
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 233,000 new cases of invasive breast cancer will be diagnosed in 2014 and 40,000 women will die of the disease. Approximately 75% of patients with breast cancer are hormone receptor positive (Estrogen Receptor/Progesterone Receptor positive) and this is a predictor of response to endocrine therapy. In premenopausal woman, the ovary is the main source of estrogen production, whereas in postmenopausal women, the primary source of estrogen is the Aromatase enzyme mediated conversion of androstenedione and testosterone to estrone and estradiol in extragonadal/peripheral tissues.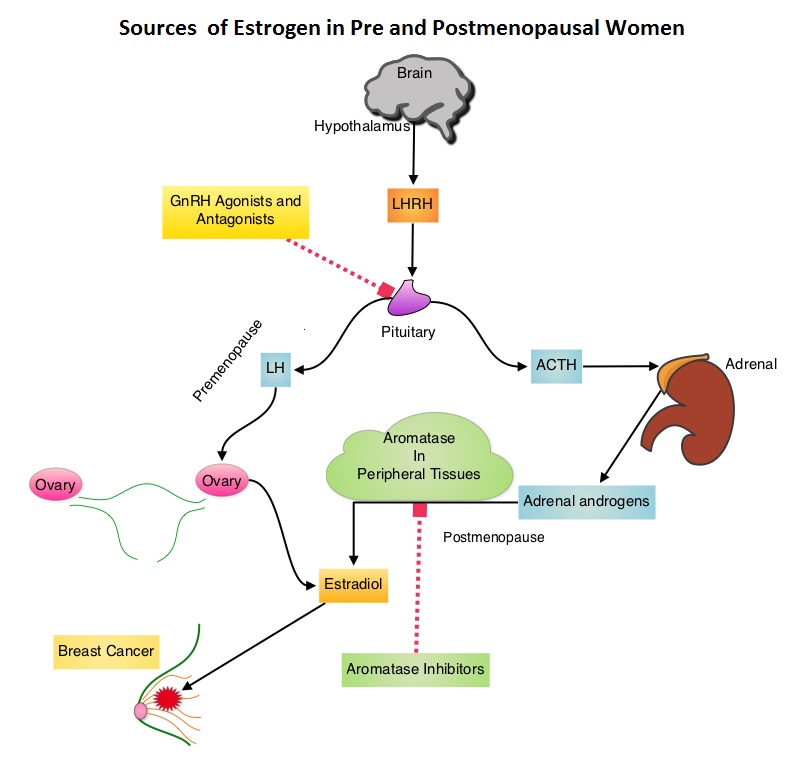 Presently available therapies include Tamoxifen and other Selective ER Modulators, which modulate ER alpha activity, Aromatase Inhibitors and Ovarian ablation that decrease estrogen production and FASLODEX® (Fulvestrant) that down regulates Estrogen Receptor. Aromatase Inhibitors (AI’s) are often prescribed, due to their superiority over Tamoxifen, for postmenopausal women with Hormone Receptor positive breast tumors, in adjuvant as well as metastatic settings. AI’s however, are not effective in premenopausal women, as these individuals derive their estrogen mainly from ovaries and not extragonadal tissues. The 2000 Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) overview, as well as subsequent studies comparing adjuvant ovarian ablation/suppression with adjuvant chemotherapy in premenopausal women with hormone positive breast tumors, have demonstrated similar magnitude of benefit. The TEXT (Tamoxifen and Exemestane Trial) and SOFT (Suppression of Ovarian Function Trial) are two phase III randomized trials, conducted at the same time and included premenopausal women (average age was 43 years) with hormone receptor positive early breast cancer. In the joint analysis of these two trials in which 5738 women were enrolled, the authors set out to answer 2 important questions – whether adjuvant AI improves outcomes in this patient group when their Ovarian Function is suppressed and whether there is any benefit with Ovarian Function suppression in premenopausal women suitable for adjuvant Tamoxifen. TEXT randomized patients (N=2672) within 3 months of surgery to 5 years of AROMASIN® (Exemestane) plus Ovarian Function Suppression (OFS) or 5 years of Tamoxifen plus OFS. The SOFT study randomized patients (N=3066) to 5 years of AROMASIN® plus OFS or 5 years of Tamoxifen plus OFS or 5 years of Tamoxifen alone. OFS choices included oophorectomy, ovarian irradiation or 5 years of TRELSTAR® (Triptorelin), a GnRH (Gonadotropin Releasing Hormone) agonist. The primary endpoint of these two studies was Disease Free Survival (DFS). In this joint analysis the outcomes for 4690 women randomized to receive AROMASIN® plus OFS or Tamoxifen plus OFS for 5 years, were analyzed. The 5 year Disease Free Survival was 91.1% in the AROMASIN® plus OFS group and 87.3% in the Tamoxifen plus OFS group (HR=0.72, P<0.0002). Compared to patients receiving Tamoxifen plus OFS, AROMASIN® plus OFS reduced the relative risk of premenopausal women developing a subsequent invasive breast cancer by 28% and the relative risk of breast cancer recurrence by 34%. The authors concluded that this largest joint analysis, evaluating adjuvant AI therapy with OFS in premenopausal women with Hormone receptor positive breast cancer, has demonstrated that 5 years of highly effective adjuvant endocrine therapy without chemotherapy can result in excellent outcomes. Further, AROMASIN® may be better than tamoxifen, when given with Ovarian Function Suppression. Pagani O, Regan MM, Walley B, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA1)
Presently available therapies include Tamoxifen and other Selective ER Modulators, which modulate ER alpha activity, Aromatase Inhibitors and Ovarian ablation that decrease estrogen production and FASLODEX® (Fulvestrant) that down regulates Estrogen Receptor. Aromatase Inhibitors (AI’s) are often prescribed, due to their superiority over Tamoxifen, for postmenopausal women with Hormone Receptor positive breast tumors, in adjuvant as well as metastatic settings. AI’s however, are not effective in premenopausal women, as these individuals derive their estrogen mainly from ovaries and not extragonadal tissues. The 2000 Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) overview, as well as subsequent studies comparing adjuvant ovarian ablation/suppression with adjuvant chemotherapy in premenopausal women with hormone positive breast tumors, have demonstrated similar magnitude of benefit. The TEXT (Tamoxifen and Exemestane Trial) and SOFT (Suppression of Ovarian Function Trial) are two phase III randomized trials, conducted at the same time and included premenopausal women (average age was 43 years) with hormone receptor positive early breast cancer. In the joint analysis of these two trials in which 5738 women were enrolled, the authors set out to answer 2 important questions – whether adjuvant AI improves outcomes in this patient group when their Ovarian Function is suppressed and whether there is any benefit with Ovarian Function suppression in premenopausal women suitable for adjuvant Tamoxifen. TEXT randomized patients (N=2672) within 3 months of surgery to 5 years of AROMASIN® (Exemestane) plus Ovarian Function Suppression (OFS) or 5 years of Tamoxifen plus OFS. The SOFT study randomized patients (N=3066) to 5 years of AROMASIN® plus OFS or 5 years of Tamoxifen plus OFS or 5 years of Tamoxifen alone. OFS choices included oophorectomy, ovarian irradiation or 5 years of TRELSTAR® (Triptorelin), a GnRH (Gonadotropin Releasing Hormone) agonist. The primary endpoint of these two studies was Disease Free Survival (DFS). In this joint analysis the outcomes for 4690 women randomized to receive AROMASIN® plus OFS or Tamoxifen plus OFS for 5 years, were analyzed. The 5 year Disease Free Survival was 91.1% in the AROMASIN® plus OFS group and 87.3% in the Tamoxifen plus OFS group (HR=0.72, P<0.0002). Compared to patients receiving Tamoxifen plus OFS, AROMASIN® plus OFS reduced the relative risk of premenopausal women developing a subsequent invasive breast cancer by 28% and the relative risk of breast cancer recurrence by 34%. The authors concluded that this largest joint analysis, evaluating adjuvant AI therapy with OFS in premenopausal women with Hormone receptor positive breast cancer, has demonstrated that 5 years of highly effective adjuvant endocrine therapy without chemotherapy can result in excellent outcomes. Further, AROMASIN® may be better than tamoxifen, when given with Ovarian Function Suppression. Pagani O, Regan MM, Walley B, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA1)
Category: Hem/Onc Updates
The ASH Choosing Wisely® campaign five hematologic tests and treatments to question
SUMMARY: CHOOSING WISELY® is a quality improvement initiative led by the American Board of Internal Medicine Foundation in collaboration with leading medical societies in the United States such as the American Society of Hematology (ASH). This organization was established to improve quality of medical care, after it was noted that about 25% of the tests ordered at the time of hospital admission and 65% of the tests ordered on subsequent days were avoidable. Further, there is ample evidence to suggest that reducing unneeded investigations can decrease costs, increase patient satisfaction and quality of care. CHOOSING WISELY® has challenged medical societies to identify 5 tests, procedures or treatments, within each specialty's clinical domain, that are offered to patients, despite the lack of evidence demonstrating its benefit. The goal is to make positive changes in the actual delivery of patient care. The ASH identified 5 tests and treatments that practicing hematologists should give due consideration to, that in some situations are not evidence based and which in certain cases are associated with risks that outweigh the benefits and are not cost efficient.
