
The FDA on October 9, 2015 approved OPDIVO® for the treatment of patients with metastatic Non Small Cell Lung Cancer (NSCLC), with progression on or after Platinum-based chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations, prior to receiving OPDIVO®. OPDIVO® Injection is a product of Bristol-Myers Squibb Company.
Tag: Lung Cancer: Non-Small Cell
FDA Approves TAGRISSO®, a Third Generation TKI, for EGFR T790M-Positive Non Small Cell Lung Cancer
SUMMARY: The U.S. FDA granted accelerated approval to TAGRISSO® (Osimertinib), for the treatment of patients with metastatic Epidermal Growth Factor Receptor (EGFR) T790M mutation-positive Non Small Cell Lung Cancer (NSCLC), as detected by an FDA-approved test, who had progressed on or after EGFR Tyrosine Kinase Inhibitor (TKI) therapy. Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. It is the leading cause of cancer death among both men and women. The American Cancer Society estimates that over 221,200 new cases of lung cancer will be diagnosed in the United States in 2015 and over 158,000 patients will die of the disease. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large cell carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer. Approximately 10% to 15% of Caucasian patients and 50% of Asian patients with Adenocarcinomas, harbor activating EGFR (Epidermal Growth Factor Receptor) mutations and 90% of these mutations are either Exon 19 deletions or L858R point mutations in Exon 21. EGFR Tyrosine Kinase Inhibitors (TKIs) such as TARCEVA® (Erlotinib), IRESSA® (Gefitinib) and GILOTRIF® (Afatinib), have demonstrated a 60% to 70% response rate as monotherapy when administered as first line treatment, in patients with metastatic NSCLC, who harbor the sensitizing EGFR mutations. However, majority of these patients experience disease progression within 9 to 14 months. This resistance to frontline EGFR TKI therapy has been attributed to acquired T790M “gatekeeper” point mutation in EGFR, identified in 50% – 60% of patients. The approval of TAGRISSO® was based on two multicenter, single arm, open label clinical trials (AURA and AURA2), in patients with metastatic EGFR T790M mutation-positive NSCLC, who had progressed on prior systemic therapy, including an EGFR TKI.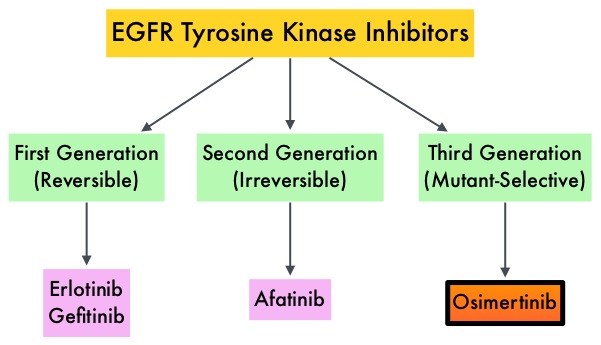
In the AURA dose escalation/expansion study (Study 1), 201 patients with EGFR mutation-positive advanced NSCLC received TAGRISSO® 80 mg PO daily until disease progression. Tumor samples were taken from all patients after disease progression on the most recent line of therapy, for prospective confirmation of T790M positive status by central laboratory testing, before enrollment. The median age was 62 years. The primary endpoint was Objective Response Rate (ORR) and secondary endpoints included Disease Control Rate (DCR), duration of response (DoR) and Progression Free Survival (PFS). The ORR in an updated analysis at the 2015 WCLC was 61% and DCR was 92%. The ORRs were similar across all lines of therapy, ie. Second line vs third line or more. The median DoR and median PFS have not been reached.
In the AURA2 Phase II study, 210 patients with locally advanced or metastatic NSCLC received TAGRISSO® 80 mg PO daily until disease progression. All eligible patients progressed on a previous EGFR TKI treatment and had a mandatory tumor sample taken after disease progression on the most recent line of therapy, for confirmation of T790M positive status by central laboratory testing. The median age was 64 years. The primary endpoint was Objective Response Rate (ORR) and secondary end points included Disease Control Rate (DCR), Duration of Response (DoR), Progression Free Survival (PFS), and safety. The ORR in an updated analysis presented at the 2015 WCLC was 71%, with 2 complete responses. The stable disease rate at 6 weeks or more was 21%, for a Disease Control Rate of 92%. The median Duration of Response was 7.8 months. The median Progression Free Survival (PFS) was 8.6 months.
Grade 1-2 toxicities from these two trials, which included a total of 411 patients included diarrhea, rash, dry skin, nail toxicity, eye disorders, nausea, decreased appetite and constipation. From these two studies it was concluded that TAGRISSO® is a new treatment option for patients who test positive for the EGFR resistance mutation, T790M, with significant response rates noted in over 50% of the treated patients. AZD9291 in pre-treated T790M positive advanced NSCLC: AURA2 Phase II study. Mitsudomi T, Tsai C, Shepherd F, et al. Presented at: 16th World Conference on Lung Cancer; September 6-9; Denver, CO. Abstract 1406.
KEYTRUDA® (Pembrolizumab)
The FDA on October 2, 2015 granted accelerated approval to KEYTRUDA® for the treatment of patients with metastatic Non-Small Cell Lung Cancer (NSCLC) whose tumors express Programmed Death Ligand 1 (PD-L1) as determined by an FDA-approved test, with disease progression on or after platinum-containing chemotherapy. KEYTRUDA® Injection is a product of Merck Sharp and Dohme Corporation.
