
The FDA on May 26, 2017 granted regular approval to ZYKADIA®, for patients with metastatic Non-Small Cell Lung Cancer (NSCLC), whose tumors are Anaplastic Lymphoma Kinase (ALK)-positive, as detected by an FDA-approved test. ZYKADIA® is a product of Novartis Pharmaceuticals Corp.
Tag: Lung Cancer: Non-Small Cell
KEYTRUDA® (Pembrolizumab)
The FDA on May 10, 2017 granted accelerated approval to KEYTRUDA® in combination with ALIMTA® (Pemetrexed) and Carboplatin for the treatment of patients with previously untreated metastatic Non-Squamous Non-Small Cell Lung Cancer (NSCLC). KEYTRUDA® is a product of Merck and Co., Inc.
FDA Approves TAFINLAR® and MEKINIST® Combination for BRAF Positive Non Small Cell Lung Cancer
SUMMARY: The FDA on June 22, 2017, granted regular approvals to TAFINLAR® (Dabrafenib) and MEKINIST® (Trametinib) administered in combination, for patients with metastatic Non Small Cell Lung Cancer (NSCLC), with BRAF V600E mutation, as detected by an FDA-approved test. These are the first FDA approvals specifically for treatment of patients with BRAF V600E mutation-positive metastatic NSCLC.
The FDA also approved the Oncomine® Dx Target Test, a next generation sequencing (NGS) test to detect multiple gene mutations for lung cancer in a single test from a single tissue specimen. This test detects the presence of BRAF, ROS1, and EGFR gene mutations or alterations in tumor tissue of patients with NSCLC. This test can be used to select patients with NSCLC with the BRAF V600E mutation for treatment with the combination of TAFINLAR® and MEKINIST®. This is the first NGS oncology panel test approved by the FDA for multiple companion diagnostic indications.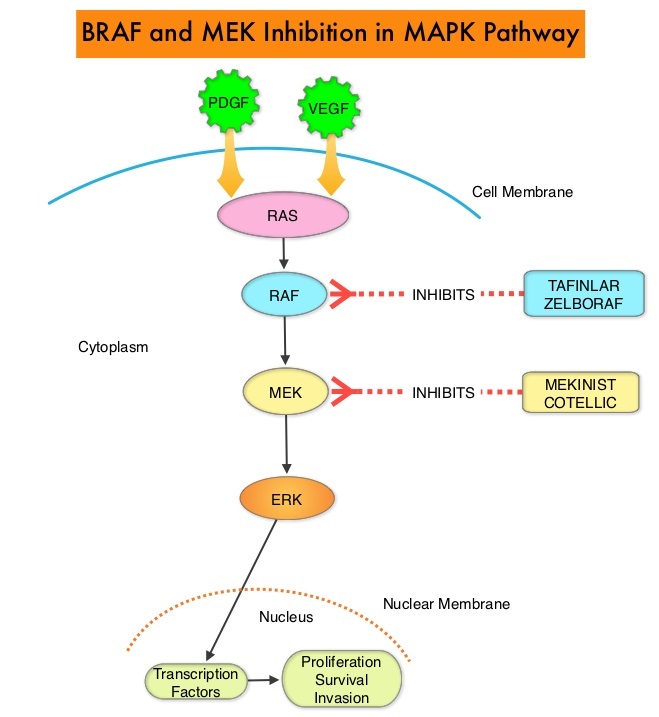
Combining MEKINIST® (Trametinib) with TAFINLAR® (Dabrafenib) to treat patients with NSCLC, was based on the understanding of the biological pathways of this malignancy. The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. This pathway has been implicated in the development of multiple malignancies including NSCLC and Melanoma. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. BRAF mutations have been demonstrated in 6-8% of all malignancies. TAFINLAR® is a selective oral BRAF inhibitor and MEKINIST® is a potent and selective inhibitor of MEK gene, which is downstream from RAF in the MAPK pathway.