Multitarget Stool DNA Testing for Colorectal-Cancer Screening
SUMMARY: The American Cancer Society estimates that approximately 137,000 new cases of colorectal cancer will be diagnosed in the United States in 2014 and over 50,000 are expected to die of the disease. It is the third leading cause of cancer death in the U.S. and the lifetime risk of developing colorectal cancer is 1 in 20. Implementation of screening programs in the U.S. has resulted in a 46% decrease in the rate of death from colorectal cancer, from its peak. The U.S. Preventive Services Task Force recommends annual screening with high sensitivity Fecal Occult Blood Testing (FOBT), sigmoidoscopy every 5 years with high-sensitivity FOBT every 3 years and screening colonoscopy every 10 years. Fecal Immunochemical testing (FIT) measures intact human globin protein as opposed to heme. Animal heme from meat will not trigger a false positive test with FIT and as such dietary restrictions are not necessary. Further, FIT is superior to FOBT in detecting advanced adenomas and only requires one stool specimen, as opposed to three specimens for FOBT.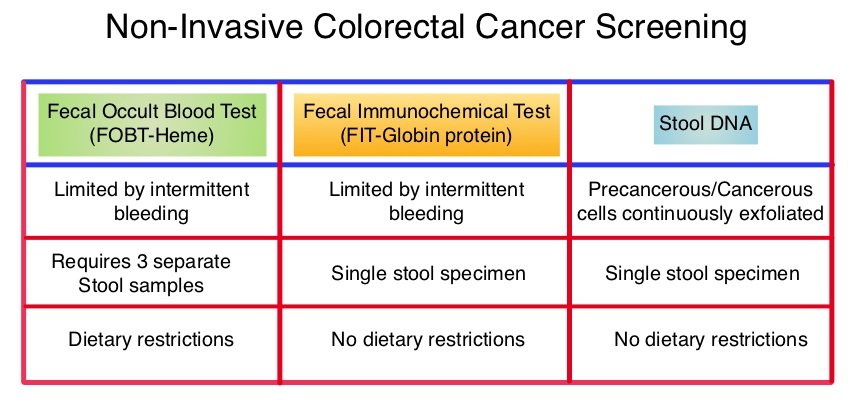 COLOGUARD® is highly sensitive, noninvasive, multitarget, stool based DNA test, for colorectal cancer screening ie.early detection of colorectal cancer and precancerous lesions. This test takes advantage of the genetic and epigenetic alterations that leads to the development of colorectal cancer and analyzes the altered DNA signatures of cancerous and precancerous cells that exfoliate into the colon. In addition, this test includes an immunochemical assay for human hemoglobin. The stool samples can be easily collected, mailed from home, and requires no bowel preparation, medication restrictions or dietary change. The purpose of this study was to determine the sensitivity of COLOGUARD® as compared with FIT, for the detection of screening-relevant colorectal cancer. The study was conducted at 90 medical centers throughout the United States and Canada and evaluable patients (N=9989) were asymptomatic individuals between ages 50 and 84 years who were required to provide a stool sample and undergo screening colonoscopy within 90 days. Enrollment was weighted toward those aged 65 years or older. The primary outcome was the ability of COLOGUARD® to detect colorectal cancer and secondary outcomes were the ability of COLOGUARD® to detect advanced precancerous lesions, polyps with high grade dysplasia and serrated sessile polyps measuring 1 cm or more, when compared to FIT. (Sensitivity is defined as the proportion of persons with disease who have a positive test and Specificity is defined as proportion of persons without disease who have a negative test.) The sensitivity for detecting colorectal cancer was 92% with COLOGUARD® and 74% with FIT (P=0.002). The sensitivity for detecting advanced precancerous lesions was 42.4% vs 23.8% (P<0.001), polyps with high-grade dysplasia was 69.2% vs 46.2% (P=0.004) and serrated sessile polyps measuring 1 cm or more were 42.4% vs 5.1%, (P<0.001) with COLOGUARD® and FIT respectively. Specificities with COLOGUARD® were lower compared to FIT (P<0.001). The authors concluded that COLOGUARD® can detect significantly more colorectal cancers and precancerous lesions than FIT. The high sensitivity of this non-invasive, stool DNA test, to detect curable stage of colorectal cancer, may increase the number of people, who will choose to be screened for colorectal cancer. Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. N Engl J Med 2014; 370:1287-1297
COLOGUARD® is highly sensitive, noninvasive, multitarget, stool based DNA test, for colorectal cancer screening ie.early detection of colorectal cancer and precancerous lesions. This test takes advantage of the genetic and epigenetic alterations that leads to the development of colorectal cancer and analyzes the altered DNA signatures of cancerous and precancerous cells that exfoliate into the colon. In addition, this test includes an immunochemical assay for human hemoglobin. The stool samples can be easily collected, mailed from home, and requires no bowel preparation, medication restrictions or dietary change. The purpose of this study was to determine the sensitivity of COLOGUARD® as compared with FIT, for the detection of screening-relevant colorectal cancer. The study was conducted at 90 medical centers throughout the United States and Canada and evaluable patients (N=9989) were asymptomatic individuals between ages 50 and 84 years who were required to provide a stool sample and undergo screening colonoscopy within 90 days. Enrollment was weighted toward those aged 65 years or older. The primary outcome was the ability of COLOGUARD® to detect colorectal cancer and secondary outcomes were the ability of COLOGUARD® to detect advanced precancerous lesions, polyps with high grade dysplasia and serrated sessile polyps measuring 1 cm or more, when compared to FIT. (Sensitivity is defined as the proportion of persons with disease who have a positive test and Specificity is defined as proportion of persons without disease who have a negative test.) The sensitivity for detecting colorectal cancer was 92% with COLOGUARD® and 74% with FIT (P=0.002). The sensitivity for detecting advanced precancerous lesions was 42.4% vs 23.8% (P<0.001), polyps with high-grade dysplasia was 69.2% vs 46.2% (P=0.004) and serrated sessile polyps measuring 1 cm or more were 42.4% vs 5.1%, (P<0.001) with COLOGUARD® and FIT respectively. Specificities with COLOGUARD® were lower compared to FIT (P<0.001). The authors concluded that COLOGUARD® can detect significantly more colorectal cancers and precancerous lesions than FIT. The high sensitivity of this non-invasive, stool DNA test, to detect curable stage of colorectal cancer, may increase the number of people, who will choose to be screened for colorectal cancer. Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. N Engl J Med 2014; 370:1287-1297
Deep Molecular Response Is Reached by the Majority of Patients Treated With Imatinib, Predicts Survival, and Is Achieved More Quickly by Optimized High-Dose Imatinib Results From the Randomized CML-Study IV
SUMMARY:Chronic Myeloid Leukemia (CML) constitutes approximately 10% of all new cases of leukemia. The American Cancer Society estimates that 5,980 new CML cases will be diagnosed in the United States in 2014 and 810 people will die of the disease. The hallmark of CML, the Philadelphia Chromosome (Chromosome 22), is a result of a reciprocal translocation between chromosomes 9 and 22, wherein the ABL gene from chromosome 9 fuses with the BCR gene on chromosome 22. As a result, the auto inhibitory function of the ABL gene is lost and the BCR-ABL fusion gene is activated resulting in cell proliferation and leukemic transformation of hematopoietic stem cells. The presently available Tyrosine Kinase Inhibitors (TKI’s) approved in the United States including GLEEVEC®, share the same therapeutic target, which is BCR-ABL kinase. Resistance to TKI’s occur as a result of mutations in the BCR-ABL kinase domain or amplification of the BCR-ABL gene. With the availability of newer therapies for CML, monitoring response to treatment is important. This is best accomplished by measuring the amount of residual disease using Reverse Transcription-Polymerase Chain Reaction (RT-PCR).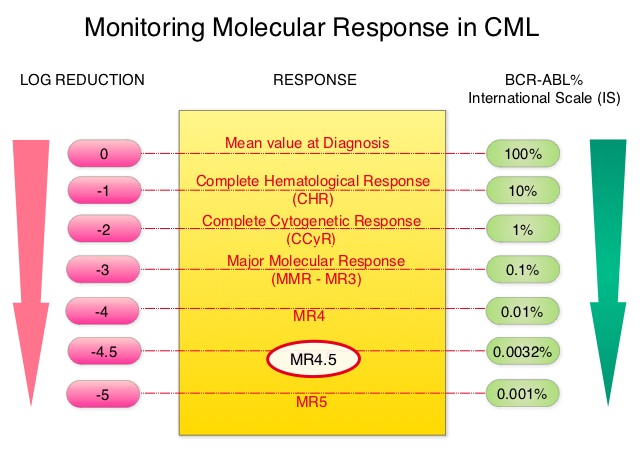 This is expressed using the International Scale (IS) as BCR-ABL%, which is the ratio between BCR-ABL and a control gene. BCR-ABL kinase domain point mutations are detected, using the mutational analysis by Sanger sequencing. Majority of the patients receiving a TKI following diagnosis of CML achieve a Complete Cytogenetic Response (CCyR) within 12 months following commencement of therapy and these patients have a life expectancy similar to that of their healthy counterparts. However, some patients have deeper responses (MR3, MR4, and MR4.5) and it is presumed that this subgroup of patients with CML may stay in unmaintained remission even after treatment discontinuation. Moreover, it is not clear what proportion of patients with CML achieve deeper responses and deeper responses have not been shown to increase survival beyond that associated with CCyR. To address these questions, the authors in this report analyzed the data from the randomized CML – Study IV to characterize the frequency and impact of deep molecular response on survival with different treatment modalities. The study is a five arm trial in which the treatment groups included high dose Imatinib (GLEEVEC® 800 mg/day), GLEEVEC® 400 mg/day, GLEEVEC® 400 mg/day in combination with Interferon alfa (IFN), GLEEVEC® 400 mg/day in combination with Cytarabine, and GLEEVEC® 400 mg/day after IFN failure. The analysis included a total of 1538 patients and the principal objective of CML – Study IV was to determine the impact of MMR (Major Molecular Response) on survival, remission rates and survival probabilities. After a median follow up of 67.5 months, 5 year overall survival was 90%, 8 year overall survival was 86% and 5 year PFS was 87.5%. The cumulative rate of MR4.5, irrespective of treatment group (defined as 4.5 or more log reduction in BCR-ABL transcripts), was 66% at 8 years and 70% at 9 years and the median time to reaching MR4.5 was 4.9 years. High dose GLEEVEC® therapy and early Major Molecular Remission predicted deep molecular response (MR4.5). High dose GLEEVEC® resulted in a more rapid MR4.5 than with GLEEVEC® 400 mg/day (P = .016). Finally, this analysis showed that a confirmed MR4.5 at 4 years predicted significantly higher 8 year overall survival probability compared to CCyR (Complete Cytogenetic response: IS 1%) or MMR (major molecular response: IS 0.1%) – 92% versus 83%, P=0.047. The authors concluded that deep molecular response (MR4.5) is a new molecular predictor of long term survival in CML patients and is achieved in a majority of patients treated with GLEEVEC®, and is achieved more rapidly with optimized high-dose GLEEVEC®. The authors further pointed out that none of the patients with confirmed MR4.5 had disease progression and this may therefore provide a therapeutic rationale for discontinuing treatment in this subset of patients with CML. These findings may also justify the use of more effective second generation TKI’s to induce early and deep molecular responses. Hehlmann R, Müller MC, Lauseker M, et al. J Clin Oncol 2014;32:415-423
