
SUMMARY: The FDA on August 5, 2016, granted accelerated approval to KEYTRUDA® (Pembrolizumab) for the treatment of patients with recurrent or metastatic Head and Neck Squamous Cell Carcinoma (HNSCC), with disease progression on or after Platinum containing chemotherapy. The American Cancer Society estimates that 61,760 people will be diagnosed with Head and Neck cancer in 2016 and 13,190 patients will die of the disease. Patients with recurrent/metastatic Squamous Cell Carcinoma of the Head and Neck have a poor prognosis with a median Overall Survival (OS) of about 13 months with first line therapy and about 6 months or less with later lines of therapy. 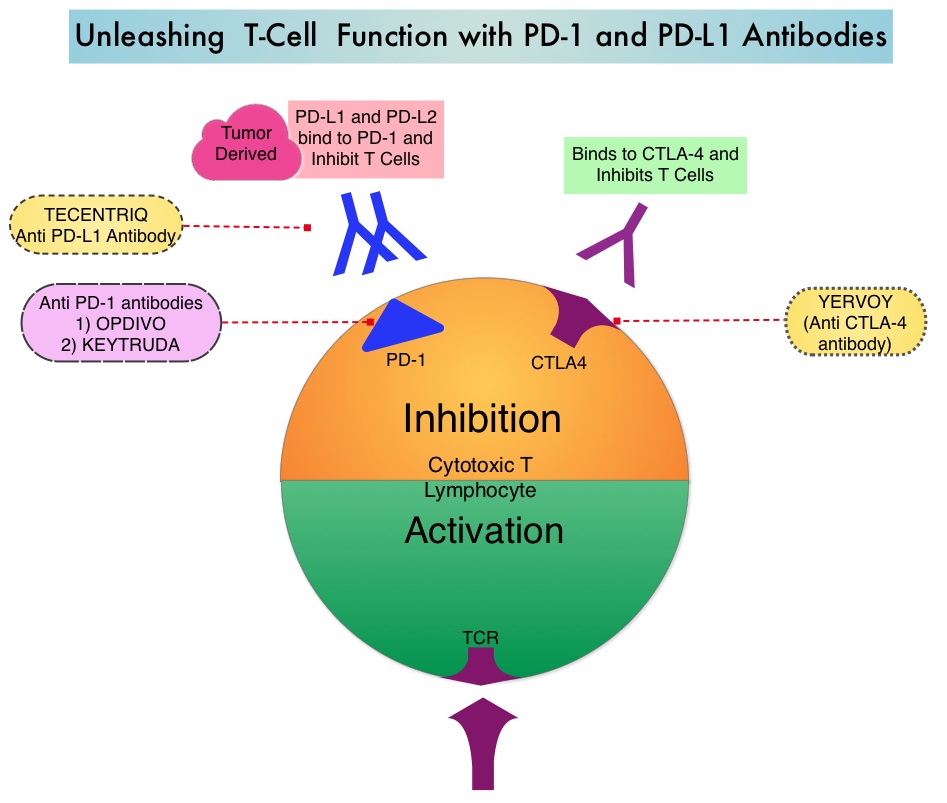 The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of the Immune checkpoints or gate keepers. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent related to their ability to escape immune surveillance by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response.
The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of the Immune checkpoints or gate keepers. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent related to their ability to escape immune surveillance by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response.
