
The FDA on October 16, 2018 approved KEYTRUDA® in combination with Carboplatin and either Paclitaxel or nab-Paclitaxel, as first-line treatment of metastatic squamous Non-Small Cell Lung Cancer (NSCLC). KEYTRUDA® is a product of Merck & Co. Inc.
Tag: Lung Cancer: Non-Small Cell
IMFINZI® after Chemoradiotherapy Significantly Improves Overall Survival in Stage III NSCLC
IMFINZI® (Durvalumab) is a selective, high-affinity, human IgG1 monoclonal antibody, that blocks the binding of Programmed Death Ligand 1 (PD-L1) to Programmed Death 1 (PD-1) receptor and CD80, thereby unleashing the T cells to recognize and kill tumor cells. Patients with stage III Non Small Cell Lung Cancer (NSCLC) are often treated with platinum-based doublet chemotherapy with concurrent radiation and have a median Progression Free Survival (PFS) of approximately 8 months and 5 year survival of only 15%. PACIFIC trial is a randomized, double-blind, international, phase III study in which IMFINZI® as consolidation therapy was compared with placebo, in patients with stage III, locally advanced, unresectable NSCLC, that had not progressed following platinum-based chemoradiotherapy.
At a median follow up of 25.2 months, the 24-month Overall Survival rate was 66.3% in the IMFINZI® group and 55.6% in the placebo group, suggesting a significantly prolonged Overall Survival with IMFINZI® when compared with placebo and a 32% reduction in the risk of death (HR for death=0.68; P=0.0025). The Overall Survival benefit with IMFINZI®, was observed across all the prespecified subgroups.
PACIFIC trial is the first study to demonstrate a survival advantage for unresectable Stage III NSCLC, supporting this regimen as the standard of care.
IMFINZI® after Chemoradiotherapy Significantly Improves Overall Survival in Stage III NSCLC
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2018 about 234,030 new cases of lung cancer will be diagnosed and over 154,050 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), approximately 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas, and 10% are Large cell carcinomas.
Approximately one third of all patients with NSCLC have stage III, locally advanced disease at the time of initial presentation. Worldwide, about 500,000 patients are diagnosed with unresectable, stage III NSCLC, each year. These patients include those with locally advanced primary tumors with tumor invading the vital mediastinal organs, as well as those with involvement of locoregional mediastinal lymph nodes. These patients are often treated with platinum-based doublet chemotherapy with concurrent radiation and have a median Progression Free Survival (PFS) of approximately 8 months and 5 year survival of only 15%. There is hence a significant unmet need for this patient group, with no major treatment advances thus far.
Preclinical evidence had suggested that chemotherapy and radiotherapy may upregulate PD-L1 expression in tumor cells. IMFINZI® (Durvalumab) is a selective, high-affinity, human IgG1 monoclonal antibody, that blocks the binding of Programmed Death Ligand 1 (PD-L1) to Programmed Death 1 (PD-1) receptor and CD80, thereby unleashing the T cells to recognize and kill tumor cells. IMFINZI® showed encouraging antitumor activity in an early phase clinical study involving multiple advanced solid tumors, including stage IIIB or IV NSCLC.
PACIFIC trial is a randomized, double-blind, international, phase III study in which IMFINZI® as consolidation therapy was compared with placebo, in patients with stage III, locally advanced, unresectable NSCLC, that had not progressed following platinum-based chemoradiotherapy. Eligible patients received two or more cycles of platinum-based doublet chemotherapy concurrently with definitive radiation therapy (54-66 Gy). Following completion of concurrent chemoradiation treatment, 713 patients were randomized, of whom 709 patients in a 2:1 ratio received consolidation treatment, within 6 weeks after completion of chemoradiation, with IMFINZI® 10 mg/kg every 2 weeks (N=473) or placebo (N=236), for up to 12 months. The median age was 64 years, and the majority of patients were men (70%) and 46% had a squamous histology. The co-Primary end points were Progression Free Survival (PFS) and Overall Survival (OS). Secondary end points included 12-month and 18-month PFS rates, Objective Response Rate (ORR), Duration of Response, time to death or distant metastasis, and safety.