This is expressed using the International Scale (IS) as BCR-ABL%, which is the ratio between BCR-ABL and a control gene. BCR-ABL kinase domain point mutations are detected, using the mutational analysis by Sanger sequencing. Majority of the patients receiving a TKI following diagnosis of CML achieve a Complete Cytogenetic Response (CCyR) within 12 months following commencement of therapy and these patients have a life expectancy similar to that of their healthy counterparts. However, some patients have deeper responses (MR3, MR4, and MR4.5) and it is presumed that this subgroup of patients with CML may stay in unmaintained remission even after treatment discontinuation. Moreover, it is not clear what proportion of patients with CML achieve deeper responses and deeper responses have not been shown to increase survival beyond that associated with CCyR. To address these questions, the authors in this report analyzed the data from the randomized CML – Study IV to characterize the frequency and impact of deep molecular response on survival with different treatment modalities. The study is a five arm trial in which the treatment groups included high dose Imatinib (GLEEVEC® 800 mg/day), GLEEVEC® 400 mg/day, GLEEVEC® 400 mg/day in combination with Interferon alfa (IFN), GLEEVEC® 400 mg/day in combination with Cytarabine, and GLEEVEC® 400 mg/day after IFN failure. The analysis included a total of 1538 patients and the principal objective of CML – Study IV was to determine the impact of MMR (Major Molecular Response) on survival, remission rates and survival probabilities. After a median follow up of 67.5 months, 5 year overall survival was 90%, 8 year overall survival was 86% and 5 year PFS was 87.5%. The cumulative rate of MR4.5, irrespective of treatment group (defined as 4.5 or more log reduction in BCR-ABL transcripts), was 66% at 8 years and 70% at 9 years and the median time to reaching MR4.5 was 4.9 years. High dose GLEEVEC® therapy and early Major Molecular Remission predicted deep molecular response (MR4.5). High dose GLEEVEC® resulted in a more rapid MR4.5 than with GLEEVEC® 400 mg/day (P = .016). Finally, this analysis showed that a confirmed MR4.5 at 4 years predicted significantly higher 8 year overall survival probability compared to CCyR (Complete Cytogenetic response: IS 1%) or MMR (major molecular response: IS 0.1%) – 92% versus 83%, P=0.047. The authors concluded that deep molecular response (MR4.5) is a new molecular predictor of long term survival in CML patients and is achieved in a majority of patients treated with GLEEVEC®, and is achieved more rapidly with optimized high-dose GLEEVEC®. The authors further pointed out that none of the patients with confirmed MR4.5 had disease progression and this may therefore provide a therapeutic rationale for discontinuing treatment in this subset of patients with CML. These findings may also justify the use of more effective second generation TKI’s to induce early and deep molecular responses. Hehlmann R, Müller MC, Lauseker M, et al. J Clin Oncol 2014;32:415-423
Clinical validity of circulating tumour cells in patients with metastatic breast cancer a pooled analysis of individual patient data
SUMMARY: Circulating tumor cells (CTCs) are epithelial cells that are shed into the circulation from a primary or metastatic tumor. After being shed, CTCs can remain in the circulation or undergo apoptosis. 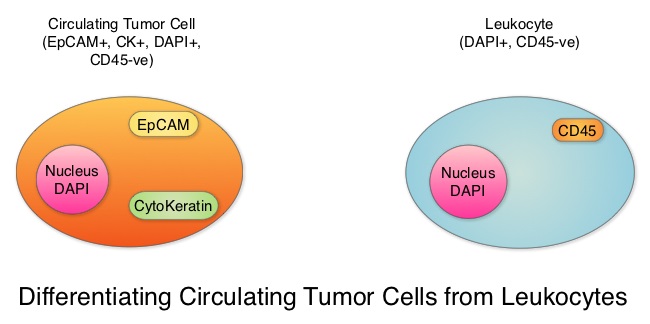 Evaluation of CTCs during the course of disease has prognostic value. Because of the very low concentrations of CTCs (1 CTC in the background of millions of normal hematopoietic cells) in the peripheral blood, different technologies have been developed that will allow enrichment and detection of these CTCs. One such technology is the CellSearch® system which is the first FDA-approved test for CTC assessment, in the peripheral blood of Metastatic Breast Cancer (MBC) patients. This automated system is able to enrich the peripheral blood sample with CTCs and the cells then are fluorescently stained for CytoKeratins (CK8,18 and 19), Common Leukocyte Antigen (CD45) and a nuclear dye (DAPI). CTCs are identified when they are CK positive, CD45 negative and DAPI positive. In essence, CTC assessment is a real time, peripheral blood evaluation (“Liquid Biopsy”) in MBC patients. The authors in this study conducted a pooled analysis to assess the clinical validity of CTCs in patients with MBC, as previously published studies reported contradictory results and were unable to ascertain whether enumeration of CTCs had better prognostic value than the traditional clinical and pathological features of the tumor and serum tumor markers. Data was gathered on 1944 patients with MBC, who had participated in clinical trials at 17 centers between 2003 and 2012. Participants in these studies were starting a new line of therapy (predominantly chemotherapy), and these studies had CTC quantification using CellSearch® platform, before start of new treatment (baseline), data for Progression Free Survival, Overall Survival or both. Using accepted statistical methodologies, the authors noted the following findings-
Evaluation of CTCs during the course of disease has prognostic value. Because of the very low concentrations of CTCs (1 CTC in the background of millions of normal hematopoietic cells) in the peripheral blood, different technologies have been developed that will allow enrichment and detection of these CTCs. One such technology is the CellSearch® system which is the first FDA-approved test for CTC assessment, in the peripheral blood of Metastatic Breast Cancer (MBC) patients. This automated system is able to enrich the peripheral blood sample with CTCs and the cells then are fluorescently stained for CytoKeratins (CK8,18 and 19), Common Leukocyte Antigen (CD45) and a nuclear dye (DAPI). CTCs are identified when they are CK positive, CD45 negative and DAPI positive. In essence, CTC assessment is a real time, peripheral blood evaluation (“Liquid Biopsy”) in MBC patients. The authors in this study conducted a pooled analysis to assess the clinical validity of CTCs in patients with MBC, as previously published studies reported contradictory results and were unable to ascertain whether enumeration of CTCs had better prognostic value than the traditional clinical and pathological features of the tumor and serum tumor markers. Data was gathered on 1944 patients with MBC, who had participated in clinical trials at 17 centers between 2003 and 2012. Participants in these studies were starting a new line of therapy (predominantly chemotherapy), and these studies had CTC quantification using CellSearch® platform, before start of new treatment (baseline), data for Progression Free Survival, Overall Survival or both. Using accepted statistical methodologies, the authors noted the following findings-
1) At baseline prior to starting treatment, 47% (N=911) patients had 5 or more CTCs per 7•5 mL of peripheral blood, suggesting more aggressive disease and this was associated with decreased Progression Free Survival (P<0•0001) and Overall Survival (P<0•0001), compared with patients with less than 5 CTCs per 7•5 mL at baseline.
2) At 3-5 weeks after start of treatment (1-2 cycles of treatment), when adjusted for baseline CTC count, 5 or more CTCs per 7•5 mL of peripheral blood was associated with shortened Progression Free Survival (P<0•0001) and Overall Survival (P<0•0001), suggesting that these patients were treatment resistant.
3) An early decrease in the CTC at week 3-5, from a high baseline of 5 or more CTCs per 7•5 mL to less than 5 CTCs per 7.5 ml was associated with significantly longer Progression Free Survival and Overall Survival.
4) Enumeration of CTCs was a better predictor of prognosis than mucin based serum biomarkers such as CEA and CA15-3.