KEYTRUDA® is a fully humanized, Immunoglobulin G4, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. The accelerated approval of KEYTRUDA® was based on a multicenter, nonrandomized, open-label, multi-cohort phase Ib study (KEYNOTE-012), which included 192 patients with recurrent or metastatic HNSCC. Approximately 33% of the patients were HPV positive and patients have a median of two prior lines of therapy. Almost all enrolled patients (95%) had prior radiation therapy. Median patient age was 60 years. Treatment consisted of KEYTRUDA® 10 mg/kg IV every 2 weeks or 200 mg IV every 3 weeks and continued until disease progression or unacceptable toxicities. Patients without disease progression were treated for up to 24 months. The primary end point was Objective Response Rate (ORR) and Duration of Response. Secondary endpoints included response by HPV status, Progression Free Survival (PFS), and safety. Efficacy was evaluated in 174 of the enrolled patients. The ORR was 16% with a Complete Response Rate of 5%. The median response duration had not been reached at the time of analysis. Among the responding patients, 82% had responses of 6 months or longer. The ORR and Duration of Response were similar irrespective of dosage regimen or HPV status. In a pooled analyses after long term follow up, responses were ongoing in 76% of the patients with a median follow up duration in responders of 12.5 months. Median Overall Survival was 8.5 months and 6 month PFS rate was 24.9%. The most common adverse reactions ((20% or greater) were fatigue, decreased appetite, and dyspnea and these were similar to those occurring in patients with Melanoma or Non Small Cell Lung Cancer, with the exception of an increased incidence of facial edema and new or worsening hypothyroidism.
It was concluded that KEYTRUDA® has significant antitumor activity in recurrent/metastatic Head and Neck Squamous Cell Carcinoma and PD-L1 testing is not needed prior to use of KEYTRUDA® for this indication. As a condition of the accelerated approval, a multicenter, randomized trial is to be conducted for continued approval, establishing the superiority of KEYTRUDA® over standard therapy. Efficacy and safety of pembrolizumab in recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC): Pooled analyses after long-term follow-up in KEYNOTE-012. Mehra R, Seiwert TY, Mahipal A, et al. J Clin Oncol 34, 2016 (suppl; abstr 6012)
