
The FDA on March 31, 2017 granted regular approval to IBRANCE® for the treatment of Hormone Receptor (HR) positive, Human Epidermal growth factor Receptor 2 (HER2) negative advanced or metastatic breast cancer, in combination with an Aromatase Inhibitor, as initial endocrine based therapy in postmenopausal women. IBRANCE® is marketed by Pfizer Inc.
Author: RR
TAGRISSO® (Osimertinib)
The FDA on March 30, 2017 granted regular approval to TAGRISSO®, for the treatment of patients with metastatic Epidermal Growth Factor Receptor (EGFR) T790M mutation-positive Non-Small Cell Lung Cancer (NSCLC), as detected by an FDA-approved test, whose disease has progressed on or after EGFR Tyrosine Kinase Inhibitor (TKI) therapy. TAGRISSO® is marketed by AstraZeneca Pharmaceuticals, LP.
BAVENCIO® (Avelumab)
The FDA on May 9, 2017 granted accelerated approval to BAVENCIO® for patients with locally advanced or metastatic urothelial carcinoma whose disease progressed during or following platinum-containing chemotherapy or within 12 months of neoadjuvant or adjuvant platinum-containing chemotherapy. BAVENCIO® is a product of EMD Serono, Inc.
IMFINZI® (Durvalumab)
The FDA on May 1, 2017 granted accelerated approval to IMFINZI®, for the treatment of patients with locally advanced or metastatic urothelial carcinoma, who have disease progression during or following platinum-containing chemotherapy or who have disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy. IMFINZI® is marketed by AstraZeneca UK Limited.
FDA Approves RYDAPT®, A Targeted Multikinase Inhibitor for FLT3-Mutated Acute Myeloid leukemia
SUMMARY: The FDA on April 28, 2017 approved RYDAPT® for the treatment of adult patients with newly diagnosed Acute Myeloid Leukemia (AML) who are FLT3 mutation-positive (FLT3+), as detected by an FDA-approved test, in combination with standard Cytarabine and Daunorubicin induction and Cytarabine consolidation. The American Cancer Society estimates that in 2017, 21,380 new cases of Acute Myeloid Leukemia (AML) will be diagnosed in the United States and 10,590 patients will die of the disease. AML can be considered as a group of heterogeneous diseases with different clinical behavior and outcomes. Cytogenetic analysis has been part of routine evaluation when caring for patients with AML. By predicting resistance to therapy, tumor cytogenetics will stratify patients, based on risk and help manage them accordingly. Even though cytotoxic chemotherapy may lead to long term remission and cure in a minority of patients with favorable cytogenetics, patients with high risk features such as unfavorable cytogenetics, molecular abnormalities, prior myelodysplasia and advanced age, have poor outcomes with conventional chemotherapy alone.
The Fms-Like Tyrosine kinase 3 (FLT3) is a receptor tyrosine kinase in the PDGF family of growth factor receptors located on the cell surface (transmembrane) and plays an important role in both normal and malignant hematopoiesis by activating key signaling pathways. Activating mutations in the FLT3 receptor is the most common genetic abnormality in AML and is detected in approximately 30% of the patients. The three FLT3 mutation subtypes include Tyrosine Kinase Domain (TKD), Internal Tandem Duplications (ITD) high and ITD low. The most common FLT3 mutation is the FLT3-ITD accounting for about 75% of patients with a FLT3 mutation. The presence of FLT3-ITD mutations can negate the benefit of any other favorable molecular and cytogenetic features. Patients with FLT3-ITD mutations are predicted to have poor outcomes with shorter remission duration and significantly decreased leukemia free and overall survival. These mutations are detected using Polymerase Chain Reaction (PCR) based molecular diagnostic DNA testing.