FDA Approves KEYTRUDA® for Advanced Lung Cancer
SUMMARY: The FDA granted accelerated approval to KEYTRUDA® (Pembrolizumab), for the treatment of patients with metastatic Non Small Cell Lung Cancer (NSCLC), whose tumors express Programmed Death Ligand 1 (PD-L1), as determined by an FDA-approved test, following disease progression on or after platinum-containing chemotherapy. Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. It is the leading cause of cancer death among both men and women. The American Cancer Society estimates that over 221,200 new cases of lung cancer will be diagnosed in the United States in 2015 and over 158,000 patients will die of the disease. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers.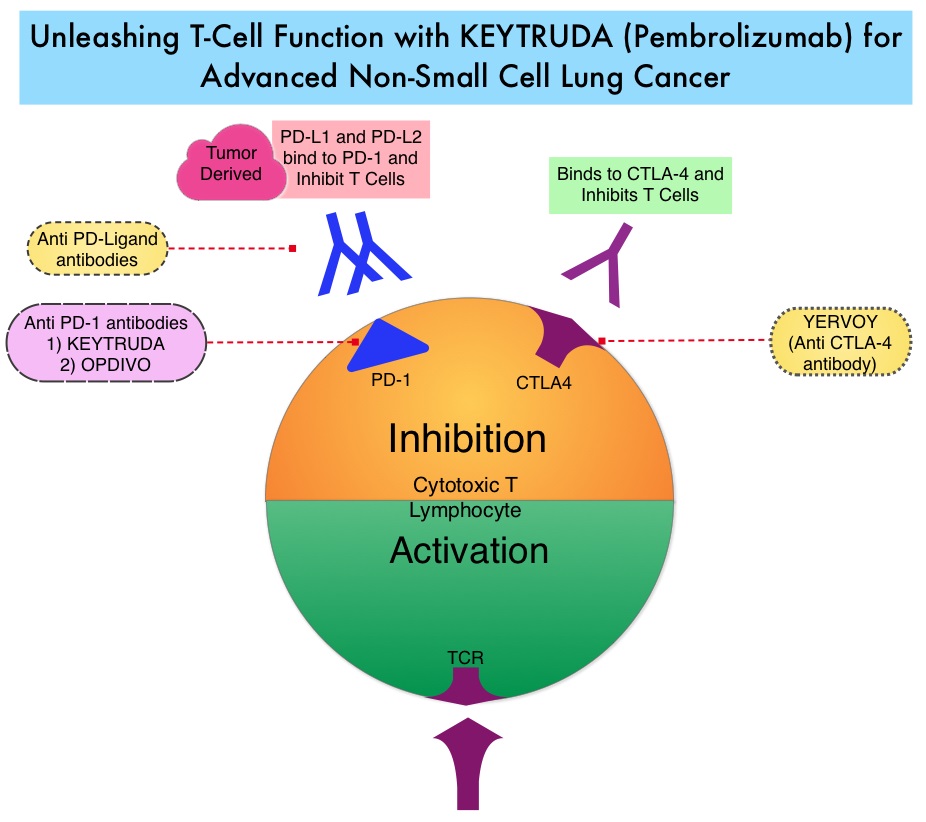
The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of the Immune checkpoints. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, Immune checkpoints or gate keepers, switch off the T cells of the immune system and thereby inhibit an intense immune response. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies have been developed, that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. Targeting Immune checkpoints unleashes the T cells, resulting in T cell proliferation, activation and a therapeutic response. KEYTRUDA® is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells.
In this publication, the authors assessed the efficacy and safety of KEYTRUDA® in patients with advanced NSCLC enrolled in the KEYNOTE-001 phase I trial. Four Hundred and Ninety five (N=495) patients were assigned to either a training group (N=182) or a validation group (N=313) and KEYTRUDA® was administered at three dosages: 2 mg/kg IV every 3 weeks, 10 mg/kg IV every 3 weeks, or 10 mg/kg IV every 2 weeks. Patient responses were assessed every 9 weeks.
The Objective Response Rate (ORR) in the entire study population was 19.4%, the median Duration of Response was 12.5 months, the median Progression Free Survival was 3.7 months and the median Overall Survival was 12.0 months. The PD-L1 (Programmed Death-Ligand 1) expression was evaluated in 204 patients in the validation group by ImmunoHisto Chemistry (IHC) and membrane PD-L1 expression of 50% or more, in tumor cells, was selected as the cutoff. It was noted that among patients with PD-L1 expression in at least 50% of tumor cells, the Objective Response Rate was 45.2%, median Progression Free Survival was 6.3 months and median Overall Survival has not been reached. Responses were not as robust in those patients with tumors demonstrating less than 50% PD-L1 expression, but in those who did respond, the duration of responses were comparable to those with 50% or more PD-L1 expression. KEYTRUDA® was well tolerated overall and the common immune mediated adverse events were infusion reactions, hypothyroidism and pneumonitis.