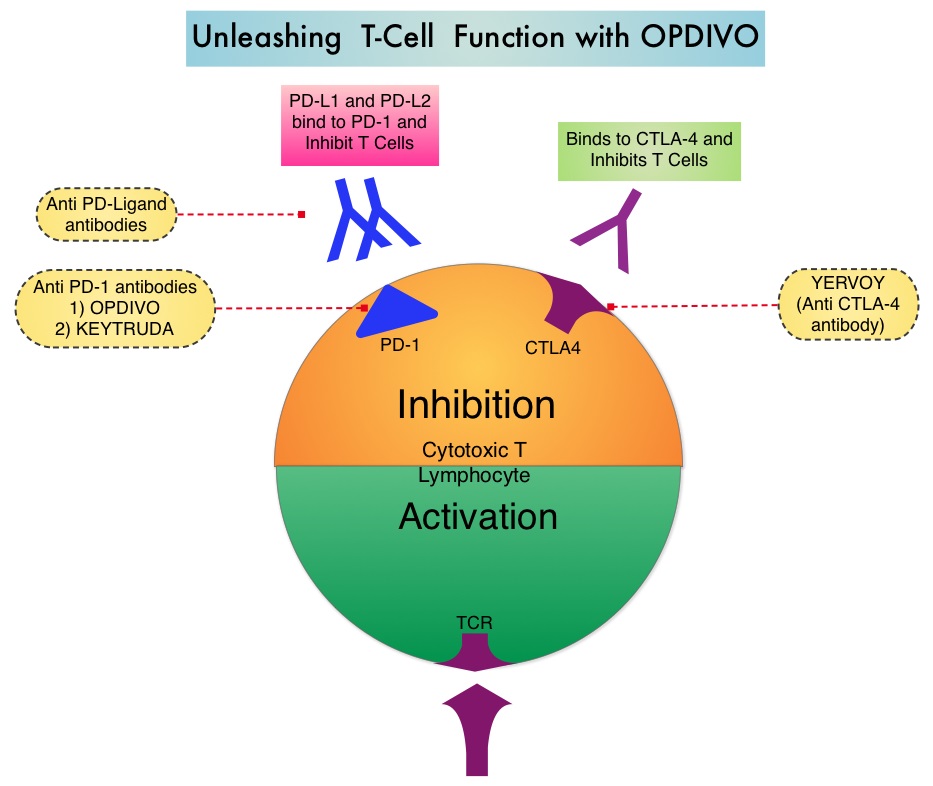
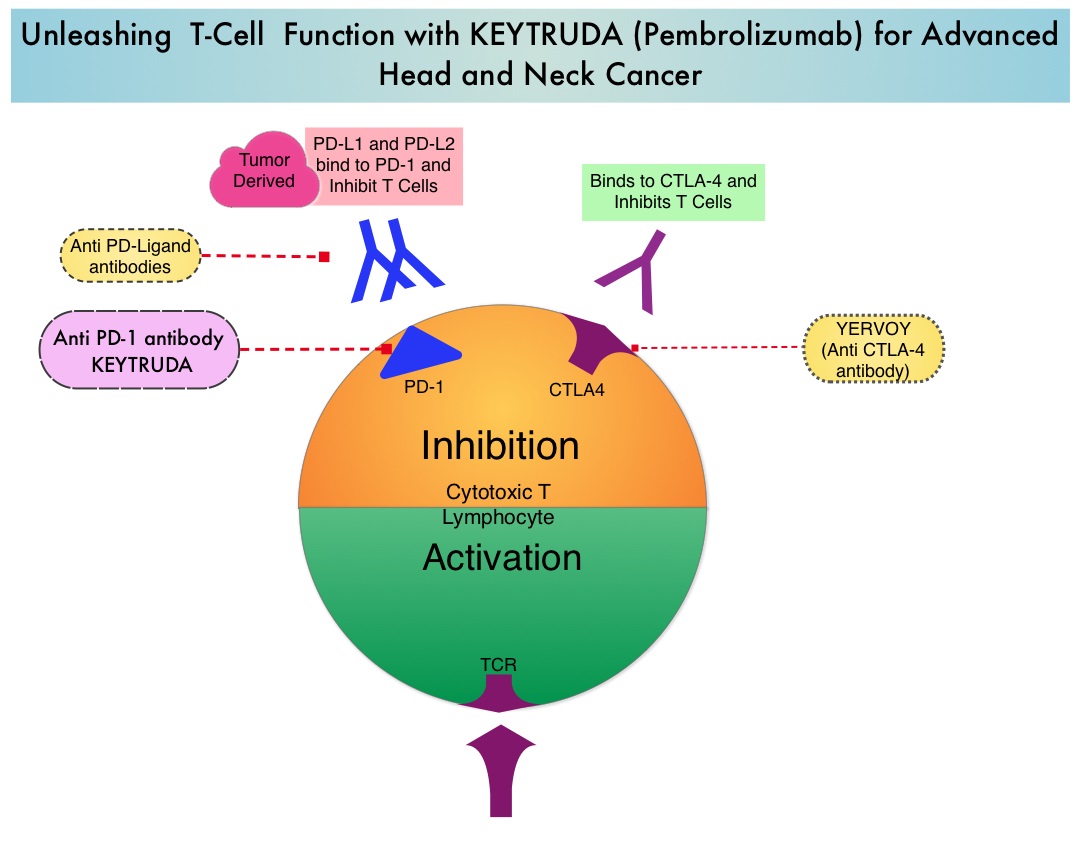 Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first Immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. The FDA granted accelerated approval to KEYTRUDA® in September 2014, for the treatment of patients with unresectable or metastatic melanoma and disease progression following YERVOY® and, if BRAF V600 mutation positive, a BRAF inhibitor. The activity of KEYTRUDA® as a single agent in advanced SCCHN patients, was previously published and was noted in PD-L1 positive tumors, regardless of the Human PapillomaVirus (HPV) status. The Overall Response Rate in this patient group was 20% and 29% of patients had stable disease. The authors in this study reported the efficacy of once every three week dose of KEYTRUDA®, in a larger expansion cohort of KEYNOTE 012 study. In this study, 132 patients with recurrent/metastatic SCCHN were enrolled, regardless of their PD-L1 expression or HPV status. These patients received a fixed dose of KEYTRUDA® 200 mg IV, every 3 weeks and patients were evaluated every 8 weeks with radiographic imaging. The mean age was 59 years and 57% of the patients had 2 or more lines of therapy for recurrent disease. Treatment was continued until disease progression. The primary end point was Overall Response Rate (ORR) and secondary endpoints included Progression Free Survival (PFS) and Overall Survival (OS). The Overall Response Rate was 25% and stable disease was noted in an additional 25% of the patients. This amounted to a disease control rate of 50%. Patients with HPV-positive disease had a response rate of 20.6% and patients with HPV-negative disease had a response rate of 27.2%, suggesting that KEYTRUDA® was active in both subgroups of patients. Serious toxicities were reported in fewer than 10% of patients and the most common adverse event was fatigue (15.2%). The authors concluded that KEYTRUDA® given every 3 weeks was well tolerated and demonstrated a meaningful response rate in a