The authors had previously reported the results of the first preplanned interim analysis, after a median follow up of 14.5 months. The median PFS from randomization to consolidation treatment was 16.8 months with IMFINZI® versus 5.6 months with placebo (HR=0.52; P<0.001). This meant a 11.2-month improvement in PFS with IMFINZI® versus placebo, and a 48% decrease in the probability of disease progression with IMFINZI®. This improvement was consistent across all patient subgroups that were analyzed.
The authors in this publication report the results for the second Primary end point of Overall Survival. At a median follow up of 25.2 months, the 24-month Overall Survival rate was 66.3% in the IMFINZI® group and 55.6% in the placebo group, suggesting a significantly prolonged Overall Survival with IMFINZI® when compared with placebo and a 32% reduction in the risk of death (HR for death=0.68; P=0.0025). The Overall Survival benefit with IMFINZI®, was observed across all the prespecified subgroups. In this updated analysis, the PFS was similar to those previously reported, with a median duration of 17.2 months in the IMFINZI® group and 5.6 months in the placebo group (HR=0.51). The median time to death or distant metastasis was 28.3 months in the IMFINZI® group and 16.2 months in the placebo group (HR=0.53). Approximately 30% of the patients in the IMFINZI® group and 26% of those in the placebo group had grade 3 or 4 adverse events of any cause, and 15% and 10% of the patients respectively, discontinued the trial regimen because of adverse events.
The authors concluded that in this updated analysis of the PACIFIC trial, the Primary end point of Overall Survival was significantly longer with IMFINZI® than with placebo, among patients with unresectable stage III NSCLC, in all the prespecified subgroups. The updated results for Secondary end points, including the time to death or distant metastasis, the incidence of new lesions, and the Objective Response Rate, were similar to those that were previously reported. The authors commented that PACIFIC trial is the first study to demonstrate a survival advantage for unresectable Stage III NSCLC, supporting this regimen as the standard of care. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. Antonia SJ, Villegas A, Daniel D, et al. [published online ahead of print September 25, 2018]. N Eng J Med. doi: 10.1056/NEJMoa1809697.
First Line KEYTRUDA® plus Chemotherapy Improves Overall Survival in Advanced Squamous NSCLC
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2018 about 234,030 new cases of lung cancer will be diagnosed and over 154,050 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), approximately 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas, and 10% are Large cell carcinomas. Non Small Cell Lung Cancer patients with Squamous Cell histology have been a traditionally hard- to-treat, patient group, and less than 15% of patients with advanced Squamous NSCLC survive a year after diagnosis and less than 5% of patients survive for five years or longer.
KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2. It thereby reverses the PD-1 pathway-mediated inhibition of the immune response and unleashes the tumor-specific effector T cells. The FDA approved KEYTRUDA® for the first-line treatment of advanced NSCLC with high PD-L1 expression (Tumor Proportion Score of 50% or more), as well as in combination with Pemetrexed and Carboplatin, as first-line treatment of patients with metastatic nonsquamous NSCLC and for previously treated advanced NSCLC with a PD-L1 Tumor Proportion Score of 1% or more. Currently, KEYTRUDA® currently is the only FDA approved immunotherapy for initial treatment of NSCLC as monotherapy (KEYNOTE-024) or in combination with chemotherapy (KEYNOTE-189).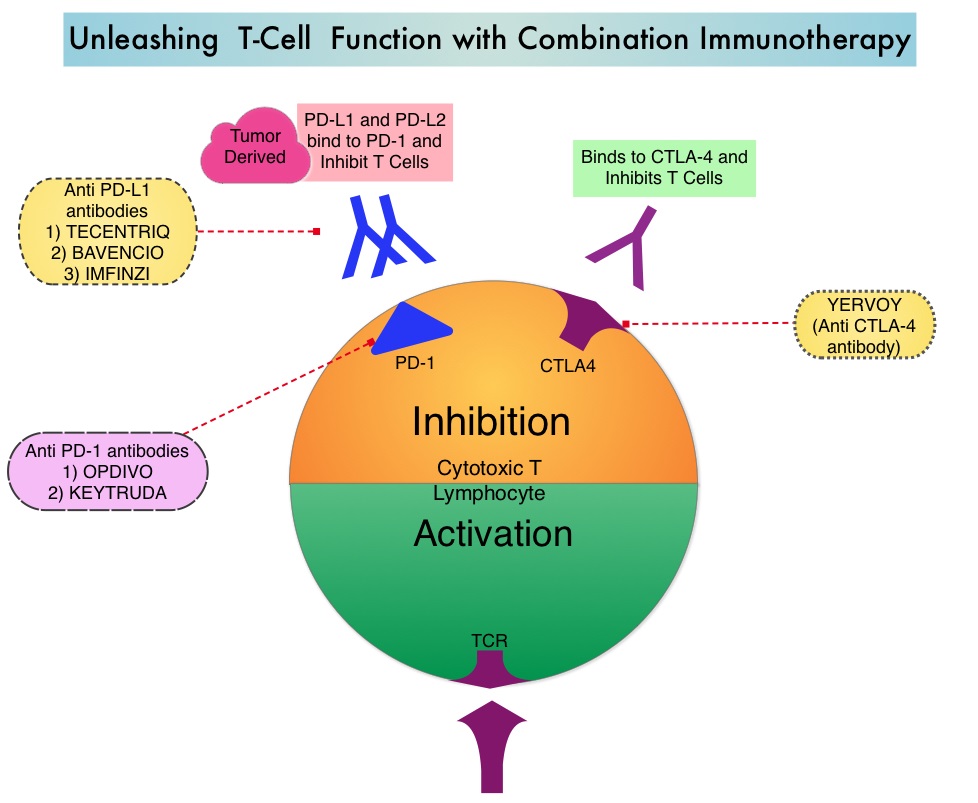
KEYNOTE-407 is a global, double-blind, placebo-controlled, phase 3 trial which compared KEYTRUDA® plus chemotherapy with placebo plus chemotherapy in patients with squamous NSCLC of any level of PD-L1 expression. In this study, 559 patients with untreated metastatic, squamous NSCLC were randomly assigned, in a 1:1 ratio to receive KEYTRUDA® 200 mg IV along with Carboplatin AUC 6 and either TAXOL® (Paclitaxel) 200 mg/m2 IV or ABRAXANE® (nab-paclitaxel) 100 mg/m2 IV days 1, 8 and 15. every 3 weeks for 4 cycles (N=278) or placebo with the same chemotherapy regimen for 4 cycles (N=281). Patients in the experimental arm following the first 4 cycles continued KEYTRUDA® every 3 weeks, for an additional 31 cycles, whereas the control group received placebo. Patients in the placebo-combination group were eligible to cross over to receive KEYTRUDA® monotherapy and 42.8% of patients assigned to the placebo plus chemotherapy group who discontinued chemotherapy went on to receive subsequent anti PD-1 or anti PD-L1 therapy and 75 patients received KEYTRUDA® monotherapy as part of in-study crossover. Patients were stratified according to the PD-L1 Tumor Proportion Score (1% or less versus more than 1%), choice of Taxane (Paclitaxel versus nab-Paclitaxel), and geographic region of enrollment. Tumor Proportion Score is the percentage of tumor cells with membranous PD-L1 staining, with less than 1% indicating PD-L1 negative score. Both treatment groups were well balanced. The co-Primary end points were Overall Survival and Progression Free Survival and the Secondary end points included Response Rate, Duration of Response and Safety. The effects of PD-L1 expression on Overall Survival (OS), Progression Free Survival (PFS), and Objective Response Rate (ORR) were prespecified exploratory end points.
