
The FDA on September 14, 2017 approved MVASI® as a biosimilar to AVASTIN® (Bevacizumab). MVASI® is the first biosimilar approved in the U.S. for the treatment of cancer, and is a product of Amgen Inc.
Author: RR
KYMRIAH® (Tisagenlecleucel)
The FDA on August 30, 2017 granted regular approval to KYMRIAH®, for the treatment of patients up to age 25 years with B-cell precursor Acute Lymphoblastic Leukemia (ALL), that is refractory or in second or later relapse. KYMRIAH® is a product of Novartis Pharmaceuticals Corp.
FDA Approves First Biosimilar for Cancer Treatment
The FDA on Sept. 14, 2017 approved MYASI® (Bevacizumab-awwb) as a Biosimilar to AVASTIN® (Bevacizumab). MYASI® is the first Biosimilar approved in the U.S. for the treatment of cancer. A Biosimilar must show that it has no clinically meaningful differences in terms of safety and effectiveness from the already approved biological product (also known as reference product). A Biosimilar product can only be approved by the FDA if it has the same mechanism of action, route of administration, dosage form and strength as the reference product, and only for the indications and conditions of use, that have been approved for the reference product. The approval of MYASI® was based on comparisons of extensive structural and functional product characterization, animal data, human PharmacoKinetic and pharmacodynamic data, clinical immunogenicity, between MYASI® and AVASTIN® (Bevacizumab), and it was noted that MYASI® is highly similar to AVASTIN® and that there are no clinically meaningful differences between the two products.
Guideline for HER2 Testing in Gastroesophageal Adenocarcinoma
SUMMARY: It is estimated that in 2016 GastroEsophageal Adenocarcinoma (GEA) accounted for 43,280 new cases in the United States. Majority of the patients with GEA have advanced disease at the time of initial presentation and have limited therapeutic options with little or no chance for cure. Patients with localized disease (stage II and stage III) are often treated with multimodality therapy and 40% of the patients may survive for 5 years or more. Approximately 7-38% of GEAs have amplification and/or overexpression of HER2. HER2 (ERBB2) is a proto-oncogene located on the long arm of chromosome 17 (17q12) that encodes a tyrosine kinase receptor, which upon dimerization and phosphorylation, initiates signaling pathways, that lead to cell division, proliferation, differentiation and anti-apoptosis signaling.
GastroEsophageal junction tumors have a higher incidence of overexpression of HER2 compared to gastric cancers. In the stomach, overexpression of HER2 varies with histologic type (intestinal-type having greater expression than diffuse-type) and differentiation (well and moderately differentiated tumors having greater expression than poorly differentiated tumors). Further, the heterogeneity of immunostaining is greater in GEA and the complete membrane staining required for positivity in breast cancer, is not common in GEA. Due to the high heterogeneity of a gastric cancer, it is appropriate to evaluate HER2 expression on biopsy specimens, especially in unresectable cases and reevaluate it on resected specimens, when available.
The NCCN (National Comprehensive Cancer Network) Clinical Practice Guidelines in Oncology for Gastric Cancer and Esophageal and Esophagogastric Junction Cancers, recommend assessment of HER2 overexpression using ImmunoHistoChemistry and/or gene amplification using FISH (Fluorescence In Situ Hybridization or another in situ hybridization method, in tumor samples from patients, with unresectable, locally advanced, recurrent, or metastatic GEA, for whom HERCEPTIN® may be potentially beneficial. Testing for HER2 is primarily performed on Formalin-Fixed and Paraffin-Embedded biopsy or resection tumor tissue from the primary or metastatic site. There are important differences in HER2 expression, scoring, and outcomes in GEA compared to breast carcinoma, and the need for HER2 guidelines (that include critical clinical and laboratory considerations) was therefore recognized. The CAP, American Society for Clinical Pathology, and ASCO convened an international expert panel to systematically review published documents and to develop an evidence-based guideline, to establish recommendations for HER2 testing in GastroEsophageal Adenocarcinoma.
HERCEPTIN® (Trastuzumab) is humanized monoclonal antibody that targets HER2. HERCEPTIN® is effective only in cancers where HER2 is overexpressed. In a previously published randomized phase III trial, HERCEPTIN® in combination with chemotherapy was shown to significantly improve Overall Survival compared with chemotherapy alone, in patients with HER2 positive advanced GEA.
The following are the Guideline Summary from the College of American Pathologists, American Society for Clinical Pathology, and American Society of Clinical Oncology
Guideline Questions
• What is the optimal testing algorithm for the assessment of Human Epithelial Growth Factor 2 (HER2) status in patients with GastroEsophageal Adenocarcinoma (GEA)?
