
SUMMARY: The FDA on November 5, 2014 approved CYRAMZA® (Ramucirumab) for use in combination with TAXOL® (Paclitaxel) for the treatment of patients with advanced gastric or GastroEsophageal Junction (GEJ) adenocarcinoma. CYRAMZA® was approved by the FDA in April, 2014 as a single agent for the treatment of patients with advanced gastric or GEJ adenocarcinoma, refractory to or progressive, following first-line therapy with platinum or fluoropyrimidine chemotherapy. It is estimated that there were approximately 21,600 new cases and 10,990 deaths from gastric cancer in the United States in 2013. The biology of gastric cancer appears to be different in different parts of the globe. Following progression after first line treatment for metastatic disease, the median survival is approximately 3 months. CYRAMZA® is a human IgG1 monoclonal antibody that inhibits VEGF-receptor 2, unlike AVASTIN® (Bevacizumab) which inhibits VEGF-A.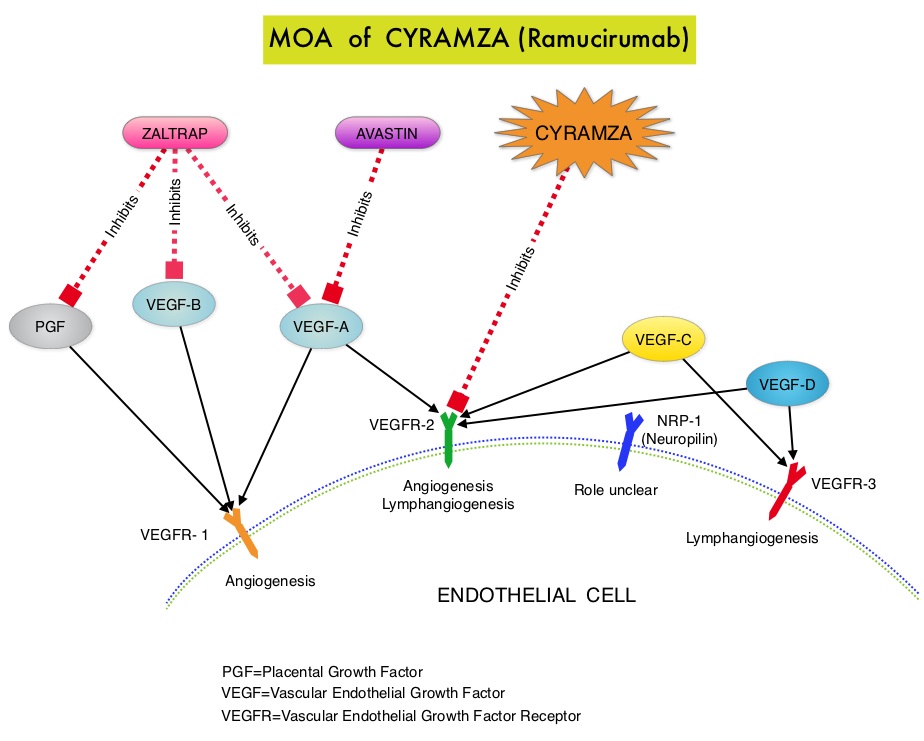 The RAINBOW study is an international, placebo-controlled, double-blind, phase III trial in which 665 patients with metastatic gastroesophageal junction or gastric adenocarcinoma, who had disease progression on or within 4 months after first-line platinum and fluoropyrimidine-based combination therapy, were included. Patients were randomly assigned to receive TAXOL® (Paclitaxel) 80 mg/m2 given on D1, 8, 15 along with Placebo (N=335) or the same dose and schedule of TAXOL® given along with CYRAMZA® at 8 mg/kg IV every 2 weeks (N=330), of a 28 day cycle. Treatment was continued until disease progression or unacceptable toxicities were noted. The primary endpoint was Overall Survival (OS). Secondary endpoints included Progression Free Survival (PFS), Objective Response Rate (ORR) and Time To Progression (TTP). The median OS for the combination of CYRAMZA® and TAXOL® was 9.6 months compared to 7.4 months for Placebo and TAXOL® (HR=0.81; P=0.017), resulting in a 19% reduction in the risk of death with the CYRAMZA® and TAXOL® combination. The secondary endpoints favored the CYRAMZA® and TAXOL® combination as well. The median PFS was 4.4 months and 2.9 months (HR=0.64; P<0.001), ORR was 28% and 16% (P<0.0001) and median TTP was 5.5 months and 3 months with the CYRAMZA® and TAXOL® combination vs Placebo and TAXOL® combination respectively. As one would expect, treatment related adverse events were seen more frequently in the CYRAMZA® and TAXOL® combination group. Significant were neutropenia, hypertension, fatigue and asthenia, diarrhea and epistaxis. The incidence of febrile neutropenia in the two treatment groups was however comparable (3.1% vs 2.4%). The authors concluded that the combination of CYRAMZA® and TAXOL® combination significantly improved both Progression Free and Overall Survival and also resulted in significantly improved disease control rates, in patients with metastatic gastroesophageal junction or gastric adenocarcinoma. Wilke H, Van Cutsem E, Oh SC, et al. J Clin Oncol 32, 2014 (suppl 3; abstr LBA7)
