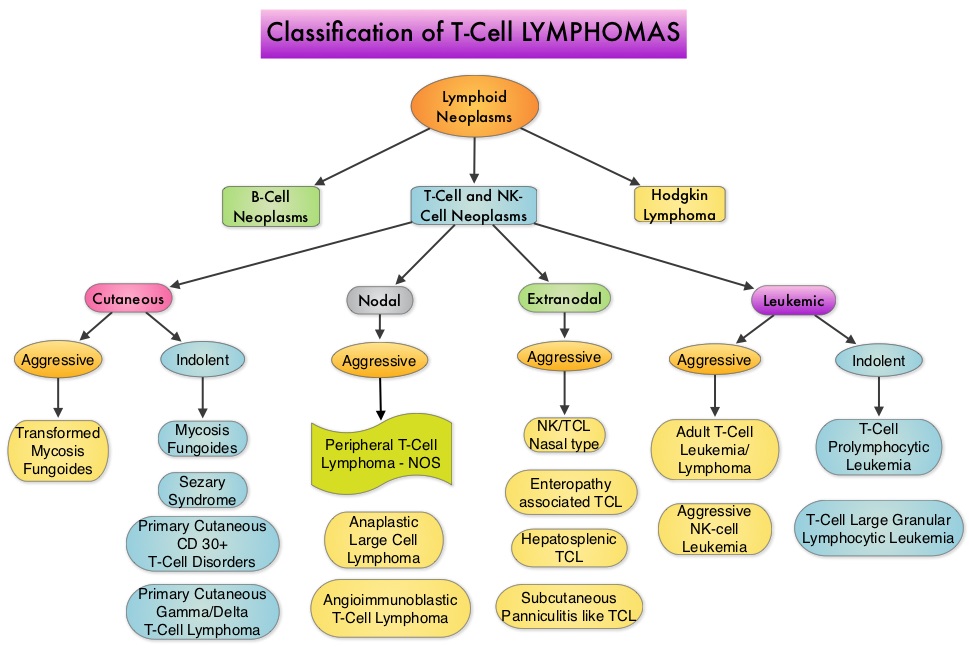
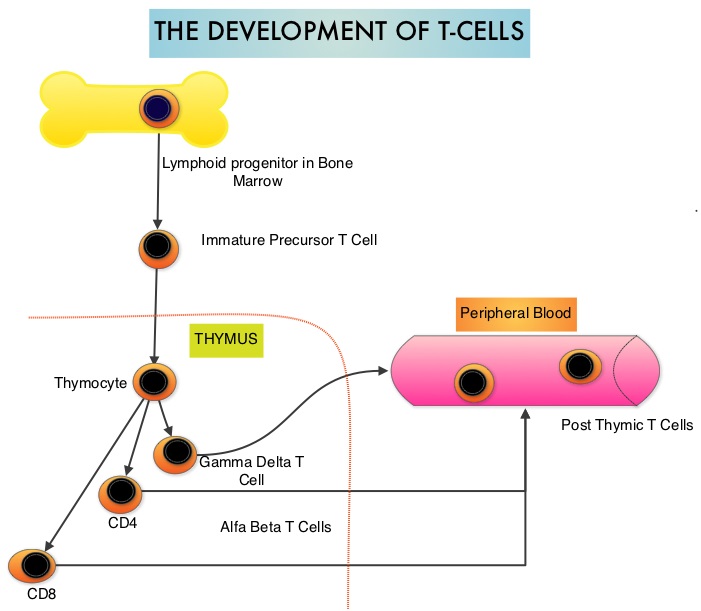 Peripheral T-cell lymphoma – NOS (PTCL-Not Otherwise Specified) is the most common of the aggressive T-cell lymphoma subtypes and accounts for 26% of all non-cutaneous PTCL’s. These malignancies are derived from mature post thymic T-cells and NK cells. These tumors are uncommon, tend to be aggressive and majority of the patients with T-cell lymphoma present with advanced stage disease and respond poorly to treatment. Relapse rates tend to be high and few patients achieve durable remission with treatment. For these reasons, prognosis remains poor. Agents from two pharmacological classes are presently available for the treatment of PTCL. The FDA granted accelerated approval to FOLOTYN® (Pralatrexate), an antifolate, in 2009, for use in patients with relapsed or refractory PTCL and to ISTODAX® (Romidepsin), a histone deacetylase (HDAC) inhibitor in 2011, for the treatment of PTCL patients, who had received at least one prior therapy.