• What strategies can help ensure optimal performance, interpretation, and reporting of established assays in patients with GEA?
Target Population: Patients with GEA.
Target Audience: Medical and surgical oncologists; oncology nurses and physician assistants; pathologists; general practitioners; and patients.
Key Points and Recommendations for Clinicians
Recommendation 1.1
For patients with advanced GEA who are potential candidates for HER2-targeted therapy, the treating clinician should request HER2 testing on tumor tissue.
Recommendation 1.2
Treating clinicians or pathologists should request HER2 testing on tumor tissue in the biopsy or resection specimens (primary or metastasis) preferably before the initiation of HERCEPTIN® therapy if such specimens are available and adequate. HER2 testing on fine-needle aspiration specimens (cell blocks) is an acceptable alternative.
Recommendation 1.3
Treating clinicians should offer combination chemotherapy and HER2-targeted therapy as the initial treatment of appropriate patients with HER2-positive tumors who have advanced GEA
Key Points and Recommendations for Pathologists
Recommendation 2.1
Laboratories/pathologists must specify the antibodies and probes used for the test and ensure that assays are appropriately validated for HER2 ImmunoHistoChemistry (IHC) and in situ hybridization (ISH) on GEA specimens.
Recommendation 2.2
When GEA HER2 status is being evaluated, laboratories/pathologists should perform/order IHC testing first, followed by ISH (In Situ Hybridization) when the IHC result is 2+ (equivocal). Positive (3+) or negative (0 or 1+) HER2 IHC results do not require further ISH testing.
Recommendation 2.3
Pathologists should use the Ruschoff/Hofmann method in scoring HER2 IHC and ISH results for GEA.
Recommendation 2.4
Pathologists should select the tissue block with the areas of lowest grade tumor morphology in biopsy and resection specimens. More than one tissue block may be selected if different morphologic patterns are present.
Recommendation 2.5
Laboratories should report HER2 test results in GEA specimens in accordance with the College of American Pathologists biomarker Template for Reporting Results of HER2 (ERBB2) Biomarker Testing of Specimens From Patients With Adenocarcinoma of the Stomach or Esophagogastric Junction.
Recommendation 2.6
Pathologists should identify areas of invasive adenocarcinoma and also mark areas with strongest intensity of HER2 expression by IHC in GEA specimens for subsequent ISH scoring when required.
Recommendation 2.7
Laboratories must incorporate GEA HER2 testing methods into their overall laboratory quality improvement program, establishing appropriate quality improvement monitors as needed to ensure consistent performance in all steps of the testing and reporting process. In particular, laboratories performing GEA HER2 testing should participate in a formal proficiency testing program, if available, or an alternative proficiency assurance activity.
Recommendation 2.8
There is insufficient evidence to recommend for or against genomic testing in patients with GEA at this time.
HER2 Testing and Clinical Decision Making in Gastroesophageal Adenocarcinoma: Guideline Summary From the College of American Pathologists, American Society for Clinical Pathology, and American Society of Clinical Oncology. Bartley AN, Washington MK, Ismaila N, et al. Journal of Oncology Practice 2017;13:53-57.