FDA Approves ALUNBRIG® for ALK Positive Non Small Cell Lung Cancer
SUMMARY: The FDA on April 28, 2017 granted accelerated approval to ALUNBRIG® (Brigatinib),for the treatment of patients with metastatic Anaplastic Lymphoma Kinase (ALK)-positive Non Small Cell Lung Cancer (NSCLC), who have progressed on or are intolerant to XALKORI® (Crizotinib). Lung cancer is the second most common cancer in both men and women and accounts for about 14% of all new cancers. It is the leading cause of cancer death among both men and women. The American Cancer Society estimates that over 222,500 new cases of lung cancer will be diagnosed in the United States in 2017 and over 155,870 patients will die of the disease. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 25% are Squamous Cell Carcinomas, 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. The discovery of rearrangements of the Anaplastic Lymphoma Kinase (ALK) gene in some patients with advanced NSCLC and adenocarcinoma histology, led to the development of agents such as XALKORI® (Crizotinib), ZYKADIA® (Ceritinib), ALECENSA® (Alectinib) and now ALUNBRIG® (Brigatinib), with promising results. It has become clear that appropriate, molecularly targeted therapy for tumors with a molecular abnormality, results in the best outcomes. According to the US Lung Cancer Mutation Consortium (LCMC), two thirds of patients with advanced adenocarcinoma of the lung, have a molecular driver abnormality. The most common oncogenic drivers in patients with advanced adenocarcinoma of the lung are, KRAS in 25%, EGFR in 21% and ALK in 8% as well as other mutations in BRAF, HER2, AKT1 and fusions involving RET and ROS oncogenes. These mutations are mutually exclusive, and the presence of two simultaneous mutations are rare.
The approval was based on findings from the ALTA trial, which is a pivotal, open-label multicenter study in which 222 patients were randomized 1:1 ratio to receive ALUNBRIG® 90 mg orally once daily (N=112) or 180 mg once daily following a 7-day lead-in at 90 mg orally once daily (N=110). Two dose regimens were evaluated in this study, as clinical responses and Adverse Events varied with starting dose of ALUNBRIG®, in a previous Phase I/II study. Eligible patients had locally advanced or metastatic ALK-positive NSCLC, who had progressed on XALKORI®. The median age of patients across the study was 54 years and 67% of the patients had brain metastases. Patients were stratified by presence of brain metastases at baseline and best response to prior treatment with XALKORI®. The Primary endpoint was Objective Response Rate (ORR) and Secondary endpoints included Progression Free Survival (PFS) and CNS response.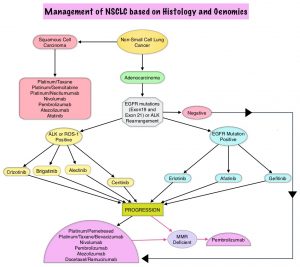
The ORR was 48% in the 90 mg dose group and 53% in the 180 mg dose group. After a median duration of follow up of 8 months, median duration of response was 13.8 months in both treatment groups. In patients with measurable brain metastases at baseline, intracranial ORR was 42% in the 90 mg group and 67% in the 180 mg group. Among patients who exhibited an intracranial response, 78% of patients in the 90 mg group and 68% of patients in the 180 mg group maintained an intracranial response for at least 4 months. The median PFS was 8.8 months in the 90 mg dose group, and 11.1 months in the 180mg dose group. The most common adverse reactions, were nausea, diarrhea, fatigue, cough, and headache. The most common serious adverse reactions were pneumonia and pneumonitis.
The authors concluded that treatment with ALUNBRIG® resulted in significant response rates and improved Progression Free Survival, with acceptable toxicity profile. The recommended dosing regimen of ALUNBRIG® is 90 mg orally once daily for the first 7 days and if tolerated, the dose is increased to 180 mg orally once daily.
Kim D-W, Tiseo M, Ahn M-J, et al. Brigatinib (BRG) in patients (pts) with crizotinib (CRZ)-refractory ALK+ non-small cell lung cancer (NSCLC): First report of efficacy and safety from a pivotal randomized phase (ph) 2 trial (ALTA). J Clin Oncol. 2016;34 (suppl; abstr 9007).
