SUMMARY: The American Cancer Society estimates that in 2026, about 79,320 people will be diagnosed with Non Hodgkin Lymphoma (NHL) in the United States and about 19,970 individuals will die of this disease. Diffuse Large B-Cell Lymphoma (DLBCL) is the most common of the aggressive Non-Hodgkin lymphomas in the United States and more than 25,000 cases of DLBCL are diagnosed each year in the United States, accounting for more than 25 percent of all lymphoma cases. The incidence has steadily increased 3-4% each year. More than half of patients are 65 or older at the time of diagnosis and the incidence is likely to increase with aging of the American population.
Background
DLBCL is a neoplasm of large B cells and the most common chromosome abnormality involves alterations of the BCL-6 gene at the 3q27 locus, which is critical for germinal center formation. Two major molecular subtypes of DLBCL arising from different genetic mechanisms have been identified, using Gene Expression Profiling: Germinal Center B-cell-like (GCB) and Activated B-Cell-like (ABC). Patients in the GCB subgroup have a higher 5-year survival rate, independent of clinical IPI (International Prognostic Index) risk score, whereas patients in the ABC subgroup have a significantly worse outcome. Regardless of molecular subtype, R-CHOP regimen (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone), given every 21 days, for 6 cycles, delivered with curative intent, is the current standard of care for patients of all ages, with newly diagnosed DLBCL. Approximately 30-40% of patients experience disease progression or relapse during the first 2 years and attempts to improve on R-CHOP regimen have not been successful.
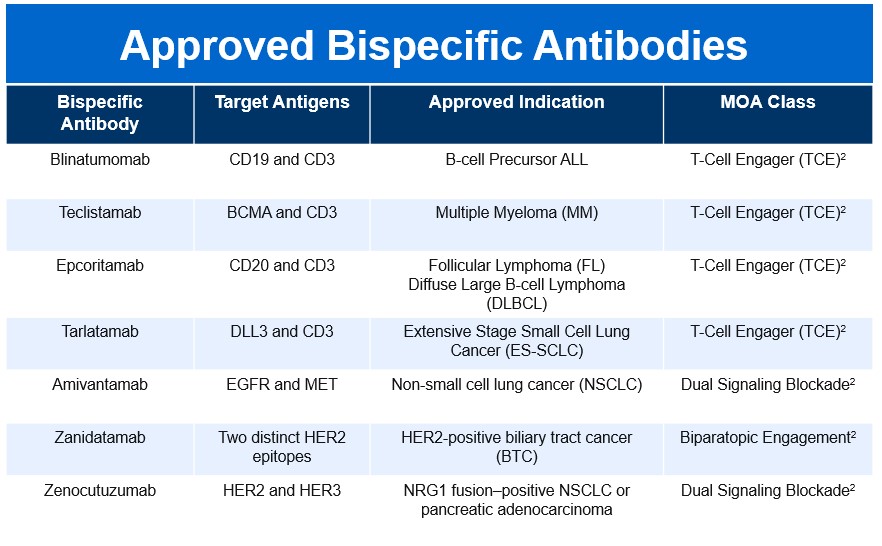
Relapsed or Refractory (R/R) Large B-Cell Lymphoma (LBCL), including Diffuse Large B-Cell Lymphoma (DLBCL), remains a challenging disease state with historically poor outcomes after multiple lines of therapy. CD20×CD3 Bispecific Antibodies (BsAbs), including Epcoritamab (EPKINLY®) and Glofitamab (COLUMVI®), represent a major therapeutic advance by redirecting endogenous T cells to malignant B cells through off-the-shelf immune engagement. Pivotal trials demonstrated encouraging response rates, leading to regulatory approvals in the United States. However, clinical trials often enroll selected patients with favorable performance status and limited comorbidity, underscoring the need for robust Real-World Evidence (RWE) to better understand effectiveness, durability, and outcomes in routine practice.
Study Design and Patient Population
The REALBiTE Consortium conducted a large multicenter retrospective analysis across 21 U.S. academic centers, evaluating patients with R/R DLBCL treated with commercially available Epcoritamab or Glofitamab between January 2023 and October 2024, with updated follow-up through May 2025.