Maintenance Therapy with REVLIMID® Prolongs PFS in High Risk CLL
SUMMARY: The American Cancer Society estimates that approximately 20,110 new cases of Chronic Lymphocytic Leukemia (CLL) will be diagnosed in 2017 and approximately 4660 patients will die from the disease. CLL is a heterogeneous disease with a clinical course that is variable, with a very indolent course in some patients and some with aggressive disease and others somewhere in between. Both Binet and the Rai CLL staging systems developed in the 1970’s rely solely on physical examination and standard laboratory testing to predict survival. With the development of Interphase Fluorescent In Situ Hybridization (FISH) technique, which allows detection of genetic abnormalities in noncycling CLL cells, it has become clear that cytogenetic abnormalities are often seen in CLL patients and these genetic abnormalities in turn appear to be reliable predictors of disease progression, response to therapy and survival. Some of these cytogenetic abnormalities include del(13q), normal karyotype, trisomy(12), del(11q), del(17p), and they are associated with decreasing survival times, in that order. Another important prognostic factor is the rearrangement and somatic hypermutation of the variable region of the immunoglobulin heavy chain genes (IGHV), which is an independent predictor of outcome in CLL. Retrospective studies have suggested that patients with CLL whose leukemic cells unmutated IGHV gene demonstrated more aggressive disease and shorter survival time compared to those patients with somatic hypermutations in their IGHV genes (Mutated IGHV gene). Expression of two flow cytometry based biomarkers, CD38 (surface marker) and ZAP-70 (intracytoplasmic protein), have been associated with poor outcomes as well.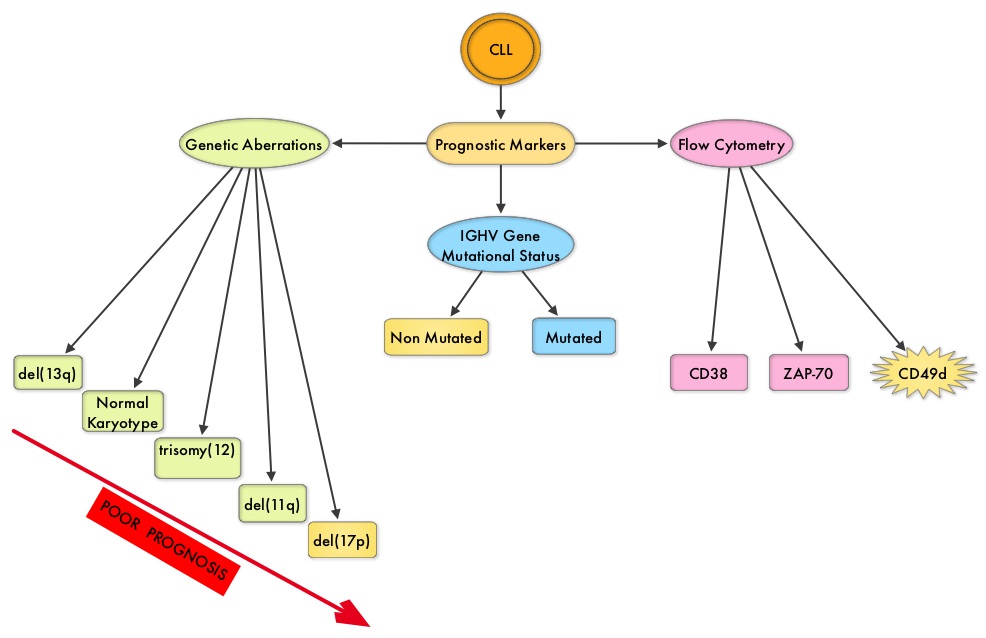
The rationale for maintenance treatment in the CLL patients is based on previously published studies showing that about 30% of patients with CLL did not substantially benefit from chemoimmunotherapy alone. These patients belong to the high risk group, as defined by poor cytogenetics, positive Minimal Residual Disease at the end of chemoimmunotherapy and unmutated IGHV gene status. The combined use of Genetic markers and Minimal Residual Disease (MRD) assessment can therefore identify patients with CLL, who have a poor outcome with first line chemoimmunotherapy.
Maintenance therapy with REVLIMID® (Lenalidomide)/Dexamethasone is considered standard of care for patients with multiple myeloma, regardless of transplantation and for newly diagnosed non-transplant candidates, as this intervention was found to improve Progression Free Survival significantly, with a favorable safety profile. Two phase III studies demonstrating the benefit of maintenance treatment with REVLIMID® in patients with CLL, were presented at the 2016 American Society of Hematology (ASH) Annual Meeting & Exposition. The first study (CLL M1 study) was conducted to demonstrate the value of maintenance treatment with REVLIMID® in patients with high risk CLL, following first line chemoimmunotherapy. For this study, 468 patients were screened, of whom 89 patients (N=89) were considered as high risk for disease progression, following 4 cycles of chemoimmunotherapy. This was based on the following factors: MRD levels of 10-2 or higher or MRD levels of 10-4 or higher to less than 10-2, combined with either an unmutated IGHV gene status, del(17p) or TP53 mutation at baseline.
Patients received investigator’s choice of chemoimmunotherapy regimens which included Fludarabine/Cyclophosphamide/Rituximab (FCR), Fludarabine and Rituximab (FR), Fludarabine and Cyclophosphamide (FC), or Bendamustine and Rituximab (BR). The most common regimens administered were Bendamustine and Rituximab followed by FCR. Approximately 78% of all patients reached Minimal Residual Disease negativity and these patients were ineligible for this trial. The 89 eligible patients were randomized in a 2:1 ratio to receive REVLIMID® maintenance (N=60) or Placebo (N=29). Treatment with REVLIMID® or Placebo was started at 5 mg daily for the first cycle, and was subsequently increased to the target dose of 15 mg by the 7th cycle. The median age of these patients was 64 years. At randomization, 37% of patients had a high and 63% had an intermediate MRD level, respectively. Based on their risk for thromboembolic events, patients received either low dose aspirin daily or appropriate prophylactic anticoagulants. The primary endpoint was Progression Free Survival (PFS).