The RAINBOW study is an international, placebo-controlled, double-blind, phase III trial in which 665 patients with metastatic gastroesophageal junction or gastric adenocarcinoma, who had disease progression on or within 4 months after first-line platinum and fluoropyrimidine-based combination therapy, were included. Patients were randomly assigned to receive TAXOL® (Paclitaxel) 80 mg/m2 given on D1, 8, 15 along with Placebo (N=335) or the same dose and schedule of TAXOL® given along with CYRAMZA® at 8 mg/kg IV every 2 weeks (N=330), of a 28 day cycle. Treatment was continued until disease progression or unacceptable toxicities were noted. The primary endpoint was Overall Survival (OS). Secondary endpoints included Progression Free Survival (PFS), Objective Response Rate (ORR) and Time To Progression (TTP). The median OS for the combination of CYRAMZA® and TAXOL® was 9.6 months compared to 7.4 months for Placebo and TAXOL® (HR=0.81; P=0.017), resulting in a 19% reduction in the risk of death with the CYRAMZA® and TAXOL® combination. The secondary endpoints favored the CYRAMZA® and TAXOL® combination as well. The median PFS was 4.4 months and 2.9 months (HR=0.64; P<0.001), ORR was 28% and 16% (P<0.0001) and median TTP was 5.5 months and 3 months with the CYRAMZA® and TAXOL® combination vs Placebo and TAXOL® combination respectively. As one would expect, treatment related adverse events were seen more frequently in the CYRAMZA® and TAXOL® combination group. Significant were neutropenia, hypertension, fatigue and asthenia, diarrhea and epistaxis. The incidence of febrile neutropenia in the two treatment groups was however comparable (3.1% vs 2.4%). The authors concluded that the combination of CYRAMZA® and TAXOL® combination significantly improved both Progression Free and Overall Survival and also resulted in significantly improved disease control rates, in patients with metastatic gastroesophageal junction or gastric adenocarcinoma. Wilke H, Van Cutsem E, Oh SC, et al. J Clin Oncol 32, 2014 (suppl 3; abstr LBA7)
Author: RR
Promise and Pitfalls of Heavy-Particle Therapy
SUMMARY: Radiation Therapy involves the use of X-Rays, gamma rays and charged particles for cancer treatment. External-beam radiation therapy is most often delivered using a linear accelerator in the form of Photon beams (either x-rays or gamma rays). Photons have no mass and are packets of energy of an electromagnetic wave. Electrons and Protons are charged particles and Electrons are considered light particles whereas Protons are considered heavy particles. Electron beams are used to irradiate skin and superficial tumors, as they are unable to penetrate deep into the tissues.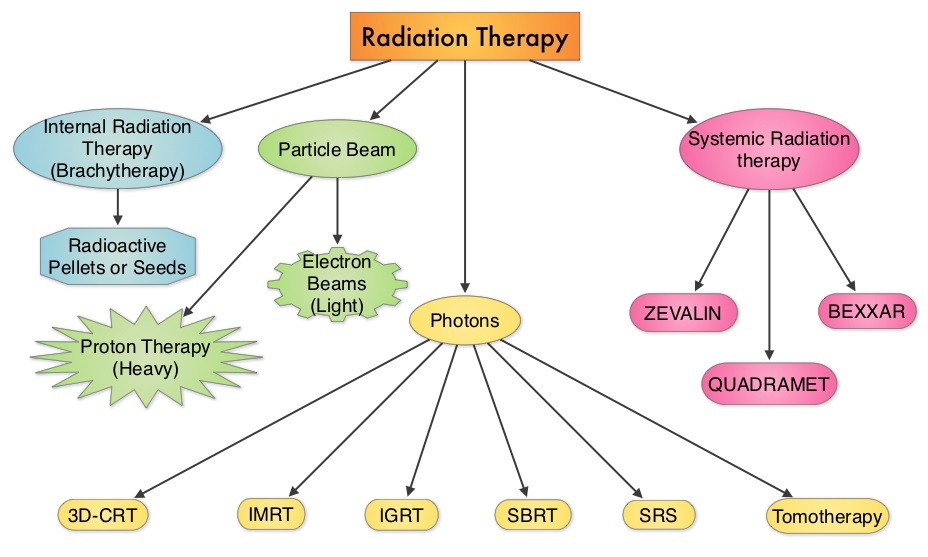 The different types of external beam radiation treatments include 3-Dimensional Conformal Radiation Therapy (3D-CRT) meant to deliver radiation to very precisely shaped target areas, IMRT or Intensity Modulated Radiation Therapy which allows different areas of a tumor or nearby tissues to receive different doses of radiation, Image Guided Radiation Therapy (IGRT) which allows reduction in the planned volume of tissue to be treated as changes in a tumor size are noted during treatment, Stereotactic RadioSurgery (SRS) which can deliver one or more high doses of radiation to a small tumor, Stereotactic Body Radiation Therapy (SBRT) or CYBERKNIFE® which is similar to SRS but also takes the normal motion of the body into account while treating malignancies involving the lung and liver and Proton Beam therapy. Proton beams unlike Photons, enter the skin and travel through the tissues and deposit