At the second interim analysis, after a median follow-up of 7.8 months, the median Overall Survival was 15.9 months in the KEYTRUDA® combination group and 11.3 months in the placebo combination group (HR=0.64; P<0.001). This meant that there was a 36% reduction in the risk of death with the addition of KEYTRUDA® to chemotherapy. This OS benefit was consistently seen regardless of the level of PD-L1 expression. The median PFS was 6.4 months in the KEYTRUDA® combination group and 4.8 months in the placebo combination group (HR=0.56; P<0.001) and this suggested that the risk of disease progression or death was 44% lower with the addition of KEYTRUDA® to chemotherapy. The PFS benefit with the addition of KEYTRUDA® to chemotherapy was observed in all prespecified subgroups with incremental improvements noted with increasing PD-L1 Tumor Proportion Score. The Objective Response Rate was also significantly higher in the KEYTRUDA® chemotherapy group compared to the placebo chemotherapy group (59.4% versus 38%; P=0.0004), with a median time to response of 1.4 months and median Duration of Response of 7.7 months versus 4.8 months, respectively. Grade 3 or higher adverse events were similar in both treatment groups. Treatment discontinuation due to adverse events was more frequent in the KEYTRUDA® combination group (13.3% versus 6.4%).
It was concluded that inpatients with previously untreated metastatic, squamous NSCLC, the addition of KEYTRUDA® to chemotherapy resulted in significantly longer Overall Survival and Progression Free Survival than chemotherapy alone, and should become a new standard of care for squamous NSCLC. Pembrolizumab plus Chemotherapy for Squamous Non–Small-Cell Lung Cancer. Paz-Ares L, Luft A, Vicente D, et al. for the KEYNOTE-407 Investigators. September 25, 2018. DOI: 10.1056/NEJMoa1810865
VIZIMPRO® (Dacomitinib)
The FDA on September 27, 2018 approved VIZIMPRO® for the first-line treatment of patients with metastatic Non-Small Cell Lung Cancer (NSCLC) with Epidermal Growth Factor Receptor (EGFR) exon 19 deletion or exon 21 L858R substitution mutations, as detected by an FDA-approved test. VIZIMPRO® is aproduct of Pfizer Pharmaceutical Company.
Hyperprogressive Disease after Immunotherapy in Advanced Non-Small Cell Lung Cancer
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2018 about 234,030 new cases of lung cancer will be diagnosed and over 154,050 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Immunotherapy with PD-1 (Programmed cell Death 1) and PD-L1 (Programmed cell Death Ligand 1) inhibitors have demonstrated a clear survival benefit both as a single agent or in combination, compared with standard chemotherapy, in both treatment-naive and previously treated patients for advanced Non Small Cell Lung Cancer (NSCLC). Immuno-Oncology therapies unleash the T cells by blocking the Immune checkpoint proteins, thereby resulting in T cell proliferation, activation and a therapeutic response.
Recent reports of an acceleration of tumor growth during immunotherapy, defined as HyperProgressive Disease (HPD), has been observed in 9% of advanced malignancies and in 29% of patients with Head and Neck cancer treated with PD-1/PD-L1 inhibitors. It has been postulated that high level of interferon gamma (IFN-gamma) usually released by PD-1 blockade may have detrimental effects on immunity. Alternatively PD-1/PD-L1 blockade may upregulate Interleukin 6, Interleukin 17, and neutrophil axis, generating a potent aberrant inflammation, responsible for immune escape and accelerated growth.
HyperProgressive Disease should be differentiated from Pseudoprogression. The later is defined as progressive disease, followed by Complete Response and/or Partial Response or Stable Disease longer than 6 months. The Tumor Growth Rate (TGR) estimates the increase in tumor volume over time based on two Computed Tomography (CT) scan measurements. TGR can be used to quantitatively assess tumor dynamics and kinetics during treatment and can be specifically applied to identify the subset of patients experiencing HPD.