The prognostic value of high CTC count at baseline and at 3-5 weeks of treatment, on Progression Free Survival and Overall Survival was maintained in all subgroups tested, regardless of breast cancer subtypes and type of therapy patients received. Based on this pooled analysis, with the largest assessment of CTC enumeration in MBC patients, the authors concluded that CTC count can prognosticate Progression Free Survival and Overall Survival early in the treatment course, allowing customized care. Further, CTC enumeration, unlike serum tumor markers, correlates with clinical and pathological characteristics. Bidard F, Peeters DJ, Fehm T, et al. The Lancet Oncology 2014;15:406-414
CD49d Is the Strongest Flow Cytometry–Based Predictor of Overall Survival in Chronic Lymphocytic Leukemia
SUMMARY:The American Cancer Society's estimates that approximately 15,720 new cases of chronic lymphocytic leukemia (CLL) will be diagnosed in 2014 and approximately 4600 patients will die from the disease. CLL is a heterogeneous disease with a clinical course that is variable, with a very indolent course in some patients and some with aggressive disease and others somewhere in between. Both Binet and the Rai CLL staging systems developed in the 1970’s rely solely on physical examination and standard laboratory testing to predict survival. With the development of Interphase Fluorescent In Situ Hybridization (FISH) technique, which allows detection of genetic abnormalities in noncycling CLL cells, it has become clear that cytogenetic abnormalities are often seen in CLL patients and these genetic abnormalities in turn appear to be reliable predictors of disease progression, response to therapy and survival. Some of these cytogenetic abnormalities include del(13q), normal karyotype, trisomy(12), del(11q), del(17p), and they are associated with decreasing survival times, in that order. Another important prognostic factor is the rearrangement and somatic hypermutation of the variable region of the immunoglobulin heavy chain genes (IGHV), which is an independent predictor of outcome in CLL.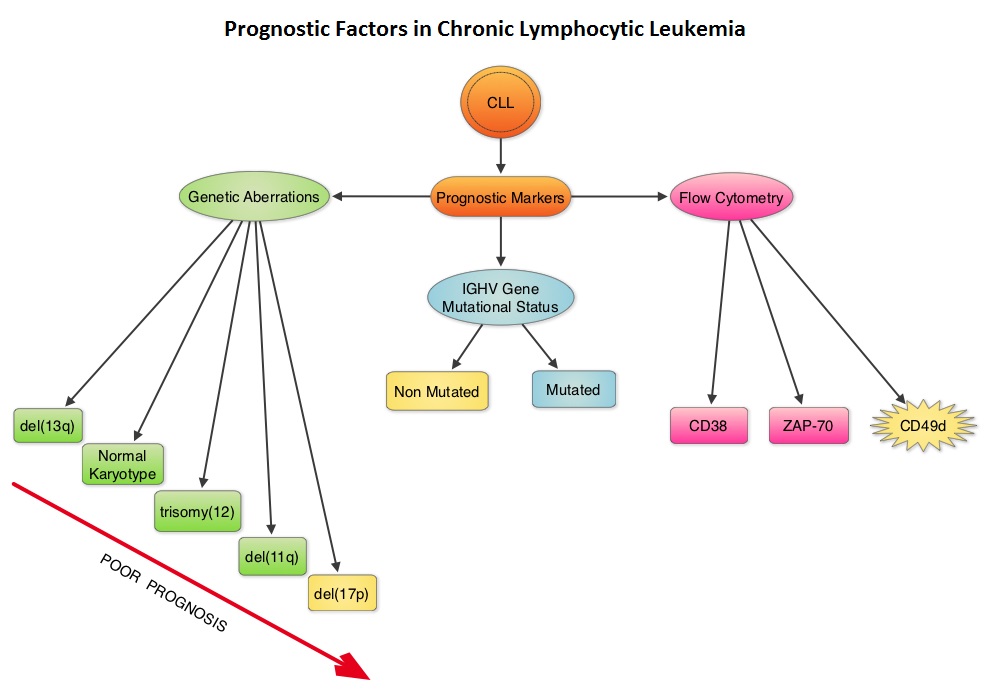 Retrospective studies have suggested that patients with CLL whose leukemic cells have clonotypically rearranged immunoglobulin genes in germline configuration (Unmutated IGHV gene) demonstrated more aggressive disease and shorter survival time compared to those patients with somatic hypermutations in their IGHV genes (Mutated IGHV gene). Expression of two flow cytometry based biomarkers, CD38 (surface marker) and ZAP-70 (intracytoplasmic protein), have been associated with poor outcomes. As we learn more about the pathobiology of CLL, it is becoming clear that survival of CLL cells is dependent not only on their intracellular defects but also on the microenvironment. CD49d, an integrin, is a surface molecule, detected by flow cytometry. CD49d expression promotes microenvironment mediated proliferation of CLL cells and has been associated with shortened survival. The authors conducted this multicenter analysis to evaluate the prognostic utility of CD49d in CLL, in comparison with CD38 and ZAP-70. The authors analysed the data of 2972 patients from 9 clinical trials. All these studies had data on CD49d expression of CLL cells by flow cytometry and reported the association between CD49d expression and Overall survival and/or Treatment Free Survival and/or Progression Free Survival. Patients with 30% or more of CLL cells expressing CD49d were considered CD49d positive. In this pooled analysis, CD49d positive patients had a significantly lower Overall Survival both at 5 years (87% vs 94%) and 10 years (62% vs 84%) compared with CD49d negative patients (P<0.001). Further, CD49d positive patients more likely required treatment, suggesting that these patients had a lower probability of remaining treatment free at both 5 years (42% vs 68%) and 10 years (24% vs 50%), compared with CD49d negative patients. When other variables were taken into consideration, CD49d was the only flow cytometry based marker which independently predicted Overall Survival with greater prognostic relevance than CD38 and ZAP-70. The authors concluded that CD49d expression and IGHV gene mutational status may be the strongest predictors of Overall Survival and Treatment Free Survival in patients with CLL and should be a part of routine baseline testing at the time of diagnosis. Bulian P, Shanafelt TD, Fegan C, et al. J Clin Oncol 2014;32:897-904