much of their energy at the end of their path (known as the Bragg peak) and deposit less energy along the way. This is unlike Photons which deposit energy all along the path through the tissues and the deposited dose decreases with increasing depth. As a result, with Proton beam therapy, normal tissues are exposed to less radiation compared with Photons. Despite this advantage, tissue heterogeneity such as organ motion, tumor volume changes during treatment can have a significant negative impact on target coverage for Proton beam therapy and can result in damage to the surrounding tissues and potential complications. The authors in this review discussed the clinical applications of Proton therapy in Adult and Pediatric malignancies. Pediatric patients with malignancies have greater benefit with Proton beam therapy, with a statistically significant lower risk of secondary malignancies and less damage to the developing tissues and organs, compared to Photon therapy (External Beam Radiation Therapy). This clinical benefit may be less so in adult malignancies in spite of superior dosimetry, compared to external beam radiation, as adults are less prone to secondary malignancies compared to children.
The different types of external beam radiation treatments include 3-Dimensional Conformal Radiation Therapy (3D-CRT) meant to deliver radiation to very precisely shaped target areas, IMRT or Intensity Modulated Radiation Therapy which allows different areas of a tumor or nearby tissues to receive different doses of radiation, Image Guided Radiation Therapy (IGRT) which allows reduction in the planned volume of tissue to be treated as changes in a tumor size are noted during treatment, Stereotactic RadioSurgery (SRS) which can deliver one or more high doses of radiation to a small tumor, Stereotactic Body Radiation Therapy (SBRT) or CYBERKNIFE® which is similar to SRS but also takes the normal motion of the body into account while treating malignancies involving the lung and liver and Proton Beam therapy. Proton beams unlike Photons, enter the skin and travel through the tissues and deposit much of their energy at the end of their path (known as the Bragg peak) and deposit less energy along the way. This is unlike Photons which deposit energy all along the path through the tissues and the deposited dose decreases with increasing depth. As a result, with Proton beam therapy, normal tissues are exposed to less radiation compared with Photons. Despite this advantage, tissue heterogeneity such as organ motion, tumor volume changes during treatment can have a significant negative impact on target coverage for Proton beam therapy and can result in damage to the surrounding tissues and potential complications. The authors in this review discussed the clinical applications of Proton therapy in Adult and Pediatric malignancies. Pediatric patients with malignancies have greater benefit with Proton beam therapy, with a statistically significant lower risk of secondary malignancies and less damage to the developing tissues and organs, compared to Photon therapy (External Beam Radiation Therapy). This clinical benefit may be less so in adult malignancies in spite of superior dosimetry, compared to external beam radiation, as adults are less prone to secondary malignancies compared to children.