Across multiple analyses, more than 300 patients were evaluated, reflecting a heavily pretreated, high-risk population:
- Over half were primary refractory to frontline therapy
- A substantial proportion had double-hit or triple-hit lymphoma
- Approximately 60% had prior CAR T-cell therapy, many of whom were CAR T-refractory
- Nearly 70% would have been ineligible for registrational trials due to comorbidities, disease burden, or performance status
This cohort therefore represents a realistic cross-section of patients encountered in contemporary lymphoma practice.
Efficacy Outcomes in the Real World
Despite high-risk features, Overall Response Rates (ORR) with BsAbs in routine practice were comparable to pivotal clinical trials:
- ORR approximately 51–54%
- Complete Response (CR) rates ranging from 23–33%
However, response durability was limited:
- Median Progression-Free Survival (PFS): ~2.5–2.6 months
- Median Overall Survival (OS): ~7.7–7.8 months
- Six-month PFS and OS rates were approximately 36% and 60%, respectively
These findings highlight a key real-world gap: while BsAbs induce meaningful initial responses, early disease progression remains common, particularly in biologically aggressive disease.
Predictors of Progression and Resistance
Several baseline clinical and biologic factors were associated with inferior outcomes:
- Double-hit or triple-hit lymphoma
- High International Prognostic Index (IPI)
- Poor performance status (ECOG ≥2)
- Primary refractory disease
- Refractoriness to the line of therapy immediately preceding BsAbs
Importantly, loss or absence of CD20 expression emerged as a critical resistance mechanism. Among patients with paired biopsies, nearly 90% lost CD20 expression following BsAb therapy, with rapid progression thereafter. Additionally, undetectable CD20 by immunohistochemistry prior to BsAb initiation was strongly associated with inferior PFS and OS, underscoring the clinical relevance of confirming target antigen expression before treatment.
Safety and Causes of Mortality
Progressive lymphoma was the leading cause of death, accounting for more than 80% of fatalities, followed by infections. Treatment-related deaths due to Cytokine Release Syndrome (CRS) or Immune effector Cell–Associated Neurotoxicity Syndrome (ICANS) were infrequent, reinforcing the manageable safety profile of BsAbs in experienced centers. Notably, infection-related mortality occurred early and late, highlighting the need for vigilance with immune suppression and supportive care.
Outcomes After Progression on Bispecific Antibodies
Disease progression following BsAb therapy was often rapid, with a median time to progression of approximately 1.5 months. Nearly half of progressing patients received no further anti-lymphoma therapy, reflecting clinical decline and limited salvage options.
Among patients who did receive subsequent treatment:
- Chemoimmunotherapy was most commonly used but achieved modest responses (~30%)
- Loncastuximab tesirine showed limited activity
- CAR T-cell therapy, when feasible, demonstrated the most favorable outcomes, with ORRs around 50% and high CR rates
- Allogeneic hematopoietic cell transplantation, used as consolidation in selected responders, resulted in encouraging short-term disease control, with many patients remaining progression-free at follow-up
Nevertheless, overall post-BsAb survival remained poor, with median OS after salvage therapy of less than 4 months.
Clinical Implications
These Real-World Data confirm that Epcoritamab and Glofitamab are active therapies in heavily pretreated R/R LBCL, even among patients excluded from clinical trials. However, the short duration of benefit in most patients emphasizes the aggressive biology of this population and the urgent need for improved sequencing strategies.
Key clinical takeaways include:
- Assessment of CD20 expression prior to BsAb initiation is critical
- Early identification of patients unlikely to benefit may help guide alternative strategies
- Clinical trial enrollment, novel combinations, or consolidation approaches (CAR T or allogeneic transplant) should be strongly considered for eligible responders
- Durable remissions, while uncommon, do occur, suggesting that a subset of patients can derive long-term benefit with appropriate selection
Conclusion
The REALBiTE Consortium provides the most comprehensive real-world assessment to date of CD20×CD3 bispecific antibodies in R/R LBCL. While Response Rates mirror those seen in pivotal trials, real-world PFS and OS are shorter, reflecting broader patient inclusion and aggressive disease biology. These findings reinforce the transformative potential of BsAbs while highlighting the need for better predictive biomarkers, rational combinations, and optimized sequencing to improve long-term outcomes for this challenging patient population.
Outcomes following disease progression after epcoritamab or glofitamab in the real-world outcomes of bispecific T-cell engagers (REALBiTE) multi-center, retrospective cohort study. Brooks T, Mian A, Nedved A, et al. Blood. 2025;146(suppl 1):402. doi:10.1182/blood-2025-402