SUMMARY: The FDA on July 31, 2017, granted accelerated approval to OPDIVO® (Nivolumab) for the treatment of patients 12 years and older with MisMatch Repair deficient (dMMR) and MicroSatellite Instability-High (MSI-H) metastatic ColoRectal Cancer, that has progressed following treatment with a Fluoropyrimidine, Oxaliplatin, and Irinotecan. ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. The lifetime risk of developing ColoRectal Cancer is about 1 in 20 (5%).
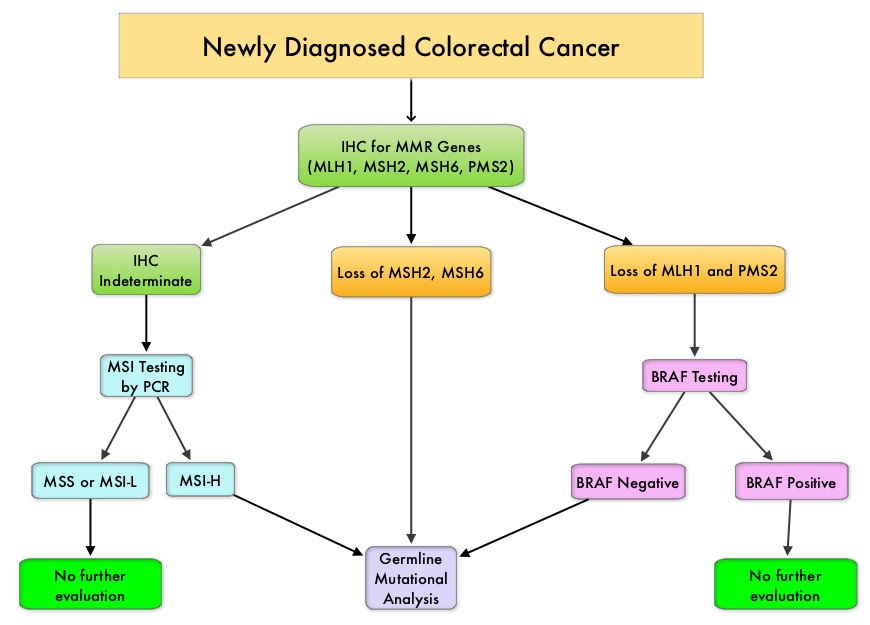
The DNA MisMatchRepair (MMR) system is responsible for molecular surveillance and works as an editing tool that identifies errors within the microsatellite regions of DNA and removes them. Defective MMR system leads to MSI (Micro Satellite Instability) and hypermutation, triggering an enhanced antitumor immune response. MSI (Micro Satellite Instability) is therefore a hallmark of defective/deficient DNA MisMatchRepair (MMR) system and occurs in 15% of all colorectal cancers. Defective MisMatchRepair can be a sporadic or heritable event. Approximately 65% of the MSI tumors are sporadic and when sporadic, the DNA MisMatchRepair gene is MLH1. Defective MisMatchRepair can also manifest as a germline mutation occurring in 1 of the 4 MisMatchRepair genes which include MLH1, MSH2, MSH6, PMS2. This produces Lynch Syndrome (Hereditary Nonpolyposis Colorectal Carcinoma – HNPCC), an Autosomal Dominant disorder and is the most common form of hereditary colon cancer, accounting for 35% of the MSI colorectal cancers. MSI tumors tend to have better outcomes and this has been attributed to the abundance of tumor infiltrating lymphocytes in these tumors from increase immunogenicity. These tumors therefore are susceptible to PD-1 blockade with immune checkpoint inhibitors.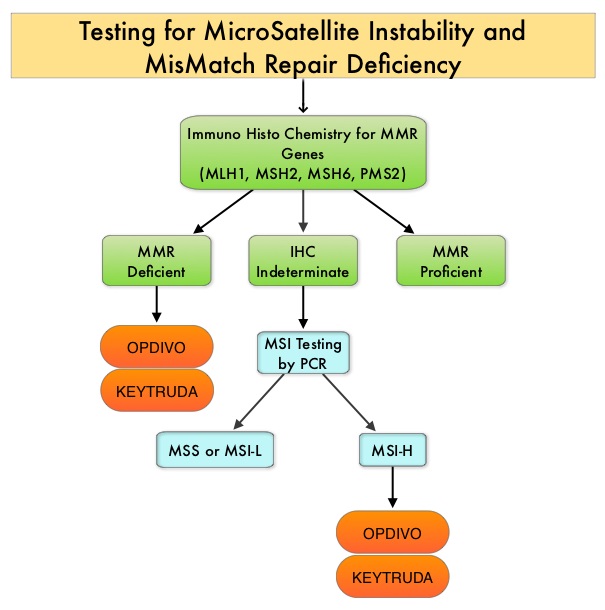
MSI (Micro Satellite Instability) testing is performed using a PCR based assay and MSI-High refers to instability at 2 or more of the 5 mononucleotide repeat markers and MSI-Low refers to instability at 1 of the 5 markers. Patients are considered Micro Satellite Stable (MSS) if no instability occurs. MSI-L and MSS are grouped together because MSI-L tumors are uncommon and behave similar to MSS tumors. Tumors considered MSI-H have deficiency of one or more of the DNA MisMatchRepair genes. MMR gene deficiency can be detected by ImmunoHistoChemistry (IHC). MLH1 gene is often lost in association with PMS2. NCCN Guidelines recommend MMR or MSI testing for all patients with a history of Colon or Rectal cancer.
This latest approval for OPDIVO® was based on results from the phase II CheckMate-142 trial, which is a multicenter, open label, single arm study, involving 53 patients with dMMR or MSI-H metastatic ColoRectal Cancer, who had disease progression during, after, or were intolerant to prior treatment with Fluoropyrimidine, Oxaliplatin, and Irinotecan-based chemotherapy. These 53 patients were a subset of the 74 patients who received at least one prior treatment regimen containing a Fluoropyrimidine with Oxaliplatin or Irinotecan for metastatic disease. All patients received OPDIVO® 3 mg/kg by intravenous infusion every 2 weeks until unacceptable toxicity or radiographic progression. The median age was 53 years. The Primary endpoint was Objective Response Rate (ORR) and exploratory endpoints included Safety, Progression Free Survival, Overall Survival and efficacy in biomarker-defined populations.
The Objective Response Rate as assessed by independent radiographic review committee, was 28% in the 53 patients who received prior Fluoropyrimidine, Oxaliplatin, and Irinotecan and responses lasted 6 months or more for the 67% of the responding patients. There was 1 complete response and 14 partial responses. The ORR was 32% among the 74 patients in the overall population. These responses and Clinical Benefit was seen regardless of PD-L1 expression, BRAF mutation status, KRAS mutation status, and clinical history of Lynch Syndrome. The most common adverse reactions related to OPDIVO® included fatigue, asthenia, rash, fever, nausea, diarrhea, musculoskeletal pain, cough and dyspnea.
The authors concluded that patients with metastatic ColoRectal Cancer who have dMMR or MSI-H tumors are less likely to respond to conventional chemotherapy and OPDIVO® demonstrated durable responses and disease control in this heavily pretreated patient group. Nivolumab in patients with DNA mismatch repair deficient/microsatellite instability high metastatic colorectal cancer: Update from CheckMate 142. Overman MJ, Lonardi S, Leone F, et al. J Clin Oncol 35, 2017 (suppl 4S; abstract 519).