This study was conducted to investigate whether HPD is observed in patients with advanced NSCLC treated with PD-1/PD-L1 inhibitors compared with single-agent chemotherapy and whether there is an association between treatment and HPD. This multicenter, retrospective study included 406 consecutive eligible patients with confirmed Stage III or IV NSCLC treated with PD-1/PD-L1 inhibitors such as OPDIVO® (Nivolumab), KEYTRUDA® (Pembrolizumab), TECENTRIQ® (Atezolizumab), or IMFINZI® (Durvalumab) as monotherapy in second or later line treatment, at eight French institutions between November 2012 and April 2017. The control cohort included equivalent data collected on 59 eligible patients with advanced NSCLC, who had failed a Platinum-based regimen and received single-agent chemotherapy (Taxanes, Pemetrexed, Vinorelbine , or Gemcitabine) in 4 French institutions from August 2011, to June 2016. The median age was 50 years, over 70% of the patients had nonsquamous histology and approximately 20% of the patients had PD-L1 positive status (1% or more by IHC) confirmed. The median followup was 12.1 months. Measurable disease (defined by Response Evaluation Criteria in Solid Tumors – RECIST version 1.1) on at least two CT scans before treatment and one CT scan during treatment, was required. HyperProgressive Disease (HPD) was defined as disease progression on the first CT scan during treatment with an absolute increase in Tumor Growth Rate exceeding 50%. The Primary end point was assessment of the HyperProgressive Disease rate in patients treated with Immunotherapy or chemotherapy.
Among those treated with PD-1/PD-L1 inhibitors, HyperProgressive Disease was noted in 13.8% of patients. HPD was significantly associated with more than two metastatic sites prior to treatment with PD-1/PD-L1 inhibitors, compared with those without HPD (62.5% versus 42.6%; P=0.006). However, baseline tumor burden and number of previous lines of therapy did not make a significant difference. Patients experiencing HPD within the first 6 weeks of beginning PD-1/PD-L1 inhibitor therapy had significantly lower median Overall Survival compared with those with progressive disease without HyperProgression at the first evaluation (3.4 months versus 6.2 months; HR=2.18; P=0.003). Pseudoprogression was observed in 4.7% patients.
Among patients treated with single-agent chemotherapy, only 5.1% were classified as having HyperProgressive Disease and the median Overall Survival was 4.5 months in those with HPD and 3.9 months in other patients with progressive disease without HyperProgression at the first evaluation (P=0.60).
The authors concluded that HyperProgressive Disease is more common with PD-1/PD-L1 inhibitors compared with chemotherapy, among previously treated patients with advanced NSCLC, and is also associated with high number of metastatic sites at baseline and poor survival. They added that the present study is the largest analysis exploring HPD to date and is the first conducted, in a dedicated NSCLC population, with a control cohort of chemotherapy-treated patients Hyperprogressive Disease in Patients With Advanced Non–Small Cell Lung Cancer Treated With PD-1/PD-L1 Inhibitors or With Single-Agent Chemotherapy. Ferrara R, Mezquita L, Texier M, et al. JAMA Oncol. Published online September 6, 2018. doi:10.1001/jamaoncol.2018.3676
KEYTRUDA® (Pembrolizumab)
The FDA on August 20, 2018 approved KEYTRUDA® in combination with ALIMTA® (Pemetrexed) and Platinum as first-line treatment of patients with metastatic, Non-Squamous Non-Small Cell Lung Cancer (NSCLC), with no EGFR or ALK genomic tumor aberrations. KEYTRUDA® is a product of Merck & Co., Inc.
Tumor Mutation Burden is a Predictive Biomarker for Response to Immune Checkpoint Inhibitors
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2018 about 234,030 new cases of lung cancer will be diagnosed and over 154,050 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Patients with advanced NSCLC (Non-Small Cell Lung Cancer) often receive either platinum-doublet chemotherapy combination as first line therapy or KEYTRUDA® (Pembrolizumab) if the tumor PD-L1 expression is 50% or more. About 20-25% of patients benefit from immunotherapy. Other biomarkers besides PD-L1 are needed, to select appropriate patients for immunotherapy.