The authors concluded that KEYTRUDA® showed significant antitumor activity in patients with advanced Non Small Cell Lung Cancer, whose tumor PD-L1expression was 50% or more. Further, the median duration of response exceeded 12 months among responders, regardless of the degree of PD-L1 expression. This study validated that PD-L1 expression in tumors is clearly a marker of response to KEYTRUDA®. Pembrolizumab for the Treatment of Non–Small-Cell Lung Cancer. Garon EB, Rizvi NA, Hui R, et al. N Engl J Med 2015; 372:2018-2028
Stereotactic Body Radiation Therapy (SBRT) Instead of Surgery for Patients with Early Stage Inoperable or Advanced Oligometastatic NSCLC
SUMMARY: Stereotactic RadioSurgery (SRS) is a non-surgical procedure that allows delivery of significantly higher doses of precisely focused radiation to the tumor, compared to conventional radiation therapy, with less collateral damage to the surrounding normal tissue. The technologies used for SRS include GAMMA KNIFE® which uses highly focused gamma rays, Proton Beam therapy which uses ionized hydrogen or Protons, Linear Accelerator (LINAC) and CYBER KNIFE® which use Photons, to target the tumor tissue. Stereotactic Body Radiation Therapy (SBRT) refers to stereotactically guided radiation therapy delivered over several days. Because SBRT is fractionated and is offered in three precise treatments, the short-and long-term side effects of radiation therapy are decreased and may allow higher total dosage to be given.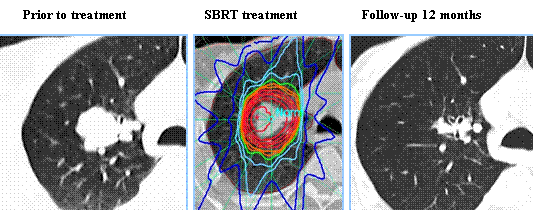
SBRT is a viable option for elderly and frail patients and those with comorbidities or those who decline surgery. Two studies presented at the 56th Annual Meeting of the American Society for Radiation Oncology (ASTRO) have provided convincing evidence in favor of SBRT in patients with inoperable early-stage lung cancer and for patients with oligometastatic stage IV Non Small Cell Lung Cancer (NSCLC). RTOG 0236 is a phase II trial in which 59 frail, elderly patients with early stage, medically inoperable Stage I Non Small Cell Lung Cancer received SBRT in three fractions of 18 Gy (total of 54 Gy) over a period of 10 days to 2 weeks. The median age was 72 years and these patients had multiple comorbidities that precluded them from curative surgery. The primary end point was 2-year actuarial primary tumor control. Secondary end points included Disease Free Survival (i.e., primary tumor, involved lobe, regional, and disseminated recurrence), treatment-related toxicity and Overall Survival. At 5 years, the Disease Free Survival and Overall Survival were 26% and 40%, respectively and the median Overall Survival was 4 years. The 5-year primary tumor and involved lobe (local) failure rate was 20%, local-regional failure rate was 38% and disseminated failure rate was 31%. In a second study, Ashworth and colleagues reported the individual patient data meta-analysis, which included 757 patients diagnosed with stage IV NSCLC at 20 cancer centers worldwide. All patients had 1-5 synchronous or metachronous metastases treated with surgical metastectomy, SBRT, or radical external beam radiation therapy and the primary tumor was treated aggressively with a curative intent. The 1-year Overall Survival (OS) was 70.2% and 5-year Overall Survival was 29.4%. The authors were able to develop a risk stratification model for survival, to help identify which patients would be the best candidates for SBRT or surgery. They noted that patients with metachronous metastases had a 5-year Overall Survival of 48% and were considered low risk, those with synchronous metastases and negative nodes had a 5-year OS of 36% and were considered intermediate risk and patients with synchronous metastases and positive nodes were considered high risk and had a 5-year overall survival of 14%.
Taken together, these two studies have demonstrated that SBRT improves Overall Survival in elderly frail patients with medically inoperable early stage Lung Cancer and SBRT also improves Overall survival in patients Stage IV Non Small Cell Lung Cancer, with metachronous metastases without nodal involvement. A multidisciplinary team approach is strongly recommended, as treatment decisions are made for the latter group.
1)Long-term Results of RTOG 0236: A Phase II Trial of Stereotactic Body Radiation Therapy (SBRT) in the Treatment of Patients with Medically Inoperable Stage I Non-Small Cell Lung Cancer. Timmerman RD, Hu C, Michalski J, et al. DOI:http://dx.doi.org/10.1016/j.ijrobp.2014.05.135
2)An Individual Patient Data Meta-Analysis of Outcomes and Prognostic Factors After Treatment of Oligometastatic Non-Small Cell Lung Cancer. Ashworth A, Senan S, Palma DA, et al. DOI: http://dx.doi.org/10.1016/j.ijrobp.2014.08.028
The FDA approves IRESSA® for metastatic Non Small Cell Lung Cancer