heavily pretreated population of patients, with recurrent/metastatic SCCHN. Evaluation of PD-L1 status for this patient group is ongoing. Antitumor activity and safety of pembrolizumab in patients (pts) with advanced squamous cell carcinoma of the head and neck (SCCHN): Preliminary results from KEYNOTE-012 expansion cohort. Seiwert TY, Haddad RI, Gupta S, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA6008)</s
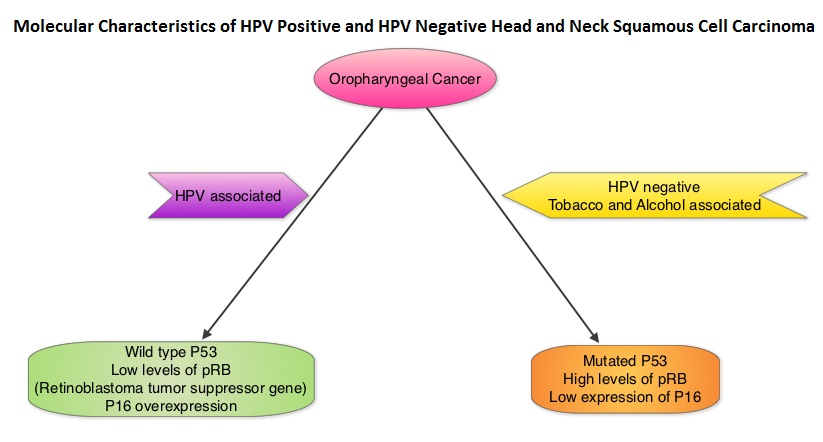
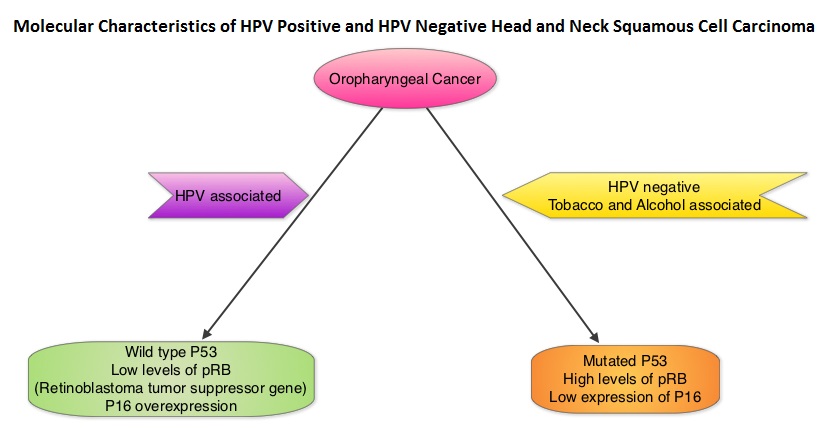
Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first Immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. The FDA granted accelerated approval to KEYTRUDA® in September 2014, for the treatment of patients with unresectable or metastatic melanoma and disease progression following YERVOY® and, if BRAF V600 mutation positive, a BRAF inhibitor. The activity of KEYTRUDA® as a single agent in advanced SCCHN patients, was previously published and was noted in PD-L1 positive tumors, regardless of the Human PapillomaVirus (HPV) status. The Overall Response Rate in this patient group was 20% and 29% of patients had stable disease. The authors in this study reported the efficacy of once every three week dose of KEYTRUDA®, in a larger expansion cohort of KEYNOTE 012 study. In this study, 132 patients with recurrent/metastatic SCCHN were enrolled, regardless of their PD-L1 expression or HPV status. These patients received a fixed dose of KEYTRUDA® 200 mg IV, every 3 weeks and patients were evaluated every 8 weeks with radiographic imaging. The mean age was 59 years and 57% of the patients had 2 or more lines of therapy for recurrent disease. Treatment was continued until disease progression. The primary end point was Overall Response Rate (ORR) and secondary endpoints included Progression Free Survival (PFS) and Overall Survival (OS). The Overall Response Rate was 25% and stable disease was noted in an additional 25% of the patients. This amounted to a disease control rate of 50%. Patients with HPV-positive disease had a response rate of 20.6% and patients with HPV-negative disease had a response rate of 27.2%, suggesting that KEYTRUDA® was active in both subgroups of patients. Serious toxicities were