Tumor Mutational Burden (TMB) has recently emerged as a potential biomarker for immunotherapy with anti PD-1 antibodies. TMB can be measured using Next-Generation Sequencing (NGS) and is defined as the number of somatic, coding base substitutions and short insertions and deletions (indels) per megabase of genome examined. In a previously published trial (CheckMate 568), patients most likely to have a response to a combination of OPDIVO® (Nivolumab) plus YERVOY® (Ipilimumab), irrespective of tumor PD-L1 expression level in NSCLC, had a TMB of at least 10 mutations per megabase. This was the basis for CheckMate 227, which evaluated the efficacy of OPDIVO® and OPDIVO®-based regimens, as first line treatment in biomarker-selected groups of patients with advanced NSCLC.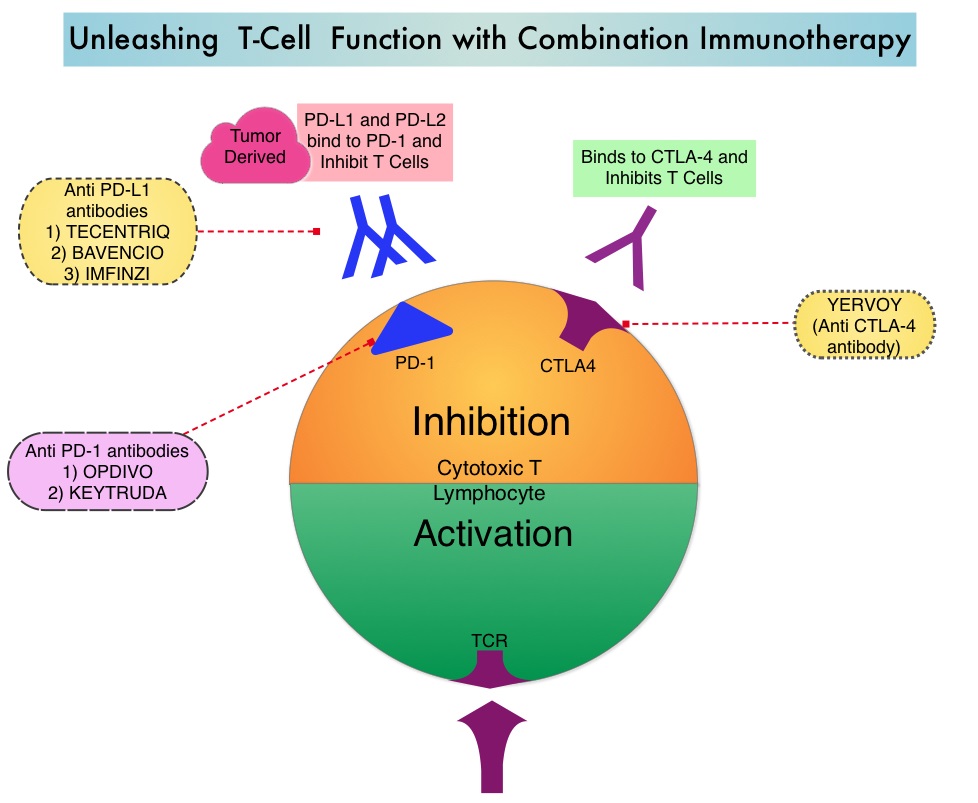
OPDIVO® is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, whereas YERVOY® is a fully human immunoglobulin G1 monoclonal antibody that blocks Immune checkpoint protein/receptor CTLA-4(Cytotoxic T-Lymphocyte Antigen 4, also known as CD152). Blocking the Immune checkpoint proteins unleashes the T cells, resulting in T cell proliferation, activation and a therapeutic response. The complementary mechanisms of action of OPDIVO® and YERVOY® combination resulted in greater efficacy in phase I trials, compared with OPDIVO® monotherapy.