Management of Localized or Locally Advanced Oropharyngeal Squamous Cell Carcinoma – ASTRO Clinical Practice Guideline
SUMMARY: The American Cancer Society estimates that 49,670 people will be diagnosed with Oral cavity and Oropharyngeal cancer in 2017 and an estimated 9700 patients will die of the disease. Over 90% of these malignancies are Squamous Cell Carcinomas (SCCs). OroPharyngeal Squamous Cell Carcinoma (OPSCC) involves the tonsils and base of the tongue, and recent studies have shown that over 70% of these tumors are caused by Human Papilloma Virus (HPV) and HPV-16 is the predominant type present in the tumor cells. The CDC estimates that more than 2,370 new cases of Human Papilloma Virus associated OPSCC are diagnosed in women and nearly 9,356 are diagnosed in men, each year in the United States, and this incidence has been on the rise.
The American Society for Radiation Oncology (ASTRO) convened the OroPharyngeal Squamous Cell Carcinoma (OPSCC) Guideline Panel which consisted of a multidisciplinary team of radiation, medical, and surgical oncologists, to perform a systematic literature review of studies published from January 1990 through December 2014, in an attempt to present evidence-based guidelines, for the treatment of OPSCC, with definitive or adjuvant Radiation Therapy (RT).
The following are the key questions and recommendations of the Guideline panel.
(1) When is it appropriate to add systemic therapy to definitive RT in the treatment of OPSCC?
Stage IVA-B disease
A) Patients with stage IVA-B tumors receiving definitive RT should receive concurrent high-dose intermittent Cisplatin.
B) Patients who are medically unfit for high-dose Cisplatin should receive concurrent Cetuximab or Carboplatin-Fluorouracil.
C) Weekly Cisplatin may be considered for patients who are medically unfit for high-dose Cisplatin.
D) Concurrent Cetuximab should not be administered in combination with chemotherapy.
E) Intra-arterial chemotherapy should not be used in this patient group.
Stage III disease
A) Patients with T3 N0-1 tumors should receive concurrent systemic therapy.
B) Patients with T1-T2 N1 tumors who are at a significant risk for locoregional recurrence may be considered for concurrent systemic therapy.
Stage I to II disease
Concurrent systemic therapy is not recommended for this patient group as there is no evidence supporting the use of systemic therapy in this generally favorable population.
(2) When is it appropriate to deliver PostOperative RT (PORT) with and without systemic therapy following primary surgery for OPSCC?
A) Concurrent high-dose intermittent Cisplatin should be delivered with PORT to patients with positive surgical margins and/or extracapsular nodal extension, independent of HPV status or the extent of extranodal tumor.
B) Concurrent weekly Cisplatin may be administered with PORT to patients who are considered inappropriate for standard high-dose intermittent Cisplatin, after a careful discussion of patient preferences and the limited evidence supporting this treatment schedule.
C) For the high-risk postoperative patient unable to receive Cisplatin-based concurrent chemoradiation therapy, RT alone should be routinely delivered without concurrent systemic therapy. Given the limited evidence supporting alternative regimens, treatment with non-Cisplatin systemic therapy should be accompanied by a careful discussion of the risks and unknown benefits of the combination.
D) Patients treated with PORT should not receive concurrent weekly Carboplatin, weekly Docetaxel or Cetuximab, either alone or in combination with chemotherapy, although such regimens are currently under investigation.
E) Patients treated with PORT should not receive concurrent Mitomycin-C, alone or with Bleomycin, given the limited evidence and experience supporting its use.
F) Postoperative chemotherapy should not be delivered alone or sequentially with postoperative RT.
Intermediate-risk pathologic factors such as lymphovascular invasion (LVI), perineural invasion (PNI), T3-4 disease, or positive lymph nodes
A) These patients should not routinely receive concurrent systemic therapy with PORT.
B) Concurrent Cisplatin-based chemotherapy may be considered if the post operative pathologic findings suggest significant risk of locoregional recurrence.
C) PORT should be delivered to patients with pathologic T3 or T4 and pathologic N2 or N3 disease.
D) PORT may be delivered to patients with pathologic N1 disease after a careful discussion with the patient.
E) PORT may be delivered to patients with LVI and/or PNI as the only risk factor(s), after a careful discussion with the patient.