ADULT MALIGNANCIES
Prostate Cancer: Majority of the patients receiving Proton beam treatment in the United States have prostate cancer. Several randomized trials have concluded that higher radiation dose to the prostate gland leads to better tumor control. Proton beam therapy may deliver this promise, but with associated toxicities, in particular rectal bleeding. This is by virtue of the anatomy of the prostate gland which is deep in the pelvis. Outcomes and patient reported side effects were similar when men with prostate cancer were treated with similar doses of radiation using either Proton beam therapy or External beam radiation therapy. The American Society of Therapeutic Radiology and Oncology (ASTRO) has recommended that Proton beam therapy for patients with prostate cancer should be offered in the context of a clinical trial or registry, as there is not enough evidence suggesting clinical benefit in this patient population.
Breast Cancer: Proton beam therapy may be of value in select situations, such as patients with bilateral implants after mastectomy and in clinical scenarios where cardiac or pulmonary risks with Photon therapy are not acceptable. This is because of a significant reduction in the radiation doses to the heart, lung and contralateral breast with Proton therapy compared to Photon therapy.
Lung Cancer: Proton beam therapy for NSCLC (Non Small Cell Lung Cancer) is in the early stages of evaluation and has the advantage of reduced radiation to the normal lung and heart. This may be relevant in patients with inoperable early stage NSCLC with poor lung function, prior chest irradiation or in those with multifocal lung cancers requiring more than one treatment course. Proton therapy can be of significant value in patients with Stage IIIA NSCLC who in addition to chemoradiation may be candidates for pneumonectomy, thus sparing the contralateral lung from radiation related toxicities.
Head and Neck Cancers: Proton therapy may be of value in nasopharyngeal carcinoma and malignancies involving the oropharynx and paranasal sinuses. Proton therapy limits the radiation dose to the brain stem, optic structures, mandible and salivary glands, decreasing the risk of xerostomia and osteoradionecrosis of the mandible.
GI Malignancies: Proton beam therapy is the preferable treatment for hepatocellular carcinoma in patients with Child-Pugh class B and class C cirrhosis, as it is able to spare more liver tissue from radiation.
Brain Tumors: Meningiomas are ideal tumors for Proton beam therapy, with less cerebral adverse events and therefore has a positive impact on quality of life of patients. Clinical trials are underway to test this hypothesis.
PEDIATRIC TUMORS
Medulloblastoma- CranioSpinal Irradiation: There is a significant long term advantage with Proton CranioSpinal Irradiation compared to conventional or IMRT photon CSI. There is a 6-12 times lower risk of secondary malignancies due to lower radiation doses to normal tissues. This is more relevant because craniospinal axis irradiation results in the most exposure of a childs tissue to radiation.
Rhabdomyosarcoma: This is the most common soft tissue sarcoma in children arising in the head and neck region and Proton therapy can significantly reduce the mean doses to the retina, optic nerve, parotid and cochlea.
Ependymoma, Craniopharyngioma, Retinoblastoma and Glioma: Proton therapy for these tumors has been associated with lower acute and long term toxicities as well lower risk of secondary malignancies.
The authors concluded that the most benefit for Proton beam therapy is in pediatric malignancies, no significant benefit in skin cancer and marginal benefit in adult lung and prostate cancer. With ongoing advances in the delivery of Proton therapy such as Intensity Modulated Proton Therapy (IMPT) and other expensive therapeutic interventions, economics will take precedence, until and unless a clear clinical benefit is proven. Mitin T and Zietman AL. J Clin Oncol 2014;32:2855-2863
Phase II study of nivolumab (Anti-PD-1, BMS-936558, ONO-4538) in patients with advanced, refractory squamous non-small cell lung cancer