After a median follow up of 17.7 months, the median PFS for REVLIMID® group has not been reached and was 13.3 months for the Placebo group. This meant a relative risk reduction for disease progression of 80% and this was highly statistically significant (P < 0.00001). There was no difference in Overall Survival at the time of this interim analysis. Adverse events such as neutropenia, diarrhea, skin disorders, etc. were more frequently noted with REVLIMID® maintenance treatment.
The authors concluded that REVLIMID® maintenance treatment for high risk CLL patients, after first line chemoimmunotherapy, significantly prolonged Progression Free Survival and this study confirmed the prognostic significance of the MRD based risk assessment.
The second study, CONTINUUM Trial, is a multicenter, randomized, double-blinded phase III study, designed to evaluate the efficacy and safety of REVLIMID® as maintenance therapy in previously treated CLL patients. In this study, 314 CLL patients who at least had a partial response (PR) to second line therapy were randomized 1:1 to receive either REVLIMID® 2.5 mg once daily on days 1-28 of the first 28 day cycle, or matching Placebo. If tolerated, REVLIMID® dose was then increased to 5 mg daily from cycle 2, and further increased to 10 mg daily at cycle 7 and thereafter. Co-primary endpoints were Progression Free Survival (PFS) and Overall Survival and secondary endpoints included Safety, Tumor response, Duration of Response and Health related Quality of Life measures.
At a median follow up of 31.5 months, the median PFS was significantly longer for the REVLIMID® group compared to the Placebo group (33.9 vs 9.2 months; HR=0.40; P<0.001). This benefit with REVLIMID® maintenance was maintained in all patient subgroups regardless of age, prior response to chemotherapy and number of poor prognostic factors.
The authors in this trial concluded that REVLIMID® maintenance resulted in a 60% reduction in the risk of disease progression in patients with CLL following second line treatment, and there was no meaningful difference in the Quality of Life between the two treatment groups.
Taken together, these two phase III studies suggest that REVLIMID® maintenance therapy following either first line or second line chemoimmunotherapy, significantly prolongs Progression Free Survival in patients with CLL. This strategy will however not be applicable to patients receiving upfront chemotherapy-free regimens such as BTK Inhibitor, IMBRUVICA® (Ibrutinib).
1. Lenalidomide maintenance after front line therapy substantially prolongs progression free survival in high risk CLL. Fink AM, Bahlo J, Sandra R, et al. 2016 ASH Annual Meeting. Abstract 229. Presented December 3, 2016.
2. Results of the phase 3 study of lenalidomide versus placebo as maintenance therapy following second-line treatment for patients with chronic lymphocytic leukemia. Foà R, Schuh A, Zaritskey A, et al. 2016 ASH Annual Meeting. Abstract 230. Presented December 3, 2016.
Screening Mammography Starting at Age 40 years May Reduce Breast Cancer Deaths by 40 percent
In the US, about 33 million screening mammograms are performed each year. Currently, the major national health care organizations in the US have different recommendations for screening mammography which has led to some confusion and emotional counterarguments. These several different recommendations include 1) Annual screening at ages 40 to 84 years. 2) Annual screening at ages 45 to 54 years and then biennially at ages 55 to 79 years. 3) Biennial screening at ages 50 to 74 years.
In a recently published study (CANCER, August 21, 2017), it was noted that the greatest breast cancer-specific mortality reduction was achieved with annual screening of women starting at age 40 years, saving 29,369 lives from breast cancer. This is the first study to compare the three most widely discussed recommendations for screening mammography, head to head.
First CAR T-Cell Immunotherapy Approved by the FDA for Acute Lymphoblastic Leukemia
The FDA on August 30, 2017, granted regular approval to KYMRIAH® (Tisagenlecleucel) for the treatment of patients up to age 25 years with B-cell precursor Acute Lymphoblastic Leukemia (ALL), that is refractory or in second or later relapse. KYMRIAH® is the first Chimeric Antigen Receptor (CAR) T-cell immunotherapy approved by the FDA. A single infusion of KYMRIAH® was highly efficacious, in patients with relapsed and refractory ALL, and was associated with a high and durable Remission Rate. This technology may be applied to other malignancies, as new antigen targets are identified.