Retrospective studies have suggested that patients with CLL whose leukemic cells have clonotypically rearranged immunoglobulin genes in germline configuration (Unmutated IGHV gene) demonstrated more aggressive disease and shorter survival time compared to those patients with somatic hypermutations in their IGHV genes (Mutated IGHV gene). Expression of two flow cytometry based biomarkers, CD38 (surface marker) and ZAP-70 (intracytoplasmic protein), have been associated with poor outcomes. As we learn more about the pathobiology of CLL, it is becoming clear that survival of CLL cells is dependent not only on their intracellular defects but also on the microenvironment. CD49d, an integrin, is a surface molecule, detected by flow cytometry. CD49d expression promotes microenvironment mediated proliferation of CLL cells and has been associated with shortened survival. The authors conducted this multicenter analysis to evaluate the prognostic utility of CD49d in CLL, in comparison with CD38 and ZAP-70. The authors analysed the data of 2972 patients from 9 clinical trials. All these studies had data on CD49d expression of CLL cells by flow cytometry and reported the association between CD49d expression and Overall survival and/or Treatment Free Survival and/or Progression Free Survival. Patients with 30% or more of CLL cells expressing CD49d were considered CD49d positive. In this pooled analysis, CD49d positive patients had a significantly lower Overall Survival both at 5 years (87% vs 94%) and 10 years (62% vs 84%) compared with CD49d negative patients (P<0.001). Further, CD49d positive patients more likely required treatment, suggesting that these patients had a lower probability of remaining treatment free at both 5 years (42% vs 68%) and 10 years (24% vs 50%), compared with CD49d negative patients. When other variables were taken into consideration, CD49d was the only flow cytometry based marker which independently predicted Overall Survival with greater prognostic relevance than CD38 and ZAP-70. The authors concluded that CD49d expression and IGHV gene mutational status may be the strongest predictors of Overall Survival and Treatment Free Survival in patients with CLL and should be a part of routine baseline testing at the time of diagnosis. Bulian P, Shanafelt TD, Fegan C, et al. J Clin Oncol 2014;32:897-904
Gaps in Pre-rituximab Hepatitis B Screening An Institutional Experience
SUMMARY:The Centers for Disease Control and Prevention (CDC) estimates that there are 800,000 -1.4 million individuals with Chronic Hepatitis B infection in the United States. Reactivation of HBV is a major concern in cancer patients who may be on chemotherapy or other immunosuppressive therapies, with the incidence of HBV reactivation ranging from 40%-60% in those who are positive for Hepatitis B surface antigen (HBsAg). HBV reactivation is preventable with prophylactic antiviral therapy, failing which it can result in delays in cancer treatment as well as potentially fatal outcomes.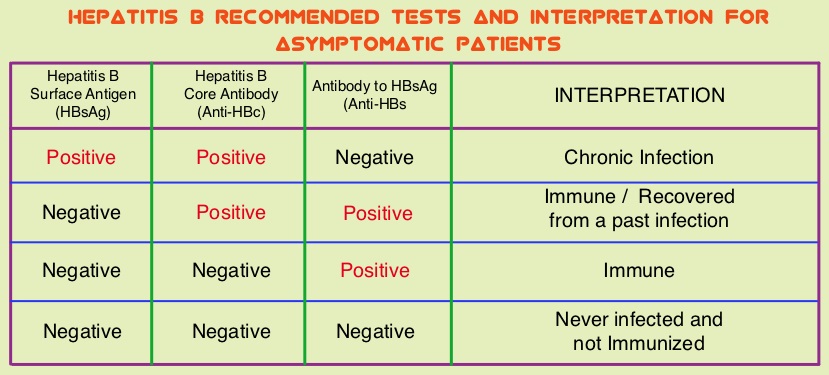 The CDC updated their recommendations in 2008 and recommended HBV screening for patients receiving cytotoxic chemotherapy or immunotherapy. The American Society of Clinical Oncology in 2010 rendered a Provisional Clinical Opinion (PCO) suggesting that there was insufficient evidence to recommend routine screening for HBV in cancer patients,but screening may be considered for patient populations at high risk or for those who are to receive highly immunosuppressive therapies including anti-CD20 monoclonal antibody therapy such as Rituximab (RITUXAN®). To evaluate compliance with these recommendations, the authors in this study retrospectively reviewed charts of patients with Low grade Non Hodgkins Lymphoma at a teritiary care center and documented the various studies performed, as a part of the pretreatment workup, between January 2005 and December 2011. They noted that only 19% of the total patients and 25% of the patients who received RITUXAN® had HBV screening done. The authors concluded that this was a significant deviation from the recommended guidelines and these findings resulted in the implementation of stricter measures for HBV screening at this teritiary care center. Screening for HBV should include testing for Hepatitis B surface antigen (HBsAg), Antibody to Hepatitis B core antigen (anti-HBc) and Antibody to Hepatitis B surface antigen (Anti-HBs). Patients positive for HBsAg and anti-HBc as well as those who are negative for HBsAg and positive for anti-HBc, should have testing for HBV viral load using serum HBV DNA and those without active disease should receive prophylactic antiviral therapy and be closely monitored for HBV reactivation. Prophylaxis is usually started one week before initiating chemotherapy and continued for at least 6 months after completion of chemotherapy, although the actual duration of prophylactic antiviral therapy remains unclear. If HBV reactivation is noted, chemotherapy should be immediately discontinued. Given the prevalence of chronic Hepatitis B in the United States, screening for HBV should become a routine part of pretreatment evaluation in cancer patients. Abbi KK, Gorris M, Skeel RT. Am J Ther. 2013;June 28.