SUMMARY: The FDA on July 13, 2015 approved IRESSA® (Gefitinib) for the treatment of patients with metastatic Non Small Cell Lung Cancer (NSCLC), whose tumors have Epidermal Growth Factor Receptor (EGFR) exon 19 deletions or exon 21 (L858R) substitution mutations, as detected by an FDA approved test. IRESSA was approved concurrently with a labeling expansion of the therascreen EGFR RGQ PCR Kit, a companion diagnostic test, for patient selection. Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. It is the leading cause of cancer death among both men and women. The American Cancer Society estimates that over 221,200 new cases of lung cancer will be diagnosed in the United States in 2015 and over 158,000 patients will die of the disease. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large cell carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer. Epidermal Growth Factor Receptor (EGFR) is frequently overexpressed in NSCLC. In 2004, the discovery of Epidermal Growth Factor Receptor (EGFR) mutations in some advanced Non Small Cell Lung Cancer (NSCLC) patients, with Adenocarcinoma histology, and the favorable responses with EGFR Tyrosine Kinase Inhibitors (TKIs) such as TARCEVA® (Erlotinib), IRESSA® (Gefitinib) and GILOTRIF® (Afatinib), has changed the treatment paradigm, in favor of targeted therapy, for this patient subset. GILOTRIF® is an irreversible blocker of the ErbB family, which includes EGFR (ErbB1), HER2 (ErbB2), ErbB3 and ErbB4. It is estimated that approximately 10% of Western patient population and 50% of Asian patients with NSCLC, harbor EGFR activating mutations. IRESSA® is an oral, EGFR Tyrosine Kinase Inhibitor (TKI), which works by blocking the activity of the EGFR tyrosine kinase enzyme responsible for regulating signaling pathways, implicated in the growth and survival of cancer cells. IRESSA® was granted Orphan Drug Designation by the FDA in August 2014 for the treatment of EGFR mutation positive NSCLC.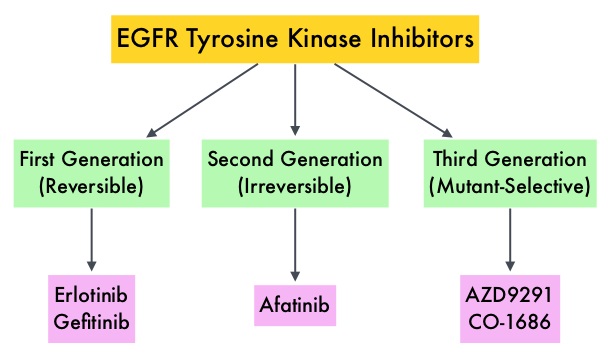
The approval of IRESSA® was based on the results of a Phase IV, single-arm, multicenter, open-label clinical study (IRESSA Follow-Up Measure or IFUM study) which included 106 treatment naïve-patients with metastatic EGFR mutation positive NSCLC who received IRESSA® 250mg PO daily. Treatment was given until disease progression or intolerable toxicity. Primary endpoint was Objective Response Rate (ORR). Secondary endpoints included Disease Control Rate (DCR), Progression Free Survival (PFS), Overall Survival (OS) and safety/tolerability. At the time of data cutoff, the investigator determined ORR was 70%, Duration of Response was 8.3 months, Disease Control Rate was 90.6%, median PFS was 9.7 months and median OS was19.2 months. This efficacy data was further supported by the IRESSA Pan-ASia Study (IPASS), a randomized phase III trial, which enrolled 1,217 treatment naïve advanced NSCLC patients with adenocarcinoma histology. Patients were randomized (1:1) to receive IRESSA® 250 mg PO daily or up to 6 cycles of combination chemotherapy with Carboplatin and Paclitaxel. The efficacy outcomes included Progression Free Survival (PFS) and Objective Response Rate (ORR). An exploratory analysis of a subset of 186 of 1217 patients (15%), who were determined to be EGFR mutation positive, had imaging studies available for evaluation (IRESSA® treated patients=88 and Carboplatin/Paclitaxel treated patients=98). The median PFS in the IRESSA® treated group was 10.9 months compared to 7.4 months for the Carboplatin/Paclitaxel treated patients (HR=0.54). The ORR was 67% with a Duration of Response (DoR) of 9.6 months for IRESSA® treated patients versus 41%, with a DoR of 5.5 months for Carboplatin/Paclitaxel treated patients. The most commonly reported adverse events for IRESSA® were diarrhea and skin toxicities including rash, acne, dry skin and pruritus. It was concluded that EGFR mutations are the strongest predictive biomarker for Progression Free Survival and tumor response to first line treatment with IRESSA®. First-line gefitinib in Caucasian EGFR mutation-positive NSCLC patients: a phase-IV, open-label, single-arm study. Douillard J-Y, Ostoros G, Cobo M, et al. Br J Cancer. 2014;110:55–62
GILOTRIF® Superior to TARCEVA® in Squamous Cell Carcinoma of the Lung
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. It is the leading cause of cancer death among both men and women. The American Cancer Society estimates that over 221,200 new cases of lung cancer will be diagnosed in the United States in 2015 and over 158,000 patients will die of the disease. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large cell carcinomas.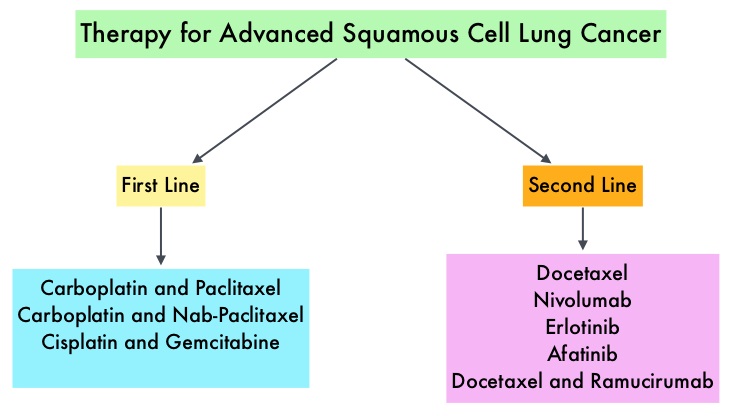 Non Small Cell Lung Cancer patients with squamous cell histology have been a traditionally hard- to-treat patient group, with less than 5% of patients with advanced SCC, surviving for five years or longer. Some of the advanced NSCLC tumors are dependent on the Epidermal Growth Factor Receptor (EGFR) for cell proliferation and survival, regardless of EGFR mutation status. TARCEVA® (Erlotinib) is a reversible EGFR Tyrosine Kinase Inhibitor and is presently approved by the FDA for the treatment of locally advanced or metastatic NSCLC, after failure of at least one prior chemotherapy regimen. GILOTRIF® (Afatinib) is an oral, irreversible blocker of the ErbB family which includes EGFR (ErbB1), HER2 (ErbB2), ErbB3 and ErbB4. This kinase inhibitor is indicated for the first line treatment of patients with metastatic NSCLC, whose tumors have Epidermal Growth Factor Receptor (EGFR) exon 19 deletions or exon 21 (L858R) substitution mutations.