reported in fewer than 10% of patients and the most common adverse event was fatigue (15.2%). The authors concluded that KEYTRUDA® given every 3 weeks was well tolerated and demonstrated a meaningful response rate in a heavily pretreated population of patients, with recurrent/metastatic SCCHN. Evaluation of PD-L1 status for this patient group is ongoing. Antitumor activity and safety of pembrolizumab in patients (pts) with advanced squamous cell carcinoma of the head and neck (SCCHN): Preliminary results from KEYNOTE-012 expansion cohort. Seiwert TY, Haddad RI, Gupta S, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA6008)</s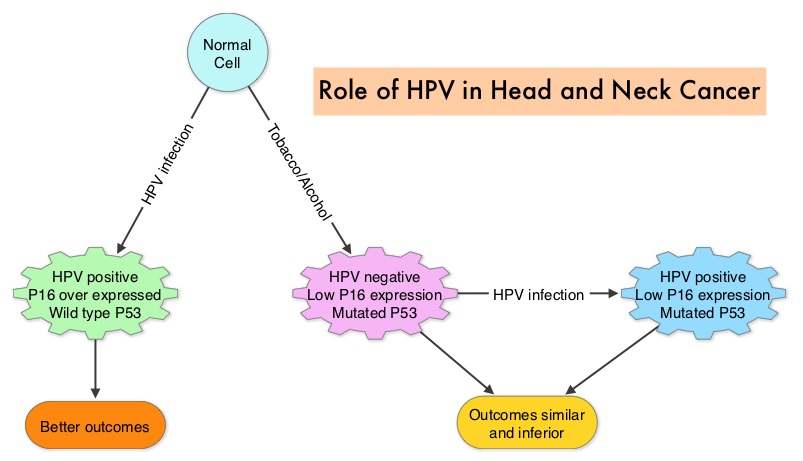 The malignant behavior of these tumors is dependent on the expression of viral E6 and E7 oncoproteins that inactivate the tumor suppressor proteins p53 and the retinoblastoma protein (pRB), respectively. HPV positive OroPharyngeal Squamous Cell Carcinoma (OPSCC) is more common among never smokers or light smokers and patients tend to be younger with better performance status. The pathobiology of HPV positive OroPharyngeal Squamous Cell Carcinoma (OPSCC) is different from the HPV negative OroPharyngeal Squamous Cell Carcinoma in that p53 is degraded/inactivated by viral E6 oncoprotein instead of by genetic mutation, pRB pathway is inactivated by viral E7 oncoprotein instead of Cyclin D1 amplification and p16 is overexpressed or upregulated instead of inactivation resulting from reduced negative feedback from pRB. Testing for HPV is based on several methodologies which include detection of HPV DNA by in situ hybridization (ISH) or Polymerase Chain Reaction (PCR), detection of HPV E6/E7 RNA expression by quantitative Reverse Transcriptase–PCR (qRT-PCR) and p16 protein overexpression, a surrogate marker of oncogenic HPV infection, by ImmunoHistoChemistry (IHC) staining. Both p16 overexpression testing by IHC and HPV by ISH can be easily performed on Formalin-Fixed Paraffin Embedded (FFPE) specimen whereas detection of HPV E6/E7 RNA expression, which is indicative of active viral oncogene transcription in tumor cells and is considered to be a gold standard, requires a larger tumor specimen compared with other methodologies.