The CDC updated their recommendations in 2008 and recommended HBV screening for patients receiving cytotoxic chemotherapy or immunotherapy. The American Society of Clinical Oncology in 2010 rendered a Provisional Clinical Opinion (PCO) suggesting that there was insufficient evidence to recommend routine screening for HBV in cancer patients,but screening may be considered for patient populations at high risk or for those who are to receive highly immunosuppressive therapies including anti-CD20 monoclonal antibody therapy such as Rituximab (RITUXAN®). To evaluate compliance with these recommendations, the authors in this study retrospectively reviewed charts of patients with Low grade Non Hodgkins Lymphoma at a teritiary care center and documented the various studies performed, as a part of the pretreatment workup, between January 2005 and December 2011. They noted that only 19% of the total patients and 25% of the patients who received RITUXAN® had HBV screening done. The authors concluded that this was a significant deviation from the recommended guidelines and these findings resulted in the implementation of stricter measures for HBV screening at this teritiary care center. Screening for HBV should include testing for Hepatitis B surface antigen (HBsAg), Antibody to Hepatitis B core antigen (anti-HBc) and Antibody to Hepatitis B surface antigen (Anti-HBs). Patients positive for HBsAg and anti-HBc as well as those who are negative for HBsAg and positive for anti-HBc, should have testing for HBV viral load using serum HBV DNA and those without active disease should receive prophylactic antiviral therapy and be closely monitored for HBV reactivation. Prophylaxis is usually started one week before initiating chemotherapy and continued for at least 6 months after completion of chemotherapy, although the actual duration of prophylactic antiviral therapy remains unclear. If HBV reactivation is noted, chemotherapy should be immediately discontinued. Given the prevalence of chronic Hepatitis B in the United States, screening for HBV should become a routine part of pretreatment evaluation in cancer patients. Abbi KK, Gorris M, Skeel RT. Am J Ther. 2013;June 28.
15-year post-treatment follow-up of radium-223 dichloride (Ra-223) in patients with castration-resistant prostate cancer (CRPC) and bone metastases from the phase 3 ALSYMPCA study
SUMMARY: Prostate cancer is the most common cancer in American men, excluding skin cancer and 1 in 7 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, over 230,000 new cases of prostate cancer will be diagnosed in 2014 and close to 30,000 men will die of the disease. Over 90% of the patients with metastatic prostate cancer have bone metastases, and the tumor burden, is an independent predictor of death in this patient population. Agents such as ZOMETA® and XGEVA® can prevent or delay Skeletal Related Events (SRE’s) and External Beam Radiation Therapy (EBRT) is often utilized to treat symptomatic SRE’s. EBRT can however damage the bone marrow in the radiated field, resulting in cytopenias, and consequently can potentially preclude patients from receiving cytotoxic chemotherapy.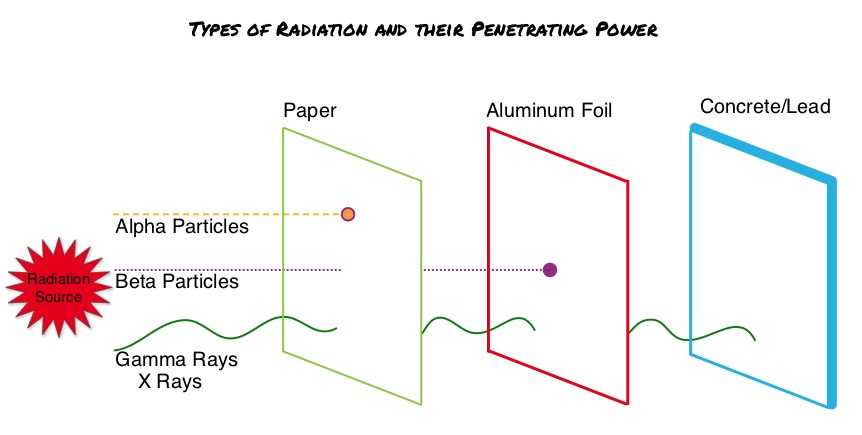 Radium Ra 223 dichloride (XOFIGO®) is a bone seeking alpha particle emitter and by virtue of its chemical similarity to calcium is preferentially taken up by the bone and forms complexes with bone mineral, hydroxyapatite, in areas where there is increased bone turnover, such as bone metastases. XOFIGO® induces double stranded DNA breaks resulting in antitumor effects and has a very short range in tissues (around 2 and 10 cells), quickly losing energy, compared to beta or gamma radiation. The end result is less damage to the adjacent healthy tissues. Further, unlike Ra-226 which was first isolated by Madame Curie, XOFIGO® has a short half life of 11.4 days and rapidly decays, preventing significant radiation exposure. The ALSYMPCA (ALpharadin in SYMptomatic Prostate CAncer patients) study is a randomized, double-blind, phase III trial, in which 921 patients with Castrate Resistant Prostate Cancer (CRPC) with 2 or more symptomatic bone metastases and no known visceral metastases, were randomly assigned in a 2:1 ratio to receive either XOFIGO® along with best supportive care (N=614) or placebo with best supportive care (N=307). Enrolled patients either progressed on or had not received TAXOTERE® (Docetaxel) for a variety of reasons and 42% of the enrolled patients were chemotherapy naïve.