Peripheral T-cell lymphoma – NOS (PTCL-Not Otherwise Specified) is the most common of the aggressive T-cell lymphoma subtypes and accounts for 26% of all non-cutaneous PTCL’s. These malignancies are derived from mature post thymic T-cells and NK cells. These tumors are uncommon, tend to be aggressive and majority of the patients with T-cell lymphoma present with advanced stage disease and respond poorly to treatment. Relapse rates tend to be high and few patients achieve durable remission with treatment. For these reasons, prognosis remains poor. Agents from two pharmacological classes are presently available for the treatment of PTCL. The FDA granted accelerated approval to FOLOTYN® (Pralatrexate), an antifolate, in 2009, for use in patients with relapsed or refractory PTCL and to ISTODAX® (Romidepsin), a histone deacetylase (HDAC) inhibitor in 2011, for the treatment of PTCL patients, who had received at least one prior therapy.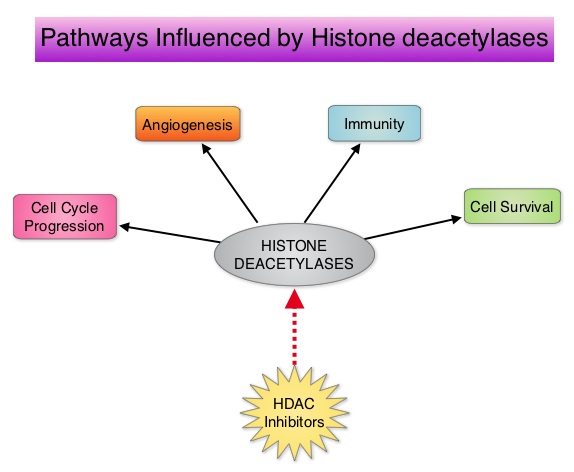 HDACs are a family of enzymes that play an important role in the regulation of gene expression. To briefly summarize the structure of a chromosome, individual loops of coiled double-helix DNA wrap around a histone protein to form a nucleosome. Nucleosomes are then coiled together to form chromatin fibers, which looks like beads on a string. The chromatin fibers are coiled even more tightly to form chromosomes. HDAC enzymes catalyze the removal of acetyl groups and regulate the level of acetylation of the histones and non-histone proteins and transcription of several genes. Hypoacetylation of histones has been associated with a condensed chromatin structure that results in the repression of gene transcription, whereas acetylated histones are associated with a more open chromatin structure and activation of gene transcription. HDACs are grouped into four major classes and regulate cell-cycle progression, cell survival, angiogenesis and immunity. BELEODAQ® (Belinostat) is a novel pan-histone deacetylase inhibitor and inhibits all 3 classes of the zinc-dependent HDAC enzymes.
HDACs are a family of enzymes that play an important role in the regulation of gene expression. To briefly summarize the structure of a chromosome, individual loops of coiled double-helix DNA wrap around a histone protein to form a nucleosome. Nucleosomes are then coiled together to form chromatin fibers, which looks like beads on a string. The chromatin fibers are coiled even more tightly to form chromosomes. HDAC enzymes catalyze the removal of acetyl groups and regulate the level of acetylation of the histones and non-histone proteins and transcription of several genes. Hypoacetylation of histones has been associated with a condensed chromatin structure that results in the repression of gene transcription, whereas acetylated histones are associated with a more open chromatin structure and activation of gene transcription. HDACs are grouped into four major classes and regulate cell-cycle progression, cell survival, angiogenesis and immunity. BELEODAQ® (Belinostat) is a novel pan-histone deacetylase inhibitor and inhibits all 3 classes of the zinc-dependent HDAC enzymes.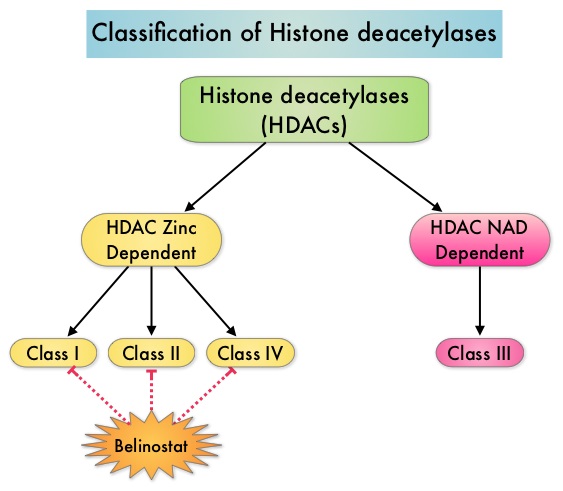 The approval of BELEODAQ® was based on the results of a multi-center, single-arm, phase II trial, in which 129 patients with relapsed or refractory PTCL, who had received a median of 2 prior therapies, were enrolled and evaluated. BELEODAQ® was administered as a 30 minute IV infusion at 1000 mg/m2 on days 1–5 of a 3 week cycle until progression or unacceptable toxicity. The median age was 63 years. The primary endpoint was Overall Response Rate (ORR). The ORR was 26% with 10% Complete Responses and 10% Partial responses and the median time to response was 5.6 weeks and the median duration of response was 8.3 months. The most common adverse events were nausea, vomiting, fatigue, fever and anemia. The most common grade 3/4 adverse events were thrombocytopenia (13%), neutropenia (13%), anemia (10%), dyspnea (6%), pneumonia (6%), and fatigue (5%). The authors concluded that BELEODAQ® demonstrated a significant overall response rate in relapsed /refractory PTCL patients, thus expanding the treatment options for these difficult to treat individuals. This was accomplished with a low incidence of myelosuppression and favorable safety profile. O'Connor OA, Masszi T, Savage KJ, et al. J Clin Oncol 31, 2013 (suppl; abstr 8507)