No pathologic risk factors
PORT may be delivered to patients without conventional adverse pathologic risk factors only if the clinical and surgical findings imply a particularly significant risk of locoregional recurrence and after a careful discussion with the patient.
(3) When is it appropriate to use induction chemotherapy in the treatment of OPSCC?
Induction Chemotherapy should not be routinely delivered to patients with OPSCC.
(4) What are the appropriate dose, fractionation, and volume regimens with and without systemic therapy in the treatment of OPSCC?
A) For patients with stage III-IV disease a dose of 70 Gy over 7 weeks should be delivered to gross primary and nodal disease.
B) The biologically equivalent dose of approximately 50 Gy in 2 Gy fractions or slightly higher should be delivered electively to clinically and radiographically negative regions at-risk for microscopic spread of tumor.
C) Altered fractionation should be used in patients with stage IVA-B disease treated with definitive RT, who are not receiving concurrent systemic therapy as well as patients with T3 N0–1 disease not receiving concurrent chemoradiation. Additionally, it may be considered for patients with T1–2 N1 or T2 N0 disease at high risk for recurrence.
D) When treating OPSCC with concurrent systemic therapy,, either standard or accelerated fractionation may be implemented.
Adjuvant PORT
Adjuvant PORT should be delivered to regions of microscopically positive primary site surgical margins and extracapsular nodal extension at 2 Gy/fraction once daily to a total dose between 60 and 66 Gy.
Early T-stage tonsillar carcinoma
A) Unilateral RT should be delivered to patients with well-lateralized (confined to tonsillar fossa) T1-T2 tonsillar cancer and N0-N1 nodal category.
B) Unilateral RT may be delivered to patients with lateralized (<1 cm of soft palate extension but without base of tongue involvement) T1-T2 N0-N2a tonsillar cancer, without clinical or radiographic evidence of extracapsular extension, after careful discussion of patient preferences and the relative benefits of unilateral treatment versus the potential for contralateral nodal recurrence and subsequent salvage treatment.
Radiation therapy for oropharyngeal squamous cell carcinoma: Executive summary of an ASTRO Evidence-Based Clinical Practice Guideline. Sher DJ, Adelstein DJ, Bajaj GK, et al. DOI: http://dx.doi.org/10.1016/j.prro.2017.02.002
PET-CT in Colorectal Cancer Patients with a Rising CEA Can Detect Occult Recurrent Disease Amenable to Curative Therapy
SUMMARY: ColoRectal Cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States. The American Cancer Society estimates that approximately 135,430 new cases of ColoRectal Cancer will be diagnosed in the United States in 2017 and over 50,260 patients are expected to die of the disease. Patients with ColoRectal Carcinoma are often followed up with regular CEA measurements after curative surgical resection and a rising CEA may be the first sign of CRC recurrence and warrants further investigation. Approximately 50% of the patients with early-stage disease after surgical resection will relapse with metastatic disease, during the first 3 years of follow-up. They may present with synchronous disease defined as distant metastases occurring within 6 months, and metachronous disease defined as distant metastases occuring beyond 6 months, of the primary diagnosis of CRC. These patients with oligo-metastatic disease, when detected early, may be potentially curable.
The authors in this study sought to (a) evaluate the utility of PET-CT in detecting occult disease recurrence in patients with raised CEA and (b) establish the prognostic effects of early detection of disease recurrence in patients with CRC. This retrospective analysis screened1200 patients from 2004 to 2010, with a confirmed diagnosis of CRC, who on follow up after curative therapy underwent FDG PET-CT imaging, for an elevated CEA, after normal findings on conventional investigations. Patients who had already received treatment with curative intent for synchronous or metachronous oligo-metastatic disease, including surgical resection, radiofrequency ablation (RFA), and radical chemoradiation, were also included. An elevated CEA level was defined as more than 3 ng/mL in nonsmokers and more than 5 ng/mL in smokers. A minimum of clinical and radiological follow up for 12 months or histopathological confirmation, were required, to ascertain recurrent disease. Eighty eight (N=88) patients who underwent PET-CT imaging because of any clinical indication and met the eligibility criteria, were included in the study. The mean age of patients was 66 years and 59% were male.