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. It is the leading cause of cancer death among both men and women. The American Cancer Society estimates that over 224,000 new cases of lung cancer will be diagnosed in the United States in 2014 and over 159,000 will die of the disease. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 25% are Squamous cell carcinomas, 40% are Adenocarcinomas and 10% are Large cell carcinomas. With a better understanding of the Immune checkpoints, the gates are now wide open for the development of various immunotherapies. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent related to their ability to escape immune surveillance by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. Checkmate -063 is a Phase II single arm, open label study designed to evaluate the efficacy of OPDIVO® (Nivolumab) in patients with advanced NSCLC with squamous histology, who had progressed on platinum based therapy as well as at least one additional systemic therapy. OPDIVO® is an immune checkpoint PD-1 (Programmed cell Death 1) targeted, fully human, immunoglobulin G4 monoclonal antibody, which demonstrated an objective response in 20% – 25% of patients with advanced Non Small Cell Lung Cancer, Melanoma and Renal Cell Carcinoma, with favorable toxicities, in previously published studies. This study enrolled 117 patients and two thirds of the patients had previously failed 3 or more treatments and three fourths of patients were within 3 months of completion of their most recent therapy. OPDIVO® was administered as a single agent at 3mg/kg by intravenous infusion every two weeks until disease progression or treatment discontinuation. The primary endpoint was Objective Response Rate (ORR) and exploratory endpoints were overall survival (OS), Progression Free Survival (PFS) and efficacy, based on PD-L1 expression status. With 11 months of minimum follow up, the Objective Response Rate (ORR) was 15% as assessed by an independent review committee and the median duration of response was not reached. These responses were independent of PD-L1 status for patients with quantifiable PD-L1 expression. The estimated one-year survival rate was 41% and median Overall Survival was 8.2 months. The authors noted that an additional 26% of patients had stable disease for a median duration of 6 months, resulting in a disease control rate (ORR+stable disease) of 41%. Approximately 17% of the patients experienced grade 3-4 adverse events which included fatigue, pneumonitis and diarrhea. The authors concluded that the high response rates, median duration of response and disease control rates for Squamous NSCLC, is very promising in this difficult to treat group of patients and phase III trials are underway evaluating OPDIVO® monotherapy in frontline and previously treated patients with Non Small Cell Lung cancer. Ramalingam SS, Mazieres J, Planchard D, et al. Presented at: 2014 Multidisciplinary Symposium in Thoracic Oncology; October 30-November 1, 2014; Chicago, IL. LBA#3462
Statin Use After Colorectal Cancer Diagnosis and Survival A Population-Based Cohort Study
SUMMARY: Approximately 32 million Americans take a statin in the United States. Statins (3-Hydroxy-3-MethylGlutaryl coenzyme A reductase inhibitors) are usually prescribed to lower LDL cholesterol. Cholesterol is a structural component of cell membranes and a reduction in the availability of cholesterol can result in decreased proliferation and migration of cancer cells. The six statin drugs available in the United States include LIPITOR® (Atorvastatin), ZOCOR® (Simvastatin), CRESTOR® (Rosuvastatin), MEVACOR® (Lovastatin), PRAVACHOL® (Pravastatin) and LESCOL® (Fluvastatin). 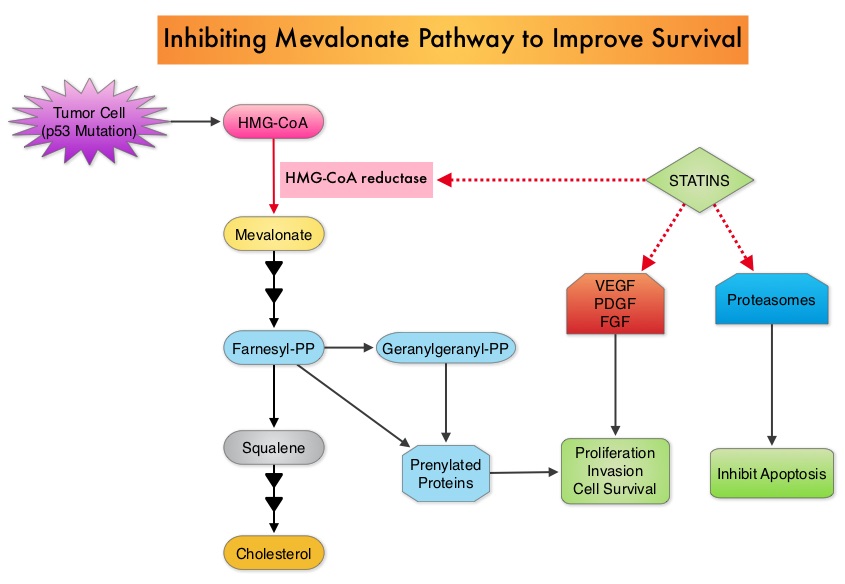 Statin use in cancer patients has been associated with a reduction in cancer related mortality in several clinical studies. This benefit has been attributed to the inhibition of HMG-CoA reductase, which is a rate limiting enzyme in the mevalonate and cholesterol synthesis pathway. The mevalonate pathway is upregulated by mutated p53 (tumor suppressor gene) which is often expressed in cancer cells. By inhibiting the mevalonate pathway, statins can reduce isoprenoid levels such as farnesylpyrophosphate (F-PP) and geranylgeranylpyrophosphate (GG-PP). These isoprenoids are essential for the posttranslational modification of several proteins involved in important intracellular signaling pathways and therefore play a crucial role in cell growth, proliferation, survival and migration. Statins also inhibit angiogenic pathways and proteasomes, thereby negatively impacting cell proliferation and survival. Survival benefit with statin use after colorectal cancer diagnosis has been unclear. To answer this question, the authors identified a cohort of patients (N=7657) diagnosed with stage I to III