First CAR T-Cell Immunotherapy Approved by the FDA for Acute Lymphoblastic Leukemia
SUMMARY: The FDA on August 30, 2017, granted regular approval to KYMRIAH® (Tisagenlecleucel) for the treatment of patients up to age 25 years with B-cell precursor Acute Lymphoblastic Leukemia (ALL), that is refractory or in second or later relapse. KYMRIAH® is the first Chimeric Antigen Receptor (CAR) T-cell immunotherapy approved by the FDA.
What is (CAR) T-cell immunotherapy? Chimeric Antigen Receptor (CAR) T-cell therapy is a type of immunotherapy and consists of T cells collected from the patient’s blood in a leukapheresis procedure, and genetically engineered to produce special receptors on their surface called Chimeric Antigen Receptors (CAR). These reprogrammed cytotoxic T cells with the Chimeric Antigen Receptors on their surface are now able to recognize a specific antigen on tumor cells. These genetically engineered and reprogrammed CAR T-cells are grown in the lab and are then infused into the patient. These cells in turn proliferate in the patient’s body and the engineered receptor on the cell surface help recognize and kill cancer cells that expresses that specific antigen. KYMRIAH® (genetically engineered T-cells) seeks out cancer cells expressing the antigen CD19, which is found uniquely on B cells and destroy them. Patients, following treatment with CAR T-cells, develop B-cell aplasia (absence of CD19 positive cells) due to B-cell destruction and may need immunoglobin replacement. Hence, B-cell aplasia can be a useful therapeutic marker, as continued B-cell aplasia has been seen in all patients who had sustained remission, following CAR T-cell therapy.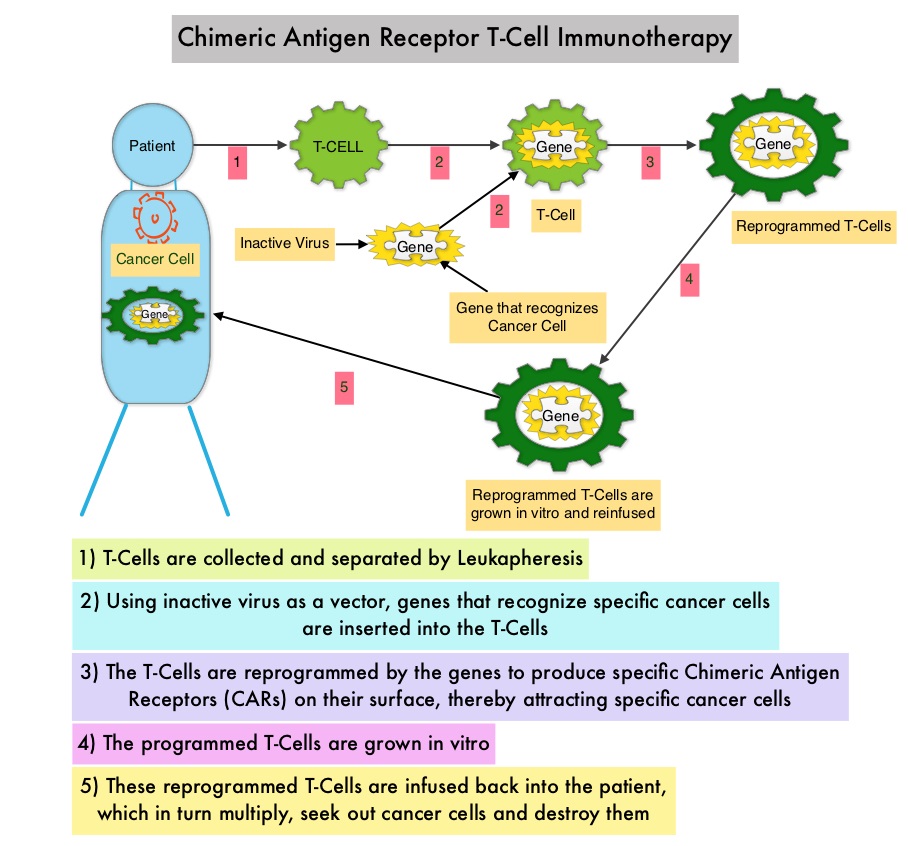 Cytokine Release Syndrome, an inflammatory process is the most common and serious side effect of CAR T-cell therapy and is associated with marked elevation of Interleukin-6. Cytokine release is important for T-cell activation and can result in high fevers and myalgias. This is usually self limiting although if severe can be associated with hypotension and respiratory insufficiency. Tocilizumab (ACTEMRA®), an Interleukin-6 receptor blocking antibody produces a rapid improvement in symptoms. This is however not recommended unless the symptoms are severe and life threatening, as blunting the cytokine response can in turn negate T-cell proliferation. Elevated serum Ferritin and C-reactive protein levels are surrogate markers for severe Cytokine Release Syndrome.