The approval of TAFINLAR® and MEKINIST® combination, for patients with metastatic NSCLC was based on an international, multicenter, three-cohort, non-randomized, open-label trial, in patients with locally confirmed BRAF V600E mutation-positive, metastatic NSCLC. In this phase II trial, 93 patients were treated with the combination of TAFINLAR® 150 mg orally twice daily and MEKINIST® 2 mg orally once daily. Of these 93 patients, 36 patients had received no prior systemic therapy for metastatic NSCLC and 57 patients received at least one prior platinum-based chemotherapy regimen and had disease progression. The third cohort in this phase II trial included 78 previously treated patients with BRAF V600E mutation-positive metastatic NSCLC, who received single-agent TAFINLAR®. The primary endpoint was Overall Response Rate (ORR).
It was noted that in the previously treated group, the ORR for the combination treatment based on independent review was 63% with a median Duration of Response of 12.6 months. In the treatment-naive group, the ORR for the combination was 61% and this group had not reached the endpoint for median Duration of Response and therefore was not estimable. However, among those who responded to treatment, 59% of the responders had response durations greater than 6 months. The ORR for patients who received single agent TAFINLAR® was 27% and the median Duration of Response was 9.9 months. The most common Grade 3-4 adverse reactions were pyrexia, fatigue, dyspnea, vomiting, rash, hemorrhage, and diarrhea.
It was concluded that TAFINLAR® plus MEKINIST® combination represents a new targeted therapy for patients with BRAF V600E mutation¬-positive metastatic NSCLC, who tend to respond less favorably to standard chemotherapy. This approval marks the fourth actionable genomic biomarker in metastatic NSCLC along with EGFR, ALK and ROS-1. Dabrafenib plus trametinib in patients with previously treated BRAF(V600E)-mutant metastatic non-small cell lung cancer: an open-label, multicentre phase 2 trial. Planchard D, Besse B, Groen HJ et al. Lancet Oncol. 2016 Jul;17(7):984-93. doi: 10.1016/S1470-2045(16)30146-2. Epub 2016 Jun 6.
Late Breaking Abstract – ASCO 2017 Dacomitinib Superior to IRESSA® in EGFR Mutant Non-Small Cell Lung Cancer
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2017 about 222,500 new cases of lung cancer will be diagnosed and over 155,000 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 25% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large cell carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer. Approximately 10% to 15% of Caucasian patients and 50% of Asian patients with Adenocarcinomas, harbor activating EGFR (Epidermal Growth Factor Receptor) mutations and 90% of these mutations are either Exon 19 deletions or L858R point mutations in Exon 21. EGFR Tyrosine Kinase Inhibitors (TKIs) such as TARCEVA® (Erlotinib), IRESSA® (Gefitinib) and GILOTRIF® (Afatinib), have demonstrated a 60% to 70% response rate as monotherapy when administered as first line treatment, in patients with metastatic NSCLC, who harbor the sensitizing EGFR mutations.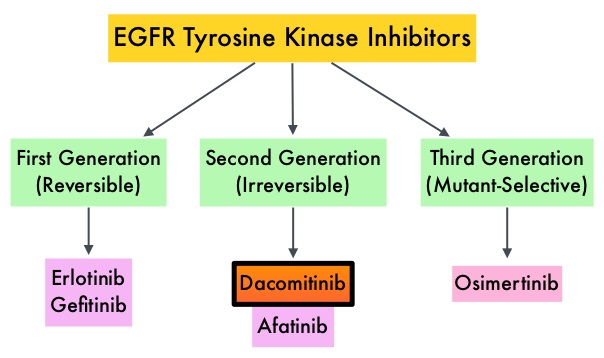
Dacomitinib is a potent, irreversible, second-generation EGFR Tyrosine Kinase Inhibitor and inhibits three members of the ErbB protein family, including EGFR/HER1, HER2 and HER4. Based on the encouraging clinical activity of Dacomitinib in treatment naïve patients with advanced NSCLC, harboring activating EGFR mutations, in a phase II study (The Lancet Oncology 2014;15:1433-1441), the authors conducted a randomized phase III trial, comparing Dacomitinib with IRESSA®, as first line therapy in this patient population . This study (ARCHER 1050) randomized 452 patients in a 1:1 ratio to either receive Dacomitinib 45 mg PO daily (N=227) or IRESSA® 250 mg PO daily (N=225). Eligible patients had newly diagnosed stage IIIB/IV or recurrent NSCLC, harboring an activating EGFR mutation (Exon 19 deletions or L858R point mutations in Exon 21, with or without Exon 20 T790M mutations). Treatments groups were well balanced and patients were stratified by race and EGFR mutation subtype. The Primary endpoint was Progression Free Survival (PFS) and Secondary endpoints included Overall Survival (OS), Objective Response Rate (ORR) and Duration of Response (DoR).
