
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2019, about 228,150 new cases of lung cancer will be diagnosed and 142,670 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. Approximately 15% of patients present with early stage (T1-2 N0) disease, and these numbers are likely to increase with the implementation of Lung Cancer screening programs. Patients with early stage disease unless medically unfit, undergo surgical resection with a curative intent. Those who are not surgical candidates are often treated with conventional Radiation Therapy, over a period of 4 to 6 weeks.
Stereotactic Body Radiation Therapy (SBRT) is a non-surgical procedure that allows delivery of significantly higher doses of precisely focused radiation to the tumor, compared to conventional Radiation Therapy, with less collateral damage to the surrounding normal tissue. The technologies used for SBRT include GAMMA KNIFE® which uses highly focused gamma rays, Proton Beam therapy which uses ionized Hydrogen or Protons, Linear Accelerator (LINAC) and CYBER KNIFE® which use Photons, to target the tumor tissue. Because SBRT is fractionated and delivered over 1-5 days, the short-and long-term side effects of radiation therapy are decreased and may allow higher total dosage to be given. Previously published single-arm trials have shown high local control with SBRT, with no significant difference in Overall Survival, compared with conventional Radiotherapy. This Phase III trial was conducted to prospectively assess the effect of SBRT on local control, Overall Survival, toxicity and Quality of Life.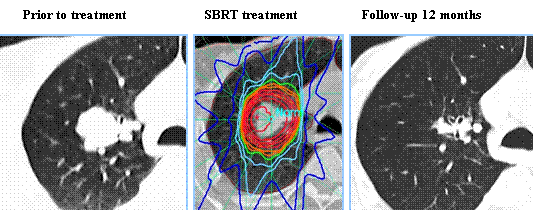
In this multicentre, randomized, Phase III trial, 101 eligible patients with biopsy proven Stage I (T1-T2aN0M0) NSCLC, diagnosed on the basis of FDG PET, who were medically inoperable or had refused surgery, were enrolled. Patients were randomly assigned in a 2:1 ratio to SBRT (54 Gy in three 18 Gy fractions, or 48 Gy in four 12 Gy fractions if the tumor was less than 2 cm from the chest wall)-(N=66) or standard Radiotherapy (66 Gy in 33 daily 2 Gy fractions or 50 Gy in 20 daily 2.5 Gy fractions (N=35), based on institutional preference. The tumor had to be non-central and peripherally located, at least 1 cm in the mediastinum and 2 cm from the bifurcation of the lobar bronchi. Patients were stratified by T stage and operability (medically operable but refused surgery versus inoperable). The Primary endpoint was time to local treatment failure and Secondary endpoints included Overall Survival, treatment related toxicity and Quality of Life. The median follow up for local treatment failure was 2.1 years for standard Radiotherapy group and 2.6 years for those patients assigned to SBRT.
Local treatment failure was noted in 14% of patients in the SBRT group whereas 31% of patients in the standard Radiotherapy group progressed locally. Freedom from local treatment failure was significantly improved the SBRT group compared with a standard radiotherapy group (HR=0.32, P=0.0077). Median time to local treatment failure was not reached in either group. Median Overall Survival was 5 years in the SBRT group and 3 years in the standard Radiotherapy group (HR=0.53; P=0.027). Overall Survival at 2 years was 77% for those receiving SBRT and 59% for those in the standard Radiotherapy group. Treatment related toxicities were low in both groups and there were no significant differences in Quality of Life between the treatment groups.
It was concluded that in patients with inoperable peripherally located Stage 1 NSCLC, compared with standard Radiotherapy, SBRT resulted in superior local control of the primary disease without an increase in major toxicity, and improvement in Overall Survival. The authors added that these findings suggest that SBRT should be the treatment of choice for this patient group. Stereotactic ablative radiotherapy versus standard radiotherapy in stage 1 non-small-cell lung cancer (TROG 09.02 CHISEL): a phase 3, open-label, randomised controlled trial. Ball D, Tao Mai G, Vinod S, et al. Lancet Oncol 2019;20:494-503
 The approval of INREBIC®was based on findings from the
The approval of INREBIC®was based on findings from the