Recurrent disease was confirmed in 64% of the patients within the 12 months after their FDG PET-CT scan and the PET scan was able to detect the site of subtle relapse. The sensitivity of PET-CT to detect recurrence was 88% and the specificity was 88% as well. Fifty five percent (55%) of the patients with PET-CT-detected relapsed disease were deemed eligible for further curative therapy of whom 70% went on to receive potentially curative therapy. The Positive Predictive Value and Negative Predictive Value for FDG PET-CT to predict recurrence were 93% and 80% respectively.
The median Time To Progression for patients who received potentially curative therapy for the PET-CT-detected recurrence was 8.8 months versus 2.2 months for the patients not treated with curative intent. The median Overall Survival was 39.9 months for those who received potentially curative treatment versus 15.6 months for those who did not receive curative therapy. The 5-year survival rate in the curative group was 36.8% versus 6.1% in the non-curative group (P <0.001).
The authors concluded that early use of FDG PET-CT in patients with rising CEA levels is a highly sensitive and specific tool for the detection of occult ColoRectal Cancer recurrence, and in more than 50% of these patients, recurrent disease may still be amenable to curative therapy, and long-term survival can be achieved in a subgroup of this patient population. Survival Outcomes in Asymptomatic Patients With Normal Conventional Imaging but Raised Carcinoembryonic Antigen Levels in Colorectal Cancer Following Positron Emission Tomography-Computed Tomography Imaging. Khana K, Athaudaa A, Aitken K, et al. The Oncologist 2016;21:1502-1508
Pegylated Form of Recombinant Hyaluronidase Significantly Improves Progression Free Survival in Metastatic Pancreatic Cancer
SUMMARY: The American Cancer Society estimates that in 2017, about 53,670 people will be diagnosed with pancreatic cancer in the United States and about 43,090 patients will die of the disease. Some important risk factors for pancreatic cancer include increasing age, obesity, smoking history, genetic predisposition, exposure to certain dyes and chemicals, heavy alcohol use and pancreatitis. The best chance for long term survival is complete surgical resection, although this may not be feasible in a majority of the patients, as they present with advanced disease at the time of diagnosis. Based on the National Cancer Data Base, the 5 year observed survival rate for patients diagnosed with exocrine cancer of the pancreas is 14% for those with Stage IA disease and 1% for those with Stage IV disease. The FDA approved ABRAXANE® ((Paclitaxel albumin-bound particles) for use in combination with GEMZAR® (Gemcitabine) for the first line treatment of patients with metastatic adenocarcinoma of the pancreas. This approval was based on the demonstration of improved Overall Survival (OS) and Progression Free Survival (PFS), in a multicenter, international, open-label, randomized trial (MPACT study), when compared to single agent GEMZAR®.
PEGPH20 is a PEGylated form of recombinant human Hyaluronidase, for the potential systemic treatment of tumors that accumulate Hyaluronan (HA). PEGPH20 is an enzyme that temporarily degrades Hyaluronan, a dense component of the tumor microenvironment that can accumulate in higher concentrations around certain cancer cells and potentially constrict blood vessels and there by impede treatment access to tumor tissue. It is estimated that 35% to 40% of patients with pancreatic cancer have high expression of Hyaluronan and this biomarker may predict response to PEGPH20.