The median PFS for patients who received Dacomitinib was 14.7 months compared with 9.2 months for the group who received IRESSA® (HR=0.59; P<0.0001). This meant a 41% reduction in the risk of cancer progression or death with Dacomitinib compared with IRESSA®. The median Duration of Response was 14.8 months with Dacomitinib versus 8.3 months with IRESSA® (HR= 0.40; P<0.0001). As expected, patients in the Dacomitinib group experienced more side effects such as skin rash and diarrhea and this has been attributed to the stronger suppression of the EGFRs in the normal healthy tissues.
The authors concluded that ARCHER 1050 is the first phase III trial comparing EGFR TKIs head-to-head, and this study demonstrated clinically meaningful superiority of Dacomitinib, when compared to IRESSA®, in treatment naïve NSCLC patients, with activating EGFR mutations. Further, the PFS achieved with Dacomitinib in this study is among the highest observed, when compared with other EGFR Tyrosine Kinase Inhibitors, for this cancer type. Dacomitinib versus gefitinib for the first-line treatment of advanced EGFR mutation positive non-small cell lung cancer (ARCHER 1050): A randomized, open-label phase III trial. Mok T, Cheng Y, Zhou X, et al. J Clin Oncol 35, 2017 (suppl; abstr LBA9007)
Late Breaking Abstract – ASCO 2017 ALECENSA® Superior to XALKORI® in Untreated ALK-Positive Non Small Cell Lung Cancer
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2017 about 222,500 new cases of lung cancer will be diagnosed and over 155,000 patients will die of the disease. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 25% are Squamous cell carcinomas, 40% are Adenocarcinomas and 10% are Large cell carcinomas. The discovery of rearrangements of the Anaplastic Lymphoma Kinase (ALK) gene in some patients with advanced NSCLC and adenocarcinoma histology, led to the development of agents such as XALKORI® (Crizotinib), ZYKADIA® (Ceritinib), ALECENSA® (Alectinib) and now ALUNBRIG® (Brigatinib), with promising results. It has become clear that appropriate, molecularly targeted therapy for tumors with a molecular abnormality, results in the best outcomes. According to the US Lung Cancer Mutation Consortium (LCMC), two thirds of patients with advanced adenocarcinoma of the lung, have a molecular driver abnormality. The most common oncogenic drivers in patients with advanced adenocarcinoma of the lung are, KRAS in 25%, EGFR in 21% and ALK in 8% as well as other mutations in BRAF, HER2, AKT1 and fusions involving RET and ROS oncogenes. These mutations are mutually exclusive and the presence of two simultaneous mutations, are rare.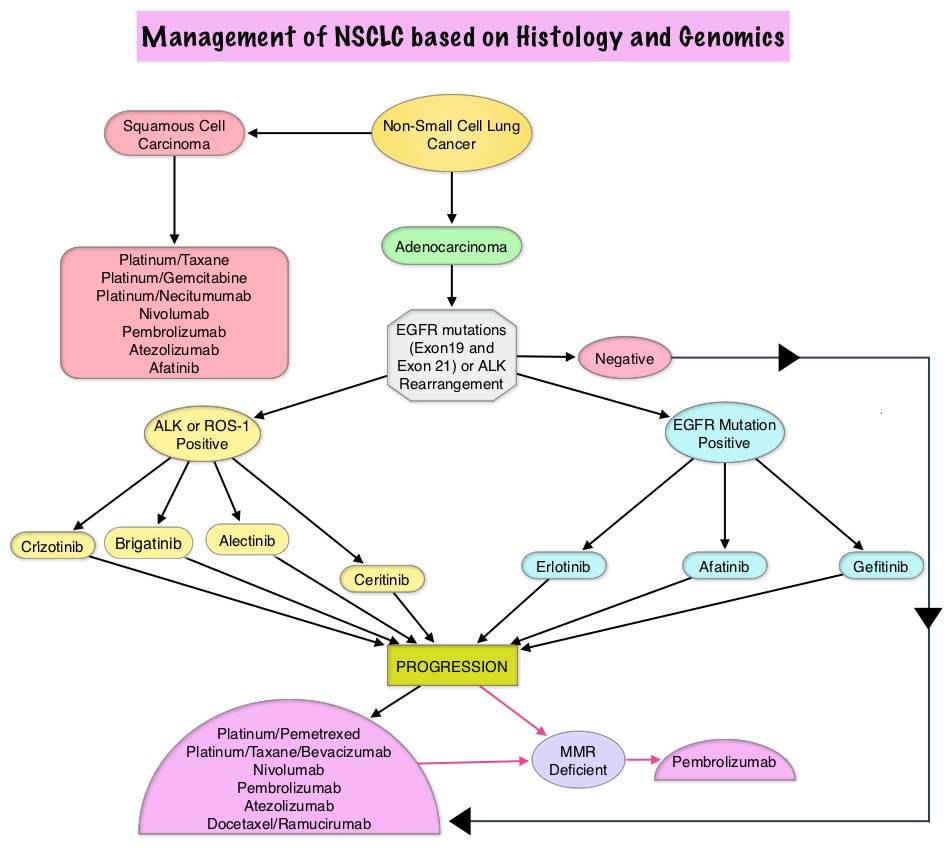