The malignant behavior of these tumors is dependent on the expression of viral E6 and E7 oncoproteins that inactivate the tumor suppressor proteins p53 and the retinoblastoma protein (pRB), respectively. HPV positive OroPharyngeal Squamous Cell Carcinoma (OPSCC) is more common among never smokers or light smokers and patients tend to be younger with better performance status. The pathobiology of HPV positive OroPharyngeal Squamous Cell Carcinoma (OPSCC) is different from the HPV negative OroPharyngeal Squamous Cell Carcinoma in that p53 is degraded/inactivated by viral E6 oncoprotein instead of by genetic mutation, pRB pathway is inactivated by viral E7 oncoprotein instead of Cyclin D1 amplification and p16 is overexpressed or upregulated instead of inactivation resulting from reduced negative feedback from pRB. Testing for HPV is based on several methodologies which include detection of HPV DNA by in situ hybridization (ISH) or Polymerase Chain Reaction (PCR), detection of HPV E6/E7 RNA expression by quantitative Reverse Transcriptase–PCR (qRT-PCR) and p16 protein overexpression, a surrogate marker of oncogenic HPV infection, by ImmunoHistoChemistry (IHC) staining. Both p16 overexpression testing by IHC and HPV by ISH can be easily performed on Formalin-Fixed Paraffin Embedded (FFPE) specimen whereas detection of HPV E6/E7 RNA expression, which is indicative of active viral oncogene transcription in tumor cells and is considered to be a gold standard, requires a larger tumor specimen compared with other methodologies.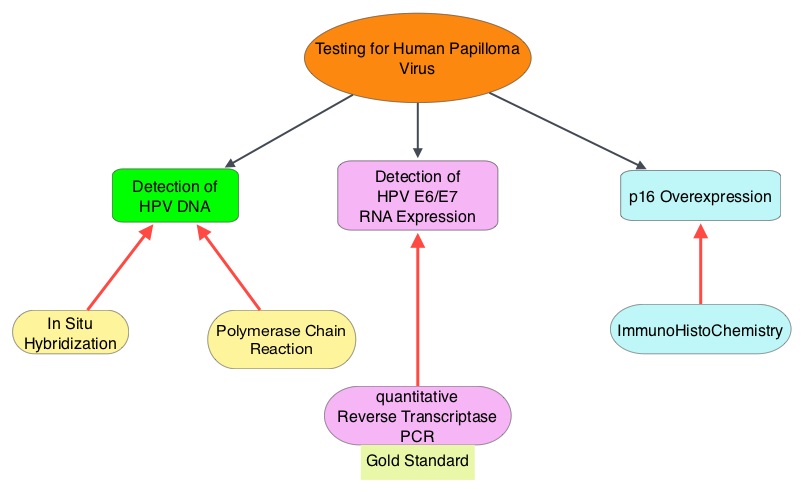 The concordance rate between HPV by ISH and p16 by IHC is approximately 90% in OPSCC, whereas the prevalence and significance p16 by IHC has remained unclear for HPV infection in non-OPSCC (oral cavity, hypopharynx and larynx). It is well established however that patients with HPV-positive/p16-positive OPSCC have better outcomes compared with those with HPV-negative/p16-negative OPSCC. However, the prognostic significance of p16 overexpression in non-OPSCC patients with or without evidence of HPV infection has not been clear. The authors in this study evaluated p16 protein overexpression by IHC and HPV status by HPV ISH as potential prognostic biomarkers in non-OPSCC tumors of patients enrolled in three prospective Radiation Therapy Oncology Group (RTOG) clinical trials. Of the 1921 patient enrolled in these three trials, 683 patients with non-OPSCC tumors were eligible and 52% (N=356) of these patients were tested for p16 overexpression and overall, 19.3% were p16 positive. When OPSCC and non-OPSCC patients were compared, OPSCC patients whose tumors were p16 positive had better Progression Free Survival and Overall Survival than non-OPSCC patients with p16 positive tumors. However, patients with p16 negative OPSCC and non-OPSCC have similar inferior outcomes. The authors concluded that patients with p16 negative non-OPSCC have worse outcomes than patients with p16 positive non-OPSCC, similar to that seen in patients with OPSCC and therefore HPV infection may influence outcomes in a subset of patients with non-OPSCC as well. Better methodologies for HPV detection and correlation with p16 expression will help identify “true” HPV infection related non-OPSCC and thereby enable tailored and less intense treatment, for this favorable group of patients. Chung CH, Zhang Q, Kong CS, et al. J Clin Oncol 2014; 32:3930-3938