Cytokine Release Syndrome, an inflammatory process is the most common and serious side effect of CAR T-cell therapy and is associated with marked elevation of Interleukin-6. Cytokine release is important for T-cell activation and can result in high fevers and myalgias. This is usually self limiting although if severe can be associated with hypotension and respiratory insufficiency. Tocilizumab (ACTEMRA®), an Interleukin-6 receptor blocking antibody produces a rapid improvement in symptoms. This is however not recommended unless the symptoms are severe and life threatening, as blunting the cytokine response can in turn negate T-cell proliferation. Elevated serum Ferritin and C-reactive protein levels are surrogate markers for severe Cytokine Release Syndrome.
The CAR T-cells have been shown to also access sanctuary sites such as the central nervous system and eradicate cancer cells. CD19 antigen is expressed by majority of the B cell malignancies and therefore most studies using CAR T-cell therapy have focused on the treatment of advanced B-cell malignancies such as Chronic Lymphocytic Leukemia (CLL), Acute Lymphoblastic Leukemia (ALL) and Non Hodgkin lymphoma (NHL), such as Diffuse Large B-Cell Lymphoma (DLBCL). Previously published studies have shown significant responses with CAR T-cell therapy in patients with relapsed and refractory B-cell ALL. But the durability of remission has remained unclear.
This FDA approval was based on ELIANA, an ongoing single-arm, open-label, multicenter, global, phase II study, that has enrolled 88 pediatric/young adult patients with CD19-positive Relapsed/Refractory B-cell ALL and with 5% or more bone marrow lymphoblasts by morphology. The median age was 12 years, 59% of patients had prior allogeneic Stem Cell Transplant and patients had received a median of 3 lines of therapy previously. Following completion of lymphodepleting chemotherapy which in most patients consisted of Fludarabine/Cyclophosphamide, patients were infused with a single dose of KYMRIAH® within 2 to 14 days following the completion of lymphodepleting chemotherapy. The primary endpoint was Overall Remission Rate – Complete Remission [CR] + CR with incomplete blood count recovery [CRi], within 3 months. Secondary endpoints included Duration of Remission (DOR), Overall Survival, Safety, and cellular kinetics.
The authors reported an updated interim analysis with a median study follow up of 6.4 months. Of the 63 patients who were evaluable for efficacy, the Overall Remission Rate was 83%, with 63% of patients achieving a Complete Remission (CR) and 19% achieving a Complete Remission with incomplete hematological recovery (CRi) within 3 months of KYMRIAH® infusion. All patients with a confirmed CR or CRi were Minimal Residual Disease (MRD) negative by flow cytometry. The relapse-free probability at 6 months after remission onset was 75% and the median Duration of Remission has not been reached. The probability of survival at 6 months was 89% and at 12 months was 79%. Thirteen percent (13%) of responders went on to have allogeneic Stem Cell Transplant within 6 months, while in remission.
The most common adverse reactions were Cytokine Release Syndrome (CRS), hypogammaglobulinemia, nausea, diarrhea, vomiting, fever, infections, headache, encephalopathy, hypotension, bleeding episodes, tachycardia, hypoxia and fatigue. Grade 3 or 4 adverse events were noted in 84% of patients. Patients with Severe Cytokine Release Syndrome were effectively treated with the Interleukin-6 receptor blocking antibody Tocilizumab (ACTEMRA®). The expansion of the genetically engineered T-cells in vivo correlated with CRS severity, and persistence of these reprogrammed T cells along with B-cell aplasia in peripheral blood was observed for 1 year or more in some responders.
The authors concluded that the ELIANA trial is the first multicenter trial of a CAR T-cell therapy and a single infusion of KYMRIAH® was highly efficacious, in patients with relapsed and refractory ALL, and was associated with a high and durable remission rate. This technology may be applied to other malignancies, as new antigen targets are identified. Buechner J, Grupp SA, Maude SL, et al. Global registration trial of efficacy and safety of CTL019 in pediatric and young adult patients with relapsed/refractory (r/r) acute lymphoblastic leukemia (ALL): update to the interim analysis. Presented at: 2017 EHA Congress; June 22-25, 2017; Madrid, Spain. Abstract S476.