Patients with advanced NSCLC harboring ALK gene rearrangements often receive XALKORI® as first line therapy and can expect a median Progression Free Survival of approximately 11 months. These patients however are at a high lifetime risk of CNS metastases. ALECENSA® (Alectinib) is a potent ALK Tyrosine Kinase Inhibitor, and is effective against several ALK mutations that confer resistance to XALKORI® Further, unlike XALKORI®, ALECENSA® can cross the blood-brain barrier and is not a substrate of P-glycoprotein, a key efflux transporter located at the blood-brain barrier.
The ALEX trial is an international, randomized, open-label, phase III study which compared ALECENSA® with XALKORI®, in patients with previously untreated, advanced ALK-positive NSCLC, including those with asymptomatic CNS disease. In this trial, 303 previously untreated patients were randomly assigned in a 1:1 ratio to receive ALECENSA® at 600 mg twice daily (N=152) or XALKORI® at 250 mg PO twice daily (N=151). Treatment was continued until disease progression or unacceptable toxicities. Patients with isolated asymptomatic CNS progression could receive a local therapy at the investigator’s discretion, followed by continued trial treatment until systemic disease progression. Patients were stratified and the primary end point was Investigator-assessed Progression Free Survival. Secondary end points were Independent Review Committee (IRC)–assessed Progression Free Survival, time to CNS progression, Objective Response Rate, and Overall Survival.
At the time of primary analysis, ALECENSA® was significantly superior to XALKORI®, reducing the risk of progression/death by 53% (HR= 0.47; P<0.0001). The median PFS for ALECENSA® was Not Reached versus 11.1 months for XALKORI®. The median Progression Free Survival assessed by the IRC was 25.7 months for ALECENSA® vs 10.4 months for XALKORI® (HR=0.50, P< 0.001). The magnitude of the benefit with ALECENSA® was generally consistent across all the subgroups although this benefit was lower in the subgroups of active smokers and patients with poor Performance Status. Objective Response Rate was 82.9% in the ALECENSA® group versus 75.5% in the XALKORI® group (P=0.09). The rate of CNS progression was 12% in the ALECENSA® group compared with 45% in the XALKORI® group (HR=0.16; P<0.001). Among patients with measurable or non-measurable CNS lesions at baseline, a CNS response occurred in 59% of the patients in the ALECENSA® group versus 26% in the XALKORI® group. Further, 45% of the patients in the ALECENSA® group had a complete CNS response, as compared with 9% in the XALKORI® group. Grade 3-5 adverse events were less frequent with ALECENSA® (41%) versus 50% with XALKORI®.