colorectal cancer from 1998 to 2009, in the National Cancer Data Repository (English Cancer Registry). Information on statin use was obtained from medical records of patients and in this cohort of patients 35% were identified to have used statin drugs following diagnosis of colorectal cancer. Twenty percent of these patients had stage I disease, 43% had stage II disease and 37% had stage III disease. Patients were followed up for 14 years following their diagnosis of colorectal cancer. Statin use after a diagnosis of colorectal cancer was associated with a 29% reduction in colorectal cancer-specific mortality (HR= 0.71). There was a dose-response association with a 36% reduction in colorectal cancer-specific mortality with statin use for more than 1 year (HR=0.64). Statin users after colorectal cancer diagnosis also had a 25% reduction in all-cause mortality (HR=0.75). The authors concluded that based on this large population based colorectal cancer cohort, statin use following diagnosis of colorectal cancer was associated with longer rates of survival. Cardwell CR, Hicks BM, Hughes C, et al. J Clin Oncol 2014;32:3177-3183
Statin use in cancer patients has been associated with a reduction in cancer related mortality in several clinical studies. This benefit has been attributed to the inhibition of HMG-CoA reductase, which is a rate limiting enzyme in the mevalonate and cholesterol synthesis pathway. The mevalonate pathway is upregulated by mutated p53 (tumor suppressor gene) which is often expressed in cancer cells. By inhibiting the mevalonate pathway, statins can reduce isoprenoid levels such as farnesylpyrophosphate (F-PP) and geranylgeranylpyrophosphate (GG-PP). These isoprenoids are essential for the posttranslational modification of several proteins involved in important intracellular signaling pathways and therefore play a crucial role in cell growth, proliferation, survival and migration. Statins also inhibit angiogenic pathways and proteasomes, thereby negatively impacting cell proliferation and survival. Survival benefit with statin use after colorectal cancer diagnosis has been unclear. To answer this question, the authors identified a cohort of patients (N=7657) diagnosed with stage I to III colorectal cancer from 1998 to 2009, in the National Cancer Data Repository (English Cancer Registry). Information on statin use was obtained from medical records of patients and in this cohort of patients 35% were identified to have used statin drugs following diagnosis of colorectal cancer. Twenty percent of these patients had stage I disease, 43% had stage II disease and 37% had stage III disease. Patients were followed up for 14 years following their diagnosis of colorectal cancer. Statin use after a diagnosis of colorectal cancer was associated with a 29% reduction in colorectal cancer-specific mortality (HR= 0.71). There was a dose-response association with a 36% reduction in colorectal cancer-specific mortality with statin use for more than 1 year (HR=0.64). Statin users after colorectal cancer diagnosis also had a 25% reduction in all-cause mortality (HR=0.75). The authors concluded that based on this large population based colorectal cancer cohort, statin use following diagnosis of colorectal cancer was associated with longer rates of survival. Cardwell CR, Hicks BM, Hughes C, et al. J Clin Oncol 2014;32:3177-3183
Cancer of Unknown Primary Site
SUMMARY:Carcinoma of Unknown Primary Site (CUPS) is a heterogeneous clinical pathologic syndrome for which the anatomical site of origin of the primary tumor is clinically undetectable. CUPS accounts for approximately 2% of all advanced malignances annually. The American Cancer Society estimates that about 31,430 cases of Cancer of Unknown Primary site will be diagnosed in 2014 in the United States. The pathobiology of tumors from unknown primary sites is similar to those with detectable primary tumors and therefore may respond to therapies similar to those with easily detectable primary tumors. Historically, the treatment approach for patients with CUPS included broad spectrum empiric chemotherapy. Histological evaluation of the biopsy tissue alone has been the standard practice for decades. With the availability of gene expression profiling assays and advances in ImmunoHistoChemistry staining as well as imaging technology, predicting the tissue of origin of the primary tumor and tailoring therapy accordingly, has improved overall survival in this patient population.