Antibiotics May Impair the Efficacy of Immune Checkpoint Inhibitors
SUMMARY: The American Cancer Society estimates that about 63,990 new cases of kidney cancer will be diagnosed in the United States in 2017 and about 14,400 patients will die from this disease. The understanding of the Immune checkpoints has lead to the development of novel immunotherapies. Immune checkpoints or gate keepers are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells may be related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies have been developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as PD-1(Programmed cell Death-1), etc. Following inhibition of PD-1 by specific antibodies, T cells are unleashed, resulting in T cell proliferation and activation with subsequent therapeutic responses.
Preclinical studies have suggested that immune-based therapies for cancer may have a very complex interplay with the host’s microbiome and there may be a relationship between gut bacteria and immune response to cancer. Broad-spectrum antibiotics can alter the bacterial composition and bacterial diversity of our gut, by killing the good bacteria. It has been postulated that this may negate the benefits of immunotherapy and influence treatment outcomes. Previously published studies have shown that intestinal microbiota modulates the anticancer immune effects of YERVOY® (Ipilimumab), an Immune checkpoint inhibitor.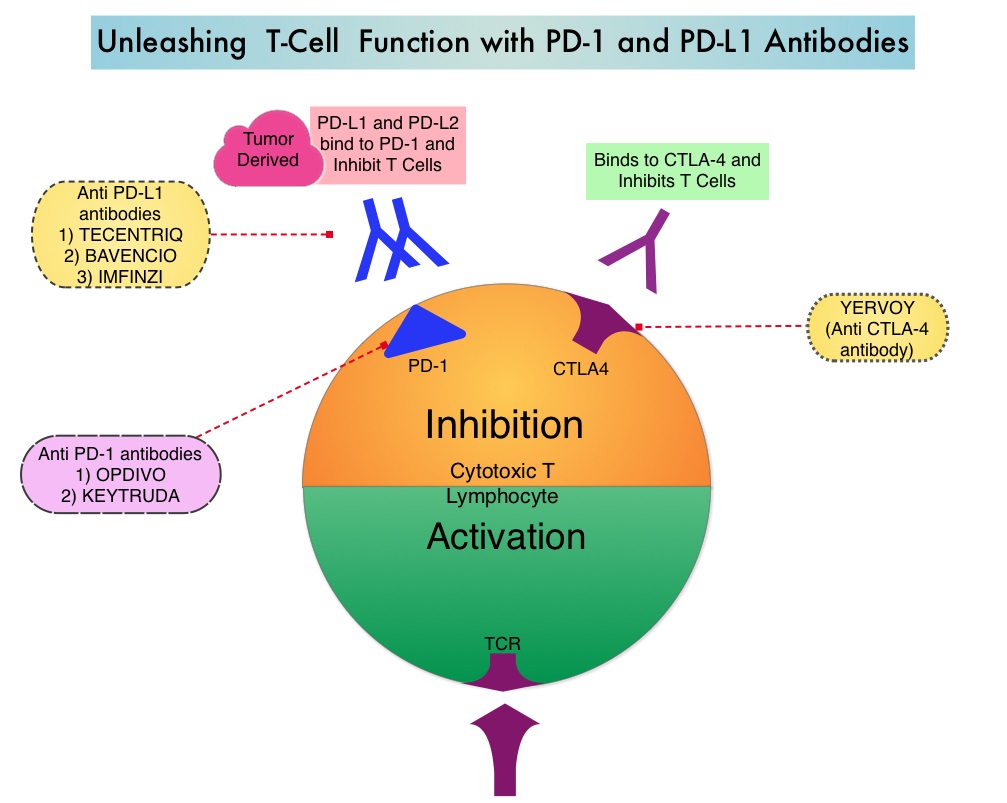
The authors in this publication evaluated the effect of broad-spectrum antibiotic use, in patients with metastatic Renal Cell Carcinoma (mRCC), treated with Immune checkpoint inhibitors. In this study, 80 mRCC patients treated in prospective trials with checkpoint inhibitors were enrolled. These patients had received anti-PD-1/PD-L1 monotherapy, primarily Nivolumab (N=67), a combination of a PD-1 inhibitor and a CTLA-4 inhibitor such as Ipilimumab (N=10), and a combination of anti-PD-L1 therapy and Bevacizumab (N=3). A majority of the patients (65%) were male, 88% had mRCC with clear cell histology, and 80% of the patients had prior nephrectomy. Using IMDC (International Metastatic Renal Cell Carcinoma Database Consortium) criteria, 21% had favorable risk disease, 57% had intermediate risk and 22% had poor risk disease. Sixteen patients (20%) had been treated with broad-spectrum antibiotics, mostly Beta-lactamases or Fluoroquinolones, for up to 1 month prior to starting treatment with immunotherapy. A retrospective analysis was conducted and the Progression Free Survival (PFS), Objective Response Rate (ORR), and Overall Survival (OS), in the group that received broad-spectrum antibiotics, were compared with the group that did not receive broad-spectrum antibiotics.