CheckMate 227 is a three part, open-label, randomized, phase III trial, designed to compare different OPDIVO® -based regimens with chemotherapy in distinct patient populations. This study enrolled 1,739 patients with previously untreated Stage IV or recurrent NSCLC with no known sensitizing EGFR or ALK mutations and patients were randomized in a 1:1:1 ratio and the comparison was between either OPDIVO®, OPDIVO® plus YERVOY® or OPDIVO® plus platinum-doublet chemotherapy and platinum-doublet chemotherapy alone. Patients were stratified according to tumor histology and PD-L1 expression of 1% or more (positive) or less than 1% (negative). The study incorporated Tumor Mutational Burden (TMB) as a biomarker. This was determined by the FoundationOne CDx assay, an FDA approved test for molecular profiling, using the validated cutoff of TMB of 10 or more mutations/megabase as High, and less than 10 mutations/megabase as Low.
The authors in this publication reported data from part 1 of this study, which was a comparison between OPDIVO® plus YERVOY® versus chemotherapy, in patients with previously untreated Stage IV or recurrent NSCLC. In this comparison, 139 TMB-High patients were treated with OPDIVO® 3 mg/kg IV every 2 weeks plus YERVOY® 1 mg/kg IV every 6 weeks, whereas 160 TMB-High patients received chemotherapy, based on tumor histology. All treatments were continued until disease progression or unacceptable toxicity. Part 1 of the study had two Coprimary end points. One Coprimary end point was Progression Free Survival (PFS) with OPDIVO® plus YERVOY® versus chemotherapy in a patient population selected on the basis of TMB. The other Coprimary end point was Overall Survival (OS) with OPDIVO® plus YERVOY® versus chemotherapy in a patient population selected on the basis of the PD-L1 expression level.
It was noted that the PFS among patients with High TMB was significantly longer with OPDIVO® plus YERVOY®, compared with chemotherapy. The median PFS with the immunotherapy combination was 7.2 months compared to 5.5 months with chemotherapy (HR=0.58; P<0.001). This represented a 42% reduction in the risk of disease progression or death. The 1 year PFS more than tripled with combination immunotherapy at 42.6% versus 13.2% with chemotherapy. The Objective Response Rate (ORR) was 45.3% with immunotherapy combination and 26.9% with chemotherapy. The improved outcomes with OPDIVO® plus YERVOY® over chemotherapy was broadly consistent within all subgroups and was independent of tumor histology and PD-L1 expression. There was a clear trend toward improved survival with the immunotherapy combination although this data is immature. Grade 3 or 4 treatment related adverse events were 31.2% with immunotherapy combination and 36.1% with chemotherapy.
The authors concluded that this is the first phase III study to evaluate Tumor Mutational Burden as a predictive biomarker for immunotherapy as a coprimary endpoint. They added that these results highlight that Tumor Mutational Burden and PD-L1 are independent biomarkers and TMB is predictive of benefit with OPDIVO® plus YERVOY® irrespective of PD-L1 expression. TMB-High therefore is a new biomarker and represents a distinct subgroup of NSCLC. Nivolumab plus Ipilimumab in Lung Cancer with a High Tumor Mutational Burden. Hellmann MD, Ciuleanu TE, Pluzanski A, et al. N Engl J Med 2018; 378:2093-2104
First Line TECENTRIQ® plus Chemotherapy in Advanced Squamous NSCLC
Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers and 30% are Squamous Cell Carcinomas (SCC). Non Small Cell Lung Cancer patients with Squamous Cell histology have been a traditionally hard- to-treat, patient group, and less than 15% of patients with advanced Squamous NSCLC survive a year after diagnosis and less than 5% of patients survive for five years or longer. IMpower131 is a multicenter, open-label, phase III study, in which 1021 chemotherapy-naïve patients with stage IV Squamous NSCLC received TECENTRIQ® ((Atezolizumab)) along with Carboplatin, and Paclitaxel, TECENTRIQ® along with Carboplatin, and ABRAXANE® (nab-paclitaxel) or Carboplatin and ABRAXANE® (control group). The addition of TECENTRIQ® to chemotherapy significantly improved median Progression Free Survival across all PD-L1 subgroups. This is the first phase III trial of an immunotherapy-based treatment regimen, to demonstrate a significant improvement in Progression Free Survival, in advanced Squamous NSCLC.