Non Small Cell Lung Cancer patients with squamous cell histology have been a traditionally hard- to-treat patient group, with less than 5% of patients with advanced SCC, surviving for five years or longer. Some of the advanced NSCLC tumors are dependent on the Epidermal Growth Factor Receptor (EGFR) for cell proliferation and survival, regardless of EGFR mutation status. TARCEVA® (Erlotinib) is a reversible EGFR Tyrosine Kinase Inhibitor and is presently approved by the FDA for the treatment of locally advanced or metastatic NSCLC, after failure of at least one prior chemotherapy regimen. GILOTRIF® (Afatinib) is an oral, irreversible blocker of the ErbB family which includes EGFR (ErbB1), HER2 (ErbB2), ErbB3 and ErbB4. This kinase inhibitor is indicated for the first line treatment of patients with metastatic NSCLC, whose tumors have Epidermal Growth Factor Receptor (EGFR) exon 19 deletions or exon 21 (L858R) substitution mutations.
The LUX-Lung 8 is a phase III trial in which 795 patients with Stage IIIB/IV Squamous Cell Carcinoma of the lung who had progressed on first line platinum based doublet therapy, were randomized 1:1 to receive GILOTRIF 40 mg PO daily (N=398) or TARCEVA 150 mg PO daily (N=397). Treatment was given until disease progression. The median age was 65 years. Majority of the patients were male, caucasian and ex-smokers. The Primary endpoint was Progression Free Survival (PFS) and Secondary endpoints included Overall Survival (OS), Objective Response Rate (ORR), Disease Control Rate (DCR), patient reported outcomes and safety. The Primary endpoint of Progression Free Survival (PFS) was met and reported in 2014 and favored GILOTRIF® over TARCEVA®. The authors in this analysis reported the Overall Survival data, as well as updated data on Progression Free Survival and other Secondary endpoints. The median Overall Survival was 7.9 months with GILOTRIF® and 6.8 months with TARCEVA® (HR=0.81; P=0.008). This meant a 19% reduction in the risk of death with GILOTRIF® when compared to TARCEVA® and this survival advantage was consistent across all time points. The updated median Progression Free Survival for GILOTRIF® was 2.6 months vs 1.9 months for TARCEVA® (HR=0.81; P=0.01). The Disease Control Rate was 50.5% for GILOTRIF® and 39.5% with TARCEVA® (P=0.002). Based on patient reported outcomes, symptoms including cough and dyspnea were better with GILOTRIF® compared to TARCEVA®. Incidence of severe adverse events was similar with both therapies, with patients on GILOTRIF® experiencing more grade 3 diarrhea and stomatitis and patients receiving TARCEVA® experiencing more grade 3 rash. The authors concluded that GILOTRIF® should be the TKI of choice in the second line treatment of patients with Squamous Cell Carcinoma of the lung, as it significantly improves Overall Survival, Progression Free Survival, Disease Control Rate and symptom control, with manageable toxicities, when compared to TARCEVA®. Afatinib (A) vs erlotinib (E) as second-line therapy of patients (pts) with advanced squamous cell carcinoma (SCC) of the lung following platinum-based chemotherapy: Overall survival (OS) analysis from the global phase III trial LUX-Lung 8 (LL8). Soria J, Felip E, Cobo M, et al. J Clin Oncol 33, 2015 (suppl; abstr 8002)
IRESSA® (Gefitinib)
The FDA on July 13, 2015 approved IRESSA® for the treatment of patients with metastatic Non Small Cell Lung Cancer (NSCLC), whose tumors have Epidermal Growth Factor Receptor (EGFR) exon 19 deletions or exon 21 (L858R) substitution mutations, as detected by an FDA approved test. IRESSA® was approved concurrently with a labeling expansion of the therascreen EGFR RGQ PCR Kit, a companion diagnostic test, for patient selection. IRESSA® tablets are a product of AstraZeneca Pharmaceuticals LP.