Radium Ra 223 dichloride (XOFIGO®) is a bone seeking alpha particle emitter and by virtue of its chemical similarity to calcium is preferentially taken up by the bone and forms complexes with bone mineral, hydroxyapatite, in areas where there is increased bone turnover, such as bone metastases. XOFIGO® induces double stranded DNA breaks resulting in antitumor effects and has a very short range in tissues (around 2 and 10 cells), quickly losing energy, compared to beta or gamma radiation. The end result is less damage to the adjacent healthy tissues. Further, unlike Ra-226 which was first isolated by Madame Curie, XOFIGO® has a short half life of 11.4 days and rapidly decays, preventing significant radiation exposure. The ALSYMPCA (ALpharadin in SYMptomatic Prostate CAncer patients) study is a randomized, double-blind, phase III trial, in which 921 patients with Castrate Resistant Prostate Cancer (CRPC) with 2 or more symptomatic bone metastases and no known visceral metastases, were randomly assigned in a 2:1 ratio to receive either XOFIGO® along with best supportive care (N=614) or placebo with best supportive care (N=307). Enrolled patients either progressed on or had not received TAXOTERE® (Docetaxel) for a variety of reasons and 42% of the enrolled patients were chemotherapy naïve.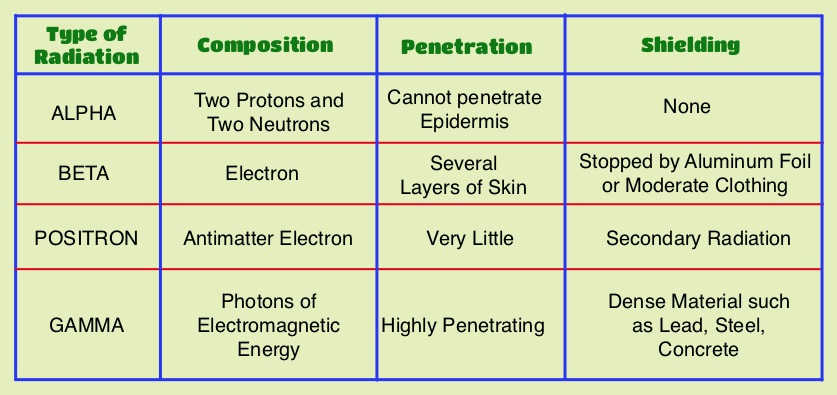 The primary endpoint was Overall Survival and secondary endpoints included time to first symptomatic skeletal event, time to increase in total alkaline phosphatase level and PSA level. This study was stopped earlier than planned, as there was a significant increase in the median overall survival in the XOFIGO® group compared to placebo group, with a 30% reduction in the risk of death (14.9 months vs 11.3 months, HR=0.70, P<0.001). All secondary endpoints favored XOFIGO® as well. The most common adverse events were cytopenias, majority of which were Grades 1 and 2 and discontinuation rates due to adverse events were lower in the XOFIGO® group (17%) compared to 21% for the Placebo group. At 1.5 years, the incidence of myelosuppression was 3%, there were no grade 3 or 4 non-hematologic toxicities and no reports of secondary malignancies in the XOFIGO® group. The authors concluded that based on the long term safety data, XOFIGO® has an excellent side-effect profile in patients with CRPC. Unlike the bone seeking beta emitters such as Strontium-89 and Samarium-153, XOFIGO®, an alpha emitter, is the only agent that has been shown to improve overall survival. Studies are underway evaluating the efficacy of chemotherapy in combination with XOFIGO®, in patients with CRPC and associated bone metastases. Nilsson S, Vogelzang NJ, Sartor AO, et al. J Clin Oncol 32, 2014 (suppl 4; abstr 9)
The primary endpoint was Overall Survival and secondary endpoints included time to first symptomatic skeletal event, time to increase in total alkaline phosphatase level and PSA level. This study was stopped earlier than planned, as there was a significant increase in the median overall survival in the XOFIGO® group compared to placebo group, with a 30% reduction in the risk of death (14.9 months vs 11.3 months, HR=0.70, P<0.001). All secondary endpoints favored XOFIGO® as well. The most common adverse events were cytopenias, majority of which were Grades 1 and 2 and discontinuation rates due to adverse events were lower in the XOFIGO® group (17%) compared to 21% for the Placebo group. At 1.5 years, the incidence of myelosuppression was 3%, there were no grade 3 or 4 non-hematologic toxicities and no reports of secondary malignancies in the XOFIGO® group. The authors concluded that based on the long term safety data, XOFIGO® has an excellent side-effect profile in patients with CRPC. Unlike the bone seeking beta emitters such as Strontium-89 and Samarium-153, XOFIGO®, an alpha emitter, is the only agent that has been shown to improve overall survival. Studies are underway evaluating the efficacy of chemotherapy in combination with XOFIGO®, in patients with CRPC and associated bone metastases. Nilsson S, Vogelzang NJ, Sartor AO, et al. J Clin Oncol 32, 2014 (suppl 4; abstr 9)
Nonleg venous thrombosis in critically ill adults a nested prospective cohort study
SUMMARY: The CDC estimates that approximately 1-2 per 1000 individuals develop Deep Vein Thrombosis/Pulmonary Embolism (PE) each year in the United States, resulting in 60,000-100,000 deaths. Even though Deep Vein Thrombosis (DVT) commonly occurs in the lower extremities, Non-Leg Deep Venous Thromboses (NLDVT) at other sites including the head and neck, trunk, and upper extremities can occur. The incidence, risk factors, management and outcomes in this patient group remains unclear. The authors therefore conducted a prospective cohort study in the ICU setting. This study is nested in a larger international trial in which 3746 patients, expected to remain in the med/surg Intensive Care Unit (ICU) for at least 3 days, were randomized to receive either Unfractionated (standard) heparin or Dalteparin (FRAGMIN®) for thromboprophylaxis.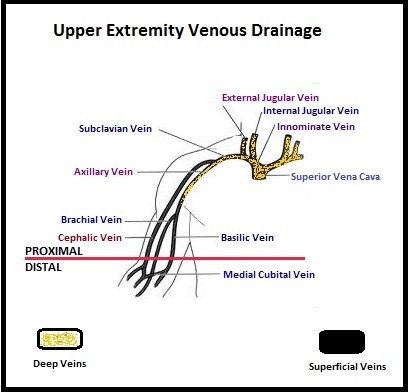 The authors characterized the NLDVT as Prevalent or Incident (depending on whether the thrombosis was identified within 72 hours of ICU admission or developed after the third ICU day) and whether they were catheter related or not. Risk factors for NLDVT and subsequent anticoagulant therapy, associated PE, and death were evaluated. Several important findings were noted from this study. Of the 3746 patients, 2.2% developed 1 or more Non-Leg Vein Thromboses (superficial or deep, proximal or distal). Majority of these thrombotic events (95%) occurred in the upper extremity and most of these occurred in the clinically important proximal and deep venous system. Further, these thrombotic episodes were more commonly Incident (2.0%) rather than Prevalent (0.2%) – P <0.001. It was noted that 1 in 7 patients with NLDVT developed PE. It appears that malignancy, hospitalization and Central Venous Catheters are risk factors for Upper Extremity Deep Vein Thrombosis (UEDVT), but the disproportionate increase in the incidence of UEDVT in hospitalized patients (30%-40% of hospital associated DVT’s) has been attributed to the increased use of CVC’s such as PICC (Peripherally Inserted Central Catheter). In this study, only 13% of the patients diagnosed with NLDVT received anticoagulation therapy. In an accompanying commentary by Dr. Greg Maynard, it was well pointed out that UEDVT is associated with similar rates of recurrence, PE and mortality as lower extremity DVT and as such UEDVT should be treated with anticoagulant therapy similar to Lower Extremity DVT. Dr. Maynard also noted that PICC associated DVT could be significantly reduced by appropriately choosing patients for a PICC line, proper PICC placement, early PICC removal, smaller diameter PICC and smaller number of lumens in the catheter. The authors concluded that despite universal prophylaxis with heparin, there was a high incidence of NLDVT in clinically important locations of the venous system, in critically ill patients and this calls for more structured preventive measures, as we learn more about this entity. Lamontagne F, McIntyre L, Dodek P, et al. JAMA Intern Med. 2014;174:689-696