It was noted that the PFS was four-fold higher in patients who did not receive antibiotics compared to those who received antibiotics (8.1 months vs 2.3 months, P<0.001) and this was statistically significant. This benefit was maintained after adjusting for age, gender, IMDC risk groups, tumor burden and proton pump inhibitors. Additionally, the ORR was higher in those who did not receive antibiotics compared to those who were treated with antibiotics (P<0.002). At a median follow up of less than 6 months, there was already a negative trend in Overall Survival, driven by broad-spectrum antibiotic usage.
It was concluded that in this first analysis, broad-spectrum antibiotics had a negative impact on outcomes, among patients with metastatic Renal Cell Carcinoma, treated with Immune checkpoint inhibitors. Caution should therefore be exercised when prescribing antibiotics to this patient group, so that the efficacy of immunotherapy is not compromised. These concerns may be true across different tumor types and additional follow up is underway. Impact of antibiotics on outcome in patients with metastatic renal cell carcinoma treated with immune checkpoint inhibitors. Derosa L, Routy B, Enot D, et al. J Clin Oncol 35, 2017 (suppl 6S; abstract 462)
Study Finds Dramatic Increase in ColoRectal Cancer Incidence among Young Adults
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. The lifetime risk of developing ColoRectal Cancer is about 1 in 20 (5%).
Even though the incidence of Colorectal cancer (CRC) in the United States has been rapidly declining overall, primarily driven by screening, the incidence however has been increasing among adults younger than age 50 years. To understand this trend, the authors in this publication conducted a retrospective cohort study among 490,305 patients aged 20 years and older, who were diagnosed with colorectal cancer between 1974 and 2013, using data from nine oldest Surveillance, Epidemiology, and End Results (SEER) registries. The SEER program is considered the gold standard for cancer registration worldwide because of the high quality of data and is the only source for historical population-based cancer incidence in the United States. This study included people born in 1890 thru 1990. Colorectal cancer incidence trends were analyzed by 5-year age group and birth cohorts.
The authors noted variations in CRC incidence patterns by age, tumor location in the colon, calendar period, and birth cohort. The study found that in adults aged 20-39 years, after a decrease in the previous decade, colon cancer incidence rates increased by 1.0-2.4% per year since the mid-1980s thru 2013. For adults aged 40-54 years during the same period, colon cancer incidence rates increased by 0.5-1.3%. Conversely, from the mid-1980s thru 2013, colon cancer rates declined in adults aged 55 years and older. In adults younger than age 50 years, there was an increasing trend for tumors to be confined to the distal colon, with the exception of adults aged 40-49 years, among whom there was an also an increasing trend for proximal tumors.
The incidence of rectal cancer has been increasing even longer and faster than colon cancer, rising about 3.2% per year from 1974-2013 in adults aged 20-29 years and from 1980-2013 in adults aged 30-39 years. In adults aged 40 to 54, rectal cancer rates increased by 2.3% per year from the 1990s to 2013. Again, rectal cancer rates declined, in adults aged 55 years and older, from 1974-2013.
Compared with adults born around 1950, those born around 1990 had double the risk of colon cancer and quadruple the risk of rectal cancer. The increase in the incidence of CRC in young adults has been attributed to western style, high carbohydrate, high fat, low fiber diet which can initiate inflammation and proliferation in the colonic mucosa within two weeks. Other lifestyle factors associated with CRC include obesity, high consumption of processed meat and alcohol, low levels of physical activity and cigarette smoking. Further, young patients are 58% more likely than older patients to be diagnosed with advanced versus localized stage CRC, due to delayed follow-up of symptoms, sometimes for years and these young adults are less likely to be screened for colon cancer, despite their symptoms.
The authors concluded that there is an increasing rate of colon and rectal cancer among young and middle-aged adults in the US and compared with adults born around 1950 when the risk was at the lowest, those born around 1990 have double the risk of colon cancer and quadruple the risk of rectal cancer. They added that as nearly a third of rectal cancer patients are younger than age 55 years, screening initiation before age 50 years should be considered. Colorectal Cancer Incidence Patterns in the United States, 1974-2013. Siegel RL, Fedewa SA, Anderson WF, et al. J Natl Cancer Inst. 2017 Aug 1;109(8). doi: 10.1093/jnci/djw322.