Late Breaking Abstract – ASCO 2015 OPDIVO® Improves Overall Survival in Non- Squamous NSCLC Patients
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. It is the leading cause of cancer death among both men and women. The American Cancer Society estimates that over 221,200 new cases of lung cancer will be diagnosed in the United States in 2015 and over 158,000 patients will die of the disease. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 25% are Squamous cell carcinomas, 40% are Adenocarcinomas and 10% are Large cell carcinomas. The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of the Immune checkpoints. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. 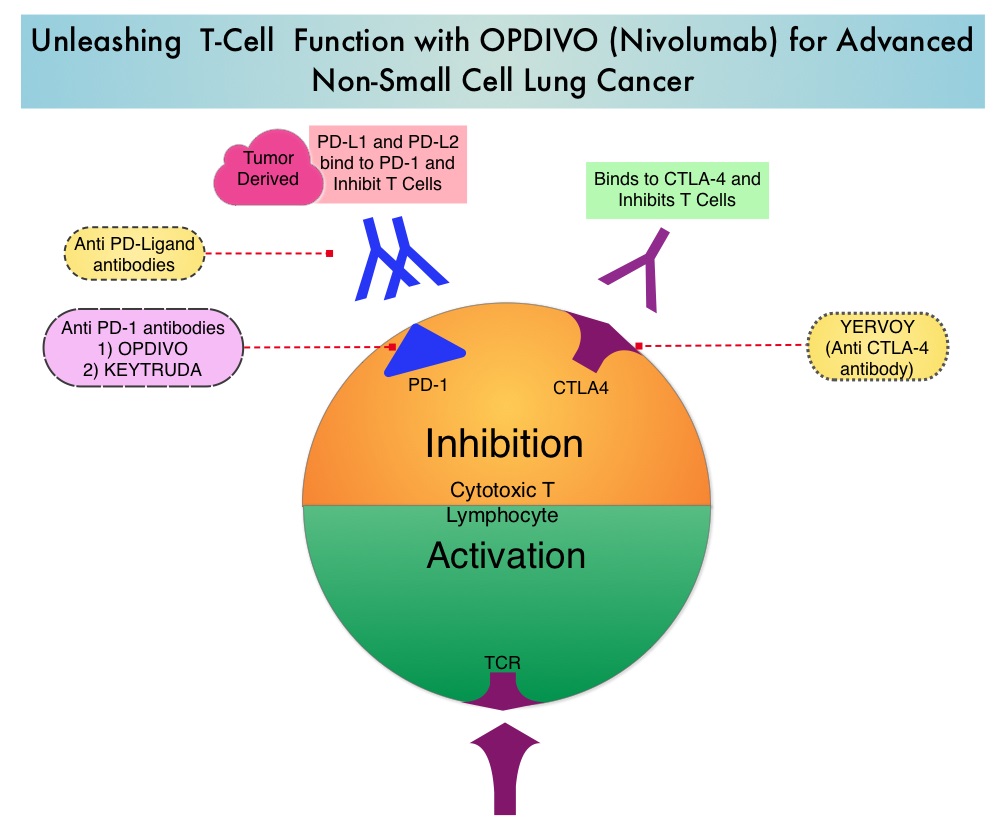 Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first Immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab) , an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. OPDIVO® (Nivolumab) is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the T cells. The U. S. Food and Drug Administration granted approval to OPDIVO®, for the treatment of patients with metastatic Squamous Non-Small Cell Lung Cancer (NSCLC), with progression on or after platinum based chemotherapy. CheckMate 057 is a randomized, international, phase 3 study designed to evaluate the benefit of OPDIVO® for patients with Non-Squamous (NSQ) NSCLC who had progressed after platinum-based doublet chemotherapy. A total of 582 patients were randomized to receive OPDIVO® 3 mg/kg IV every 2 weeks (n=292) or TAXOTERE® 75 mg/m2 IV every 3 weeks (n=290). Eligible patients included those with advanced Non-Squamous NSCLC who had progressed after platinum-based doublet chemotherapy and a Tyrosine Kinase Inhibitor (TKI), if deemed eligible for a TKI. Treatment was continued until disease progression or unacceptable toxicity. The primary clinical endpoint was Overall Survival (OS). Secondary endpoints included Objective Response Rate (ORR), Progression Free Survival (PFS), Efficacy based on PD-L1 expression, Quality of Life, and Safety. The study was stopped earlier than expected following assessment by the independent Data Monitoring Committee (DMC) which concluded that the study met its endpoint, demonstrating superior overall survival, in patients receiving OPDIVO®, compared to the control group. Patients in the OPDIVO®, group had a significantly higher median OS compared to those in the TAXOTERE® group (12.2 months versus 9.4 months, Hazard Ratio [HR] 0.73, P=0.0015). This meant a 27% reduction in the risk of death in the OPDIVO® group and this survival benefit was seen in all predefined subgroup of patients. The Objective Response Rate (ORR) was also significantly higher for patients receiving OPDIVO® compared to TAXOTERE® (19% versus 12%, P=0.0246) and the median duration of response (DOR) was significantly higher for the OPDIVO® group (17.2 months) vs the TAXOTERE® group (5.6 months). More importantly, when tumor PD-L1 expression was correlated with Overall Survival, the median OS for OPDIVO® was 17.2 months, 18.2 months, and 19.4 months for patients with tumors having 1% or higher, 5% or higher, and 10% or higher of cells staining positive for PD-L1, respectively, compared with 9.0 months, 8.1 months, and 8.0 months with TAXOTERE® treatment. Even though this study showed significant survival outcomes for patients expressing any level of PD-L1, the magnitude of benefit was even more so, in patients with tumors expressing higher levels of PD-L1. PD-L1 expression may therefore be a predictor of response, although this should not yet be used for patient selection. Grade 3-5 adverse events occurred more often in the TAXOTERE® group compared to the OPDIVO® group (54% vs 10%). Based on this compelling data, the authors concluded that OPDIVO® significantly improves Overall Survival when compared to TAXOTERE®, in patients with advanced non-Squamous NSCLC, after failure of platinum based doublet therapy. Phase III, randomized trial (CheckMate 057) of nivolumab (NIVO) versus docetaxel (DOC) in advanced non-squamous cell (non-SQ) non-small cell lung cancer (NSCLC). Paz-Ares L, Horn L, Borghaei H, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA109)</s
Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first Immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab) , an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. OPDIVO® (Nivolumab) is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the T cells. The U. S. Food and Drug Administration granted approval to OPDIVO®, for the treatment of patients with metastatic Squamous Non-Small Cell Lung Cancer (NSCLC), with progression on or after platinum based chemotherapy. CheckMate 057 is a randomized, international, phase 3 study designed to evaluate the benefit of OPDIVO® for patients with Non-Squamous (NSQ) NSCLC who had progressed after platinum-based doublet chemotherapy. A total of 582 patients were randomized to receive OPDIVO® 3 mg/kg IV every 2 weeks (n=292) or TAXOTERE® 75 mg/m2 IV every 3 weeks (n=290). Eligible patients included those with advanced Non-Squamous NSCLC who had progressed after platinum-based doublet chemotherapy and a Tyrosine Kinase Inhibitor (TKI), if deemed eligible for a TKI. Treatment was continued until disease progression or unacceptable toxicity. The primary clinical endpoint was Overall Survival (OS). Secondary endpoints included Objective Response Rate (ORR), Progression Free Survival (PFS), Efficacy based on PD-L1 expression, Quality of Life, and Safety. The study was stopped earlier than expected following assessment by the independent Data Monitoring Committee (DMC) which concluded that the study met its endpoint, demonstrating superior overall survival, in patients receiving OPDIVO®, compared to the control group. Patients in the OPDIVO®, group had a significantly higher median OS compared to those in the TAXOTERE® group (12.2 months versus 9.4 months, Hazard Ratio [HR] 0.73, P=0.0015). This meant a 27% reduction in the risk of death in the OPDIVO® group and this survival benefit was seen in all predefined subgroup of patients. The Objective Response Rate (ORR) was also significantly higher for patients receiving OPDIVO® compared to TAXOTERE® (19% versus 12%, P=0.0246) and the median duration of response (DOR) was significantly higher for the OPDIVO® group (17.2 months) vs the TAXOTERE® group (5.6 months). More importantly, when tumor PD-L1 expression was correlated with Overall Survival, the median OS for OPDIVO® was 17.2 months, 18.2 months, and 19.4 months for patients with tumors having 1% or higher, 5% or higher, and 10% or higher of cells staining positive for PD-L1, respectively, compared with 9.0 months, 8.1 months, and 8.0 months with TAXOTERE® treatment. Even though this study showed significant survival outcomes for patients expressing any level of PD-L1, the magnitude of benefit was even more so, in patients with tumors expressing higher levels of PD-L1. PD-L1 expression may therefore be a predictor of response, although this should not yet be used for patient selection. Grade 3-5 adverse events occurred more often in the TAXOTERE® group compared to the OPDIVO® group (54% vs 10%). Based on this compelling data, the authors concluded that OPDIVO® significantly improves Overall Survival when compared to TAXOTERE®, in patients with advanced non-Squamous NSCLC, after failure of platinum based doublet therapy. Phase III, randomized trial (CheckMate 057) of nivolumab (NIVO) versus docetaxel (DOC) in advanced non-squamous cell (non-SQ) non-small cell lung cancer (NSCLC). Paz-Ares L, Horn L, Borghaei H, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA109)</s
Targeting ROS1 Molecular Driver Mutations with XALKORI® in NSCLC
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. It is the leading cause of cancer death among both men and women. The American Cancer Society estimates that over 221,200 new cases of lung cancer will be diagnosed in the United States in 2015 and over 158,000 patients will die of the disease. Non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 25% are Squamous cell carcinomas, 40% are Adenocarcinomas and 10% are Large cell carcinomas. There is now growing body of evidence suggesting superior outcomes when advanced NSCLC patients with specific genomic alterations receive targeted therapies.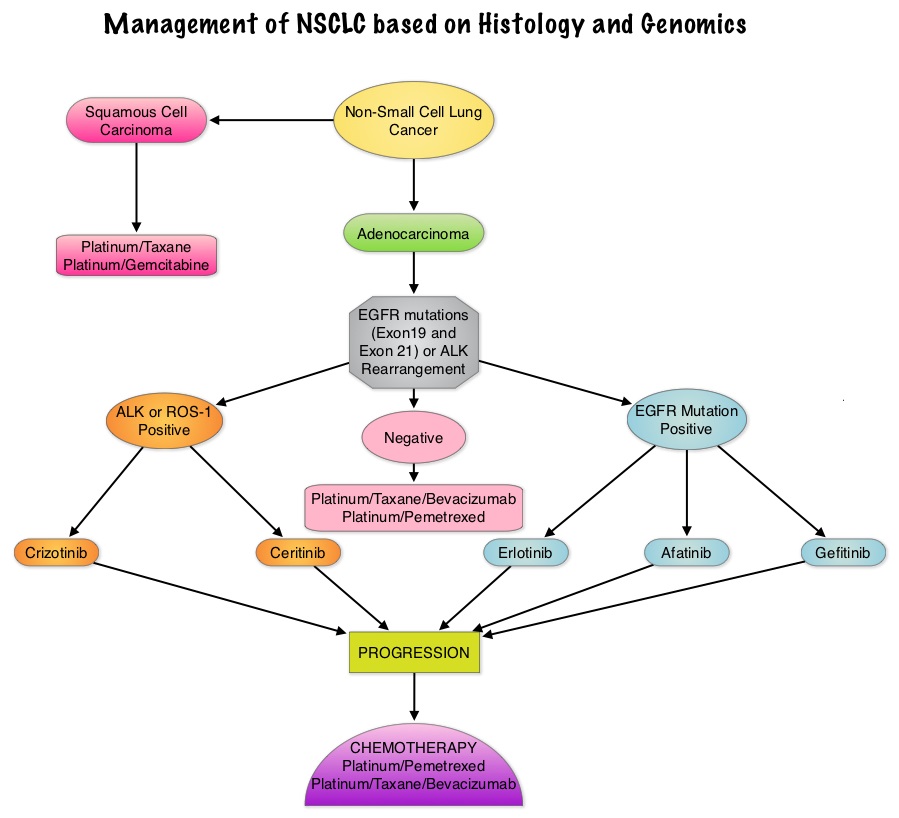 Approximately 1% – 2% of lung adenocarcinomas harbor ROS1 gene rearrangements. ROS1 gene is located on chromosome 6q22 (long arm of chromosome 6) and plays an important role in cell growth and development. ROS1 gene fusion with another gene results in a mutated DNA sequence which then produces an abnormal protein responsible for unregulated cell growth and cancer. ROS1 gene rearrangement has been identified as a driver mutation in Non Small cell Lung Cancer with adenocarcinoma histology. This is more common in nonsmokers or in light smokers (<10 pack years) who are relatively young (average age of 50 years) and thus share similar characteristics with ALK-positive patients. The ROS protein and the ALK protein have similar structure and function and are sensitive to Tyrosine Kinase Inhibitors such as