The concordance rate between HPV by ISH and p16 by IHC is approximately 90% in OPSCC, whereas the prevalence and significance p16 by IHC has remained unclear for HPV infection in non-OPSCC (oral cavity, hypopharynx and larynx). It is well established however that patients with HPV-positive/p16-positive OPSCC have better outcomes compared with those with HPV-negative/p16-negative OPSCC. However, the prognostic significance of p16 overexpression in non-OPSCC patients with or without evidence of HPV infection has not been clear. The authors in this study evaluated p16 protein overexpression by IHC and HPV status by HPV ISH as potential prognostic biomarkers in non-OPSCC tumors of patients enrolled in three prospective Radiation Therapy Oncology Group (RTOG) clinical trials. Of the 1921 patient enrolled in these three trials, 683 patients with non-OPSCC tumors were eligible and 52% (N=356) of these patients were tested for p16 overexpression and overall, 19.3% were p16 positive. When OPSCC and non-OPSCC patients were compared, OPSCC patients whose tumors were p16 positive had better Progression Free Survival and Overall Survival than non-OPSCC patients with p16 positive tumors. However, patients with p16 negative OPSCC and non-OPSCC have similar inferior outcomes. The authors concluded that patients with p16 negative non-OPSCC have worse outcomes than patients with p16 positive non-OPSCC, similar to that seen in patients with OPSCC and therefore HPV infection may influence outcomes in a subset of patients with non-OPSCC as well. Better methodologies for HPV detection and correlation with p16 expression will help identify “true” HPV infection related non-OPSCC and thereby enable tailored and less intense treatment, for this favorable group of patients. Chung CH, Zhang Q, Kong CS, et al. J Clin Oncol 2014; 32:3930-3938
 To address this further, the authors examined the influence of tumor HPV status (tumor p16) on patterns of failure and survival after disease progression, by performing a retrospective analysis of the association between tumor p16 status and overall survival (OS) after disease progression, amongst patients enrolled in the Radiation Therapy Oncology Group (RTOG) trials 0129 and RTOG 0522. Eligible patients from these two trials had stage III-IV OroPharygeal Squamous Cell Carcinoma. Their tumor p16 status was known and these patients had local, regional, and/or distant progression after receiving platinum-based chemoradiotherapy. Of the 181 patients included in this analysis, 105 patients had p16 positive OPSCC and 76 patients had p16 negative OPSCC. Tumor p16 expression was evaluated using immunohistochemistry methodology. Even though the patterns of failure and median time to progression were similar for patients with p16-positive and p16-negative tumors, after a median follow up period of 4 years after disease progression, patients with p16-positive OPSCC had significantly improved Overall Survival (OS) rates compared with p16-negative patients (2-year OS, 54.6% vs 27.6%; median, 2.6 vs 0.8 years; P <0.001). This meant that patients with HPV positive recurrent OPSCC had nearly twice the overall survival rate compared to HPV negative patients. Further, salvage surgery after disease progression in HPV positive patients reduced the risk of death. Factors associated with improved survival in multivariate analysis included, HPV positive status, salvage surgery, locoregional progression vs distant progression, lower T stage at enrollment and less than 20 pack year smoking history.