The authors characterized the NLDVT as Prevalent or Incident (depending on whether the thrombosis was identified within 72 hours of ICU admission or developed after the third ICU day) and whether they were catheter related or not. Risk factors for NLDVT and subsequent anticoagulant therapy, associated PE, and death were evaluated. Several important findings were noted from this study. Of the 3746 patients, 2.2% developed 1 or more Non-Leg Vein Thromboses (superficial or deep, proximal or distal). Majority of these thrombotic events (95%) occurred in the upper extremity and most of these occurred in the clinically important proximal and deep venous system. Further, these thrombotic episodes were more commonly Incident (2.0%) rather than Prevalent (0.2%) – P <0.001. It was noted that 1 in 7 patients with NLDVT developed PE. It appears that malignancy, hospitalization and Central Venous Catheters are risk factors for Upper Extremity Deep Vein Thrombosis (UEDVT), but the disproportionate increase in the incidence of UEDVT in hospitalized patients (30%-40% of hospital associated DVT’s) has been attributed to the increased use of CVC’s such as PICC (Peripherally Inserted Central Catheter). In this study, only 13% of the patients diagnosed with NLDVT received anticoagulation therapy. In an accompanying commentary by Dr. Greg Maynard, it was well pointed out that UEDVT is associated with similar rates of recurrence, PE and mortality as lower extremity DVT and as such UEDVT should be treated with anticoagulant therapy similar to Lower Extremity DVT. Dr. Maynard also noted that PICC associated DVT could be significantly reduced by appropriately choosing patients for a PICC line, proper PICC placement, early PICC removal, smaller diameter PICC and smaller number of lumens in the catheter. The authors concluded that despite universal prophylaxis with heparin, there was a high incidence of NLDVT in clinically important locations of the venous system, in critically ill patients and this calls for more structured preventive measures, as we learn more about this entity. Lamontagne F, McIntyre L, Dodek P, et al. JAMA Intern Med. 2014;174:689-696
Bevacizumab Combined With Chemotherapy for Platinum-Resistant Recurrent Ovarian Cancer The AURELIA Open-Label Randomized Phase III Trial
SUMMARY: It is estimated that in the United States, approximately 22,000 women will be diagnosed with ovarian cancer in 2014 and a little over 14,000 women will die of the disease. In spite of significantly improved median survival following aggressive surgical debulking and platinum plus taxane based therapy, long term cure rate is approximately 20-30%. Majority of the patients relapse in 18-24 months and 25% of these patients are Platinum Resistant. These platinum resistant patients are usually treated with single agent chemotherapy drugs such as DOXIL® (Pegylated Liposomal Doxorubicin-PLD), TAXOL® (Paclitaxel) and HYCAMTIN® (Topotecan), with an expected response rate of 10-15%, median response duration of about 3-4 months and median Overall Survival of approximately 12 months. AURELIA (Avastin Use in Platinum-Resistant Epithelial Ovarian Cancer) is a multicenter, randomized, open-label, Phase III study in which 361 women with platinum resistant recurrent epithelial ovarian, primary peritoneal or fallopian tube cancer were enrolled. These patients had disease progression within six months of their platinum based chemotherapy (Platinum Resistant) and were randomly assigned to receive AVASTIN® (Bevacizumab) 10 mg/kg every 2 weeks or 15 mg/kg every 3 weeks in combination with investigators choice of single agent chemotherapy agent such as weekly TAXOL®, HYCAMTIN®, DOXIL® (N=179) or single agent chemotherapy alone (N=182). Patients with refractory disease, history of bowel obstruction, or those who had received two or more prior anticancer regimens were excluded. Treatment was given until disease progression. Patients who had progressed on single agent chemotherapy were allowed to cross over to single agent AVASTIN®. The primary end point was Progression Free Survival (PFS) and secondary end points included Objective Response Rate (ORR), Overall Survival (OS), safety, and patient reported outcomes. The combination of AVASTIN® plus chemotherapy resulted in a 52% reduction in the risk of progression compared to those who received chemotherapy alone, with a median PFS of 6.7 months for the AVASTIN® plus chemotherapy group vs 3.4 months for the single agent chemotherapy group (HR=0.48, P<0.001) and thus met the primary endpoint of this clinical trial. This PFS benefit was seen consistently across all subgroups including the subgroup of patients with ascites. The ORR was 27.3% with the AVASTIN® combination vs 11.8% with single agent chemotherapy (P =0.001). The median OS was 16.6 months for the AVASTIN® combination vs 13.3 months for the single agent chemotherapy group (HR=0.85; P < .17). The lack of statistical significance in the OS has been attributed to cross over of 40% of patients, initially randomized to the chemotherapy alone group, who upon progression, received single agent AVASTIN®. As expected, grade 2 or more hypertension and proteinuria were common in the AVASTIN® group and GI perforation occurred in 2.2% of these patients. There was a 15% improvement in abdominal and GI symptoms as reported by patients, with the AVASTIN® combination, compared to chemotherapy alone. The authors concluded that AVASTIN® in combination with chemotherapy significantly improved Progression Free Survival and Objective Response Rates in patients with Platinum Resistant recurrent Ovarian Cancer. Pujade-Lauraine E, Hilpert F, Weber B, et al. J Clin Oncol 2014;32:1302-1308
AURELIA (Avastin Use in Platinum-Resistant Epithelial Ovarian Cancer) is a multicenter, randomized, open-label, Phase III study in which 361 women with platinum resistant recurrent epithelial ovarian, primary peritoneal or fallopian tube cancer were enrolled. These patients had disease progression within six months of their platinum based chemotherapy (Platinum Resistant) and were randomly assigned to receive AVASTIN® (Bevacizumab) 10 mg/kg every 2 weeks or 15 mg/kg every 3 weeks in combination with investigators choice of single agent chemotherapy agent such as weekly TAXOL®, HYCAMTIN®, DOXIL® (N=179) or single agent chemotherapy alone (N=182). Patients with refractory disease, history of bowel obstruction, or those who had received two or more prior anticancer regimens were excluded. Treatment was given until disease progression. Patients who had progressed on single agent chemotherapy were allowed to cross over to single agent AVASTIN®. The primary end point was Progression Free Survival (PFS) and secondary end points included Objective Response Rate (ORR), Overall Survival (OS), safety, and patient reported outcomes. The combination of AVASTIN® plus chemotherapy resulted in a 52% reduction in the risk of progression compared to those who received chemotherapy alone, with a median PFS of 6.7 months for the AVASTIN® plus chemotherapy group vs 3.4 months for the single agent chemotherapy group (HR=0.48, P<0.001) and thus met the primary endpoint of this clinical trial. This PFS benefit was seen consistently across all subgroups including the subgroup of patients with ascites. The ORR was 27.3% with the AVASTIN® combination vs 11.8% with single agent chemotherapy (P =0.001). The median OS was 16.6 months for the AVASTIN® combination vs 13.3 months for the single agent chemotherapy group (HR=0.85; P < .17). The lack of statistical significance in the OS has been attributed to cross over of 40% of patients, initially randomized to the chemotherapy alone group, who upon progression, received single agent AVASTIN®. As expected, grade 2 or more hypertension and proteinuria were common in the AVASTIN® group and GI perforation occurred in 2.2% of these patients. There was a 15% improvement in abdominal and GI symptoms as reported by patients, with the AVASTIN® combination, compared to chemotherapy alone. The authors concluded that AVASTIN® in combination with chemotherapy significantly improved Progression Free Survival and Objective Response Rates in patients with Platinum Resistant recurrent Ovarian Cancer. Pujade-Lauraine E, Hilpert F, Weber B, et al. J Clin Oncol 2014;32:1302-1308