The approval of BELEODAQ® was based on the results of a multi-center, single-arm, phase II trial, in which 129 patients with relapsed or refractory PTCL, who had received a median of 2 prior therapies, were enrolled and evaluated. BELEODAQ® was administered as a 30 minute IV infusion at 1000 mg/m2 on days 1–5 of a 3 week cycle until progression or unacceptable toxicity. The median age was 63 years. The primary endpoint was Overall Response Rate (ORR). The ORR was 26% with 10% Complete Responses and 10% Partial responses and the median time to response was 5.6 weeks and the median duration of response was 8.3 months. The most common adverse events were nausea, vomiting, fatigue, fever and anemia. The most common grade 3/4 adverse events were thrombocytopenia (13%), neutropenia (13%), anemia (10%), dyspnea (6%), pneumonia (6%), and fatigue (5%). The authors concluded that BELEODAQ® demonstrated a significant overall response rate in relapsed /refractory PTCL patients, thus expanding the treatment options for these difficult to treat individuals. This was accomplished with a low incidence of myelosuppression and favorable safety profile. O'Connor OA, Masszi T, Savage KJ, et al. J Clin Oncol 31, 2013 (suppl; abstr 8507)
Efficacy and safety of continued zoledronic acid every 4 weeks versus every 12 weeks in women with bone metastases from breast cancer Results of the OPTIMIZE-2 trial
SUMMARY: Bone is the most common site of metastatic disease, in patients with Breast Cancer. Bisphosphonates inhibit osteoclast-mediated bone resorption and both oral and IV bisphosphonates reduce the risk of developing Skeletal Related Events (SRE’s) and delay the time to SRE’s in patients with Breast Cancer with bone metastases. Bisphosphonates can also reduce bone pain and may improve Quality of life. Of the four bisphosphonates proven to be effective in patients with Breast Cancer with bone metastases, only intravenous Pamidronate (AREDIA®) and Zoledronic acid (ZOMETA®) have been approved in the USA, whereas intravenous and oral Ibandronate and oral Clodronate have been approved in Europe. Both AREDIA® and ZOMETA® are administered every 3 to 4 weeks during the first year, following diagnoses of bone metastases. However, the optimal treatment schedule following this initial phase of treatment has remained unclear. Further, renal toxicity, long bone fractures and OsteoNecrosis of the Jaw (ONJ) have been identified as potential problems with bisphosphonate use.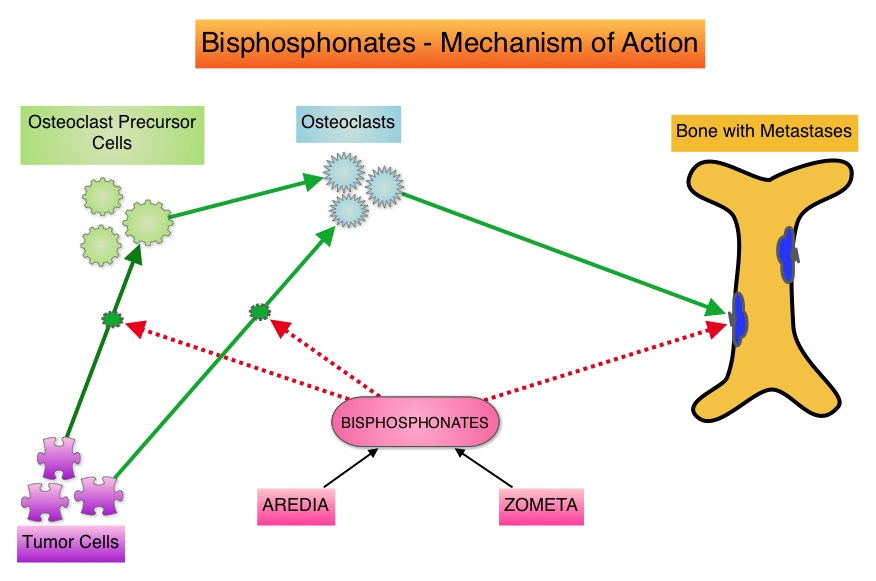 OPTIMIZE-2 is a prospective, randomized, double-blind, multicenter trial, in which the authors evaluated the outcomes of a less intense schedule of ZOMETA® administered every 12 weeks, following one year of the standard initial phase of treatment with bisphosphonates. This study included 403 women with bone metastases from Breast Cancer, who had received 9 or more doses of either intravenous ZOMETA® or AREDIA®, during the first 10-15 months of therapy. The median age was 59 years and patients were randomized (1:1) to receive either ZOMETA® 4 mg IV every 4 weeks (N=200) or every 12 weeks (N=203), for one year. The primary endpoint was Skeletal Related Event (SRE) rate, defined as the proportion of patients with one or more SRE’s (pathologic fractures, spinal cord compression, need for radiotherapy or surgical stabilization of the bone). The primary analysis was non-inferiority, for the difference in SRE rates between the treatment groups. Secondary endpoints included time to first SRE, Skeletal Morbidity Rate (SMR), bone pain