To address this further, the authors examined the influence of tumor HPV status (tumor p16) on patterns of failure and survival after disease progression, by performing a retrospective analysis of the association between tumor p16 status and overall survival (OS) after disease progression, amongst patients enrolled in the Radiation Therapy Oncology Group (RTOG) trials 0129 and RTOG 0522. Eligible patients from these two trials had stage III-IV OroPharygeal Squamous Cell Carcinoma. Their tumor p16 status was known and these patients had local, regional, and/or distant progression after receiving platinum-based chemoradiotherapy. Of the 181 patients included in this analysis, 105 patients had p16 positive OPSCC and 76 patients had p16 negative OPSCC. Tumor p16 expression was evaluated using immunohistochemistry methodology. Even though the patterns of failure and median time to progression were similar for patients with p16-positive and p16-negative tumors, after a median follow up period of 4 years after disease progression, patients with p16-positive OPSCC had significantly improved Overall Survival (OS) rates compared with p16-negative patients (2-year OS, 54.6% vs 27.6%; median, 2.6 vs 0.8 years; P <0.001). This meant that patients with HPV positive recurrent OPSCC had nearly twice the overall survival rate compared to HPV negative patients. Further, salvage surgery after disease progression in HPV positive patients reduced the risk of death. Factors associated with improved survival in multivariate analysis included, HPV positive status, salvage surgery, locoregional progression vs distant progression, lower T stage at enrollment and less than 20 pack year smoking history.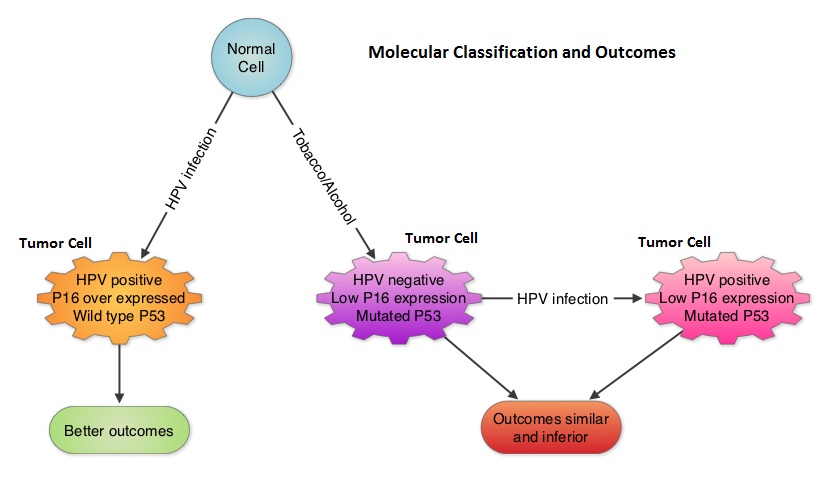 The authors concluded that patients with HPV positive OroPharyngeal Squamous Cell Carcinoma (OPSCC) have tumors with different molecular behavior, compared to HPV negative and tobacco related OPSCC and tumor p16 status is independently associated with Overall Survival among OPSCC patients with disease progression. This important information should be a stratification factor for clinical trials and the benefits of salvage surgery dictates close surveillance as these patients are followed up. Fakhry C, Zhang Q, Nguyen-Tan PF, et al. Published Ahead of Print on June 23, 2014 as 10.1200/JCO.2014.55.1937
The authors concluded that patients with HPV positive OroPharyngeal Squamous Cell Carcinoma (OPSCC) have tumors with different molecular behavior, compared to HPV negative and tobacco related OPSCC and tumor p16 status is independently associated with Overall Survival among OPSCC patients with disease progression. This important information should be a stratification factor for clinical trials and the benefits of salvage surgery dictates close surveillance as these patients are followed up. Fakhry C, Zhang Q, Nguyen-Tan PF, et al. Published Ahead of Print on June 23, 2014 as 10.1200/JCO.2014.55.1937