XALKORI® (Crizotinib) and ZYKADIA® (Ceritinib). ROS1 mutations have been also been associated with Cholangiocarcinoma (Bile duct cancer) and Glioblastoma multiforme. ROS1 rearrangements are mutually exclusive with other oncogenic mutations found in NSCLC such as EGFR mutations, KRAS mutations and ALK rearrangement. The presence of a ROS1 rearrangement can be detected by Fluorescence In Situ Hybridization (FISH), ImmunoHistoChemistry (IHC), Reverse Transcriptase– Polymerase Chain Reaction (RT-PCR) and Next Generation-Sequencing. XALKORI® is a small molecule Tyrosine Kinase Inhibitor that targets ALK, MET and ROS1 tyrosine kinases. In a previously published expansion cohort of the phase 1 study by Shaw and colleagues ( NEJM 2014; 371:1963-1971), XALKORI® showed significant activity in patients with in patients with advanced ROS1rearranged NSCLC. The authors in this publication provided additional evidence that ROS1 gene rearrangement is an actionable target in NSCLC, by conducting a retrospective study in centers that tested for ROS1 rearrangement and evaluated the outcomes of ROS1-positive NSCLC patients, who had been treated with XALKORI®. They included 32 patients with NSCLC whose tumors showed ROS1 rearrangement and who had received off-label treatment with XALKORI®. The median age was 50.5 years. They noted an overall response rate of 80% and a disease control rate, 86.7%. The median Progression Free Survival (PFS) was 9.1 months, and the PFS rate at 12 months was 44%. This impressive efficacy data again validates that similar to EGFR mutations and ALK rearrangements, ROS1 gene rearrangements are molecular drivers and patients with NSCLC with adenocarcinoma histology should be tested for ROS1. Crizotinib Therapy for Advanced Lung Adenocarcinoma and a ROS1 Rearrangement: Results From the EUROS1 Cohort. Mazières J, Zalcman G, Crinò L, J Clin Oncol. 2015;33:992-999
Approximately 1% – 2% of lung adenocarcinomas harbor ROS1 gene rearrangements. ROS1 gene is located on chromosome 6q22 (long arm of chromosome 6) and plays an important role in cell growth and development. ROS1 gene fusion with another gene results in a mutated DNA sequence which then produces an abnormal protein responsible for unregulated cell growth and cancer. ROS1 gene rearrangement has been identified as a driver mutation in Non Small cell Lung Cancer with adenocarcinoma histology. This is more common in nonsmokers or in light smokers (<10 pack years) who are relatively young (average age of 50 years) and thus share similar characteristics with ALK-positive patients. The ROS protein and the ALK protein have similar structure and function and are sensitive to Tyrosine Kinase Inhibitors such as XALKORI® (Crizotinib) and ZYKADIA® (Ceritinib). ROS1 mutations have been also been associated with Cholangiocarcinoma (Bile duct cancer) and Glioblastoma multiforme. ROS1 rearrangements are mutually exclusive with other oncogenic mutations found in NSCLC such as EGFR mutations, KRAS mutations and ALK rearrangement. The presence of a ROS1 rearrangement can be detected by Fluorescence In Situ Hybridization (FISH), ImmunoHistoChemistry (IHC), Reverse Transcriptase– Polymerase Chain Reaction (RT-PCR) and Next Generation-Sequencing. XALKORI® is a small molecule Tyrosine Kinase Inhibitor that targets ALK, MET and ROS1 tyrosine kinases. In a previously published expansion cohort of the phase 1 study by Shaw and colleagues ( NEJM 2014; 371:1963-1971), XALKORI® showed significant activity in patients with in patients with advanced ROS1rearranged NSCLC. The authors in this publication provided additional evidence that ROS1 gene rearrangement is an actionable target in NSCLC, by conducting a retrospective study in centers that tested for ROS1 rearrangement and evaluated the outcomes of ROS1-positive NSCLC patients, who had been treated with XALKORI®. They included 32 patients with NSCLC whose tumors showed ROS1 rearrangement and who had received off-label treatment with XALKORI®. The median age was 50.5 years. They noted an overall response rate of 80% and a disease control rate, 86.7%. The median Progression Free Survival (PFS) was 9.1 months, and the PFS rate at 12 months was 44%. This impressive efficacy data again validates that similar to EGFR mutations and ALK rearrangements, ROS1 gene rearrangements are molecular drivers and patients with NSCLC with adenocarcinoma histology should be tested for ROS1. Crizotinib Therapy for Advanced Lung Adenocarcinoma and a ROS1 Rearrangement: Results From the EUROS1 Cohort. Mazières J, Zalcman G, Crinò L, J Clin Oncol. 2015;33:992-999