Late Breaking Abstract – ASCO 2018 Blood Test Demonstrates High Specificity for Detection of Early Stage Lung Cancer
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2018 about 234,030 new cases of lung cancer will be diagnosed and over 154,050 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Survival rates however are significantly higher when lung cancer is diagnosed early. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas, and 10% are Large cell carcinomas.
Although the U.S. Preventive Services Task Force (USPSTF) has recommended annual screening for lung cancer with Low-Dose Computed Tomography (LDCT) for individuals with significant smoking history, screening is vastly underutilized, with a screening rate of less than 2% among smokers eligible for screening. Screening for lung cancer using a peripheral blood sample may improve lung cancer screening rates. Analysis of cell-free DNA (cfDNA) from peripheral blood (Liquid Biopsy), is presently approved to select EGFR targeted therapies (cobas EGFR mutation test), in patients with advanced Non Small Cell Lung Cancer. However, the role of cell-free DNA analysis for early detection of lung cancer is not well established.
The Circulating Cell-Free Genome Atlas (CCGA) is a prospective, multi-center, observational study and is the largest study ever initiated, to develop a noninvasive, liquid biopsy assay for early cancer detection, based on cell-free DNA (cfDNA). This study has currently enrolled 10,012 of a planned 15,000 participants, including people with a recent cancer diagnosis and also a control group of individuals with no known malignancy (70% with cancer, 30% without cancer), across 141 sites in the United States and Canada. This report is one of the first pre-planned sub-studies from the CCGA, involving investigation of blood samples from 1,627 participants (878 patients with newly diagnosed untreated cancer including 127 patients with lung cancer and 749 controls – 580 controls and 169 technical assay controls ), across 20 tumor types and all clinical stages.
The cell-free DNA was isolated from the peripheral blood and analyzed using the following three sequencing methods that were designed to detect cancer-defining signals (mutations and other genomic changes), that could be utilized for early cancer detection.
Targeted sequencing to detect somatic (non-inherited) mutations, such as Single Nucleotide Variants and small insertions and/or deletions, in specific sections of the genome.
Whole-Genome Sequencing (WGS) to detect somatic gene copy number changes across the genome.
Whole-Genome Bisulfite Sequencing (WGBS) of cfDNA to detect abnormal patterns of cfDNA methylation (epigenetic changes)
In this initial sub-study, the authors explored the ability of the above three different assays to detect cancer in 127 people with stage I-IV lung cancer. It was noted that biologic signals suggesting lung cancer were detected and comparable across all assays, and the signal increased with cancer stage. At 98% specificity, the Targeted sequencing detected 51% of early-stage (stage I-IIIA) lung cancers and 89% of late-stage (stage IIIB-IV) lung cancers. Whole-Genome Sequencing detected 38% of early-stage cancers and 87% of late-stage cancers. Whole-Genome Bisulfite Sequencing had similar efficacy, detecting 41% of early stage lung cancers and 89% of late-stage cancers. Similar sensitivities were noted across all assays for adenocarcinoma, squamous cell and small cell lung cancer. False positive rates were low. Of the 580 control participants without cancer at study enrollment, less than 1% (five participants) had cancer-like signal across all three assays, of whom two were subsequently diagnosed with cancer. This highlights the potential for these assays to detect early stage cancers. The authors caution that a large proportion of cell-free DNA is derived from White Blood Cells (WBCs) and DNA mutations in the WBC population can also be generated by processes other than cancer such as clonal hematopoiesis during human aging. In this study, signal generated from the WBCs was subtracted resulting in a cleaner signal, only from tumor related variants.
It was concluded that based on the initial results from the CCGA study, it is possible to detect early-stage lung cancer, with a high degree of specificity, from a simple blood test, using genome sequencing. The authors plan to further optimize the assays and validate results in a larger group of people. Genome-wide sequencing for early stage lung cancer detection from plasma cell-free DNA (cfDNA): The Circulating Cancer Genome Atlas (CCGA) study. Oxnard GR, Maddala T, Hubbell E, et al. J Clin Oncol. 2018;36(suppl; abstr LBA8501)