HALO 202 (Halo 109-202) is a phase 2 multicenter, randomized clinical trial, in which PEGPH20 in combination with ABRAXANE® and GEMZAR® was compared with ABRAXANE® and GEMZAR® alone, in treatment naive patients with metastatic pancreatic carcinoma. In this study, following enrollment of 146 patients in the first stage of the trial, the study was placed on hold to address concerns regarding thromboembolic events, in the group receiving PEGPH20. The protocol was amended to exclude those at high risk for a thromboembolic event and prophylaxis with Low Molecular Weight Heparin was required. One hundred thirty-three patients (N=133) were enrolled into the second stage of the trial for a total of 279 patients. Patients enrolled in stage 2 received Low Molecular Weight Heparin at a starting dose of 40 mg/day or 1 mg/kg/day, to prevent thromboembolic events. PEGPH20 was administered at 3 µg/kg twice weekly for cycle 1 followed by weekly administration in subsequent cycles. ABRAXANE® and GEMZAR® were administered at their standard FDA-approved doses. Tumor biopsy samples for the Hyaluronan analysis were available for 138 patients treated with PEGPH20 and 79 patients treated in the control group across both stages of the study. Overall, 49 patients in the PEGPH20 arm and 35 in the control group had Hyaluronan expression of 50% or more. The primary endpoint of the study was Progression Free Survival (PFS) across the entire treatment group. Following change in the treatment protocol, a second primary endpoint was added to assess thromboembolic event rate. Secondary endpoints included Objective Response Rate, PFS by Hyaluronan level, and Overall Survival. The second stage of this study was also utilized to validate a companion diagnostic for Hyaluronan (HA) levels.
It was noted that across the overall study population, there was a statistically significant increase in Progression Free Survival (PFS) in patients with high levels of Hyaluronan (HA-High) treated with PEGPH20 plus ABRAXANE® and GEMZAR®, compared to HA-High patients receiving ABRAXANE® and GEMZAR® alone. Among the patients in the second stage of this study, there was a 91% improvement in median PFS for HA-High patients in the PEGPH20 group compared to the control group (8.6 months versus 4.5 months) and the additional primary endpoint of a reduction in the rate of thromboembolic events was achieved, in the PEGPH20 group. Across all patients, thromboembolic events were experienced by 14% of those in the PEGPH20 group versus 10% of those in the ABRAXANE® and GEMZAR® group. These events were lower in those receiving Low Molecular Weight Heparin at 1 mg/kg/day dose versus 40 mg/day (6% vs 10%, respectively). The most common adverse events were cytopenias.
The authors concluded that the addition of PEGPH20 to ABRAXANE® and GEMZAR® resulted in significant improvement in Progression Free Survival compared with ABRAXANE®/GEMZAR® alone, in treatment naïve patients with advanced pancreatic cancer. Patients with high levels of expression of the biomarker Hyaluronan, had the best outcomes suggesting that a biopsy-based biomarker for hyaluronan content can potentially identify patients who will have a meaningfully greater response when PEGPH20 is added to standard chemotherapy. A phase III study is underway, evaluating PEGPH20 in combination with ABRAXANE® and GEMZAR® in patients with metastatic pancreatic cancer, with high Hyaluronan levels. Countouriotis A. Study 202 Overall Results and Stage 2 Results [webcast]. Halozyme Investor Call; January 5, 2017. Final analysis of stage 1 data from a randomized phase II study of PEGPH20 plus nab-Paclitaxel/gemcitabine in stage IV previously untreated pancreatic cancer patients (pts), utilizing Ventana companion diagnostic assay. Bullock AJ, Hingorani SR, Wu XW, et al. J Clin Oncol 34, 2016 (suppl; abstr 4104)