It was concluded that ALECENSA® showed superior efficacy and lower toxicity compared with XALKORI®, and should be a new standard of care for treatment-naïve patients with ALK-positive NSCLC. Alectinib versus crizotinib in treatment-naive advanced ALK-positive non–small cell lung cancer (NSCLC): primary results of the global phase III ALEX study. Shaw AT, Peters S, Mok T, et al. J Clin Oncol. 2017;35 (suppl; abstr LBA9008).
FDA Approves KEYTRUDA® in Combination with Chemotherapy as First-Line Treatment for Metastatic NSCLC
SUMMARY: The FDA on May 10, 2017 granted accelerated approval to KEYTRUDA® (Pembrolizumab) in combination with ALIMTA® (Pemetrexed) and Carboplatin, for the treatment of patients with previously untreated metastatic non-squamous Non Small Cell Lung Cancer (NSCLC). Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. The American Cancer Society estimates that for 2017 about 222,500 new cases of lung cancer will be diagnosed and over 155,000 patients will die of the disease. Non Small Cell Lung Cancer accounts for approximately 85% of all lung cancers. The FDA in October 2016, approved KEYTRUDA® for the treatment of patients with metastatic NSCLC, whose tumors have high PD-L1 expression (Tumor Proportion Score greater than or equal to 50%), as determined by an FDA-approved test, with no EGFR or ALK genomic tumor aberrations, and no prior systemic chemotherapy treatment for metastatic NSCLC.
KEYTRUDA® is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. High level of Programmed Death-Ligand 1 (PD-L1) expression is defined as 
ALUNBRIG® (Brigatinib)
The FDA on April 28, 2017 granted accelerated approval to ALUNBRIG ® tablets for the treatment of patients with metastatic Anaplastic Lymphoma Kinase (ALK)-positive Non-Small Cell Lung Cancer (NSCLC), who have progressed on or are intolerant to XALKORI® (Crizotinib). ALUNBRIG® is a product of Takeda Pharmaceutical Company Limited, through its wholly owned subsidiary ARIAD Pharmaceuticals, Inc.
TAGRISSO® (Osimertinib)
The FDA on March 30, 2017 granted regular approval to TAGRISSO®, for the treatment of patients with metastatic Epidermal Growth Factor Receptor (EGFR) T790M mutation-positive Non-Small Cell Lung Cancer (NSCLC), as detected by an FDA-approved test, whose disease has progressed on or after EGFR Tyrosine Kinase Inhibitor (TKI) therapy. TAGRISSO® is marketed by AstraZeneca Pharmaceuticals, LP.
FDA Approves ALUNBRIG® for ALK Positive Non Small Cell Lung Cancer
SUMMARY: The FDA on April 28, 2017 granted accelerated approval to ALUNBRIG® (Brigatinib),for the treatment of patients with metastatic Anaplastic Lymphoma Kinase (ALK)-positive Non Small Cell Lung Cancer (NSCLC), who have progressed on or are intolerant to XALKORI® (Crizotinib). Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers. It is the leading cause of cancer death among both men and women. The American Cancer Society estimates that over 222,500 new cases of lung cancer will be diagnosed in the United States in 2017 and over 155,870 patients will die of the disease. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 25% are Squamous Cell Carcinomas, 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. The discovery of rearrangements of the Anaplastic Lymphoma Kinase (ALK) gene in some patients with advanced NSCLC and adenocarcinoma histology, led to the development of agents such as XALKORI® (Crizotinib), ZYKADIA® (Ceritinib), ALECENSA® (Alectinib) and now ALUNBRIG® (Brigatinib), with promising results. It has become clear that appropriate, molecularly targeted therapy for tumors with a molecular abnormality, results in the best outcomes. According to the US Lung Cancer Mutation Consortium (LCMC), two thirds of patients with advanced adenocarcinoma of the lung, have a molecular driver abnormality. The most common oncogenic drivers in patients with advanced adenocarcinoma of the lung are, KRAS in 25%, EGFR in 21% and ALK in 8% as well as other mutations in BRAF, HER2, AKT1 and fusions involving RET and ROS oncogenes. These mutations are mutually exclusive, and the presence of two simultaneous mutations are rare.