score, change in bone turnover markers, and safety. After a median follow up of 11.9 months, the SRE rate was 22% and 23.2% in the ZOMETA® every 4 weeks group and ZOMETA® every 12 weeks group respectively (P=0.724), suggesting that ZOMETA® given every 12 weeks was non-inferior to the q 4 week regimen. The secondary endpoints were comparable as well. More patients had renal toxicities in the ZOMETA® q 4 week group vs q 12 week group (9.6% vs 7.9%, respectively) and two cases (1.0%) of OsteoNecrosis of the Jaw (ONJ) were reported in the ZOMETA® q 4 week group. The authors concluded that the efficacy of continuing ZOMETA® for an additional year at the q 12 week schedule was non-inferior to ZOMETA® given q 4 weeks, among patients who had initially received IV bisphosphonates monthly, for one year or longer. Further the less frequent dosing of ZOMETA® compared with the standard monthly dosing, may be more convenient for the patients and result in less toxicities. Hortobagyi GN, Lipton A, Chew HK, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA9500)
OPTIMIZE-2 is a prospective, randomized, double-blind, multicenter trial, in which the authors evaluated the outcomes of a less intense schedule of ZOMETA® administered every 12 weeks, following one year of the standard initial phase of treatment with bisphosphonates. This study included 403 women with bone metastases from Breast Cancer, who had received 9 or more doses of either intravenous ZOMETA® or AREDIA®, during the first 10-15 months of therapy. The median age was 59 years and patients were randomized (1:1) to receive either ZOMETA® 4 mg IV every 4 weeks (N=200) or every 12 weeks (N=203), for one year. The primary endpoint was Skeletal Related Event (SRE) rate, defined as the proportion of patients with one or more SRE’s (pathologic fractures, spinal cord compression, need for radiotherapy or surgical stabilization of the bone). The primary analysis was non-inferiority, for the difference in SRE rates between the treatment groups. Secondary endpoints included time to first SRE, Skeletal Morbidity Rate (SMR), bone pain score, change in bone turnover markers, and safety. After a median follow up of 11.9 months, the SRE rate was 22% and 23.2% in the ZOMETA® every 4 weeks group and ZOMETA® every 12 weeks group respectively (P=0.724), suggesting that ZOMETA® given every 12 weeks was non-inferior to the q 4 week regimen. The secondary endpoints were comparable as well. More patients had renal toxicities in the ZOMETA® q 4 week group vs q 12 week group (9.6% vs 7.9%, respectively) and two cases (1.0%) of OsteoNecrosis of the Jaw (ONJ) were reported in the ZOMETA® q 4 week group. The authors concluded that the efficacy of continuing ZOMETA® for an additional year at the q 12 week schedule was non-inferior to ZOMETA® given q 4 weeks, among patients who had initially received IV bisphosphonates monthly, for one year or longer. Further the less frequent dosing of ZOMETA® compared with the standard monthly dosing, may be more convenient for the patients and result in less toxicities. Hortobagyi GN, Lipton A, Chew HK, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA9500)
Increased Risk of Pancreatic Adenocarcinoma After Acute Pancreatitis
SUMMARY: The American Cancer Society estimates that in 2014, over 46,000 people will be diagnosed with Pancreatic Cancer in the United States and close to 40,000 people will die of the disease. Some important risk factors for Pancreatic Cancer include increasing age, obesity, smoking history, genetic predisposition, exposure to certain dyes and chemicals, heavy alcohol use and pancreatitis. The best chance for long term survival is complete surgical resection, although this may not be feasible in a majority of the patients, as they present with advanced disease, at the time of diagnosis. Based on the National Cancer Data Base, the 5 year observed survival rate for patients diagnosed with exocrine cancer of the pancreas is 14% for those with Stage IA disease and 1% for those with Stage IV disease. Early diagnosis may therefore play an important role in treatment outcomes, in patients with Pancreatic Cancer. Pancreatic Cancer can cause acute pancreatitis by obstructing the pancreatic duct and patients diagnosed with Pancreatic Cancer often present initially with acute pancreatitis. With this background information, the authors performed a retrospective study of patients with acute pancreatitis who sought their medical care at the Veterans Health Administration from 1998 through 2007.  