Lower Dose of XARELTO® Adequate for Prevention of Recurrent Venous Thromboembolism
SUMMARY: The Center for Disease Control and Prevention (CDC) estimates that approximately 1-2 per 1000 individuals develop Deep Vein Thrombosis/Pulmonary Embolism (PE) each year in the United States, resulting in 60,000-100,000 deaths. Venous ThromboEmbolism (VTE) is the third leading cause of cardiovascular mortality, after myocardial infarction and stroke. With the exception of those with active malignancy, patients with VTE are often treated with Direct Oral Anticoagulant agents such as XARELTO® (Rivaroxaban) over vitamin K antagonists such as Warfarin because, Direct Oral Anticoagulant agents do not require routine laboratory monitoring or dose adjustment, have fewer interactions with food or other drugs and are associated with a lower risk of bleeding complications. Anticoagulation therapy is usually recommended for 3 months following an initial episode VTE in association with a transient risk factor such as surgery. In patients without reversible risk factors however, the risk of recurrent VTE is 10% or more during the first year, if anticoagulation therapy is discontinued. Extended anticoagulation therapy beyond 6 to 12 months even though effective is often not a common practice, for the fear of bleeding complications. Aspirin has been shown to reduce the risk of recurrent VTE when compared with placebo, but recurrence rate with this intervention is still significant at 5.1% per year. 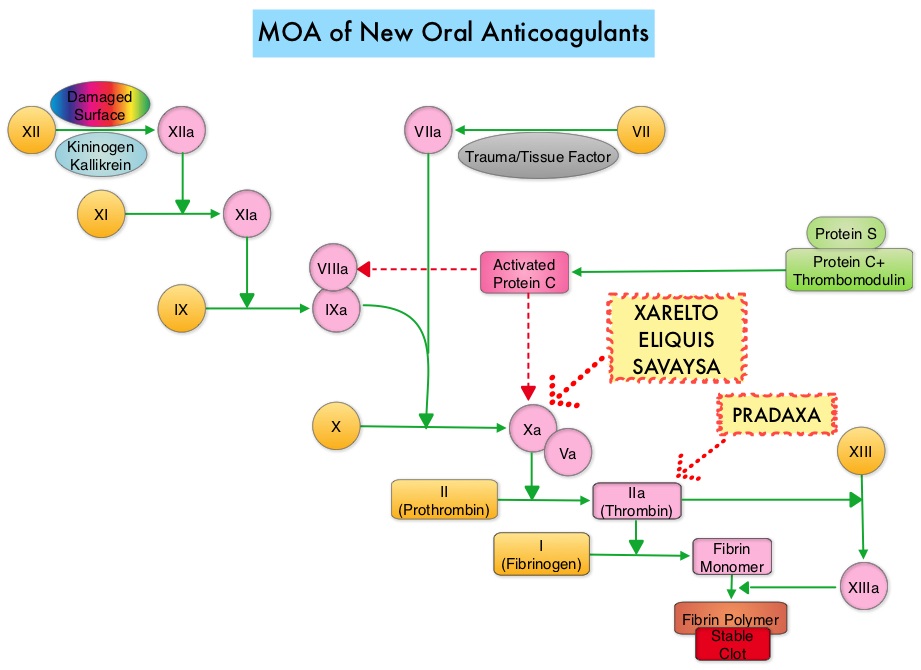
The authors in this study compared the efficacy and safety of two doses of XARELTO® with Aspirin, in patients with Venous ThromboEmbolism, who had completed 6 to 12 months of anticoagulation therapy, and in whom there was uncertainty regarding the need for continued anticoagulation. In this randomized, double-blind, phase III trial, 3396 (N=3396) patients with Venous ThromboEmbolism were assigned, in a 1:1:1 ratio, to receive either XARELTO® 20 mg, XARELTO® 10 mg or Aspirin 100 mg given once daily. The primary efficacy outcome was symptomatic recurrent fatal or nonfatal Venous ThromboEmbolism, and the principal safety outcome was major bleeding. Secondary endpoints included whether the lower dose of XARELTO® was as effective as the higher dose and whether it was associated with less bleeding.
It was noted that after a median duration of treatment of 351 days, symptomatic recurrent fatal or nonfatal Venous ThromboEmbolism or unexplained death occurred in 1.5% of the patients assigned to XARELTO® 20 mg and 1.2% of the patients assigned to XARELTO® 10 mg compared with 4.4% among the patients assigned to the Aspirin group (P<0.001). Major or clinically relevant non-major bleeding occurred in 3.3%, 2.4%, and 2.0% of the patients, respectively.
It was concluded that among patients with Venous ThromboEmbolism for whom continued anticoagulation is a consideration, after an initial treatment course at usual therapeutic doses, the risk of a recurrent thromboembolic events were significantly lower with XARELTO® given at either a therapeutic dose (20 mg) or a prophylactic dose (10 mg), compared with Aspirin. There was no significant increase in bleeding rates. Rivaroxaban or Aspirin for Extended Treatment of Venous Thromboembolism. Weitz JI, Lensing AW, Prins MH, et al. for the EINSTEIN CHOICE Investigators. N Engl J Med 2017; 376:1211-1222