The approval was based on findings from the ALTA trial, which is a pivotal, open-label multicenter study in which 222 patients were randomized 1:1 ratio to receive ALUNBRIG® 90 mg orally once daily (N=112) or 180 mg once daily following a 7-day lead-in at 90 mg orally once daily (N=110). Two dose regimens were evaluated in this study, as clinical responses and Adverse Events varied with starting dose of ALUNBRIG®, in a previous Phase I/II study. Eligible patients had locally advanced or metastatic ALK-positive NSCLC, who had progressed on XALKORI®. The median age of patients across the study was 54 years and 67% of the patients had brain metastases. Patients were stratified by presence of brain metastases at baseline and best response to prior treatment with XALKORI®. The Primary endpoint was Objective Response Rate (ORR) and Secondary endpoints included Progression Free Survival (PFS) and CNS response.
The ORR was 48% in the 90 mg dose group and 53% in the 180 mg dose group. After a median duration of follow up of 8 months, median duration of response was 13.8 months in both treatment groups. In patients with measurable brain metastases at baseline, intracranial ORR was 42% in the 90 mg group and 67% in the 180 mg group. Among patients who exhibited an intracranial response, 78% of patients in the 90 mg group and 68% of patients in the 180 mg group maintained an intracranial response for at least 4 months. The median PFS was 8.8 months in the 90 mg dose group, and 11.1 months in the 180mg dose group. The most common adverse reactions, were nausea, diarrhea, fatigue, cough, and headache. The most common serious adverse reactions were pneumonia and pneumonitis.
The authors concluded that treatment with ALUNBRIG® resulted in significant response rates and improved Progression Free Survival, with acceptable toxicity profile. The recommended dosing regimen of ALUNBRIG® is 90 mg orally once daily for the first 7 days and if tolerated, the dose is increased to 180 mg orally once daily.
Kim D-W, Tiseo M, Ahn M-J, et al. Brigatinib (BRG) in patients (pts) with crizotinib (CRZ)-refractory ALK+ non-small cell lung cancer (NSCLC): First report of efficacy and safety from a pivotal randomized phase (ph) 2 trial (ALTA). J Clin Oncol. 2016;34 (suppl; abstr 9007).
Reduced Lung-Cancer Mortality with Low-Dose Computed Tomographic Screening
SUMMARY: The rationale for Lung Cancer screening is based on the National Lung Cancer Screening Trial (NLST) in which the use of low dose CT scan in high risk, healthy patients, resulted in a 20% reduction in lung cancer mortality, compared to screening with a chest x-ray. It is important that eligible people who are smokers participate in a smoking cessation program and quit smoking. Further, those eligible for screening should understand the limitations associated with any screening methodology and potential risks associated with procedures that may follow a false positive result.
Lung cancer screening is performed using a non-contrast low dose CT scan. Criteria for lung cancer screening include-
1) People 55-74 years of age with no signs or symptoms of lung cancer
2) Current or former smoker with a 30 pack year smoking history (Number of years smoked multiplied by the number of packs of cigarettes per day)
3) Current smokers are strongly urged to enter a smoking cessation program
4) Former smokers must have quit smoking within the past 15 years
People with serious comorbid conditions, those on home oxygen and individuals with metallic devices or implants in the chest or back (which can interfere with the scan) should be excluded from lung cancer screening. Lung cancer screening with low dose CT scan is presently not covered by most insurance plans. The National Lung Screening Trial Research Team. N Engl J Med 2011; 365:395-409