Patients with pre-existing Pancreatic Adenocarcinoma or those with recurrent acute pancreatitis were excluded from this analysis. A diagnosis of acute pancreatitis was made in 5720 patients and 710 patients were diagnosed with Pancreatic Cancer from 2000 through 2007. They noted that of those who were diagnosed with Pancreatic Adenocarcinoma, 76 patients (10.7%) had acute pancreatitis within 2 years of Pancreatic Cancer diagnosis. This risk for Pancreatic Cancer was greatest during the ï¬rst year following diagnosis of acute pancreatitis and this risk decreased rapidly thereafter. Patients less than 40 years of age had negligible risk whereas those 70 years of age or older had the highest risk. The authors concluded that a signiï¬cant number of patients with Pancreatic Adenocarcinoma (12.1%) initially present with acute pancreatitis and the diagnosis of cancer is often delayed by up to 2 years. Acute pancreatitis should be considered as an index event which in turn may identify a population of patients at high risk to develop Pancreatic Adenocarcinoma. They recommend that Endoscopic UltraSound (EUS) should be performed in these high risk patients, following diagnosis of acute pancreatitis, before discharge from the hospital, as this test is highly sensitive in picking up small tumors in the pancreas that are amenable to surgical resection. This is in comparison with contrast enhanced CT scans and pancreatic protocol CT scans that are not as sensitive in identifying tumors less than 2 cm in size. This interesting analysis could potentially open the doors for pancreatic cancer screening in high risk patients. Munigala S, Kanwal F, Xian H, et al. Clinical Gastroenterology and Hepatology 2014;12:1143-1150
Patients with pre-existing Pancreatic Adenocarcinoma or those with recurrent acute pancreatitis were excluded from this analysis. A diagnosis of acute pancreatitis was made in 5720 patients and 710 patients were diagnosed with Pancreatic Cancer from 2000 through 2007. They noted that of those who were diagnosed with Pancreatic Adenocarcinoma, 76 patients (10.7%) had acute pancreatitis within 2 years of Pancreatic Cancer diagnosis. This risk for Pancreatic Cancer was greatest during the ï¬rst year following diagnosis of acute pancreatitis and this risk decreased rapidly thereafter. Patients less than 40 years of age had negligible risk whereas those 70 years of age or older had the highest risk. The authors concluded that a signiï¬cant number of patients with Pancreatic Adenocarcinoma (12.1%) initially present with acute pancreatitis and the diagnosis of cancer is often delayed by up to 2 years. Acute pancreatitis should be considered as an index event which in turn may identify a population of patients at high risk to develop Pancreatic Adenocarcinoma. They recommend that Endoscopic UltraSound (EUS) should be performed in these high risk patients, following diagnosis of acute pancreatitis, before discharge from the hospital, as this test is highly sensitive in picking up small tumors in the pancreas that are amenable to surgical resection. This is in comparison with contrast enhanced CT scans and pancreatic protocol CT scans that are not as sensitive in identifying tumors less than 2 cm in size. This interesting analysis could potentially open the doors for pancreatic cancer screening in high risk patients. Munigala S, Kanwal F, Xian H, et al. Clinical Gastroenterology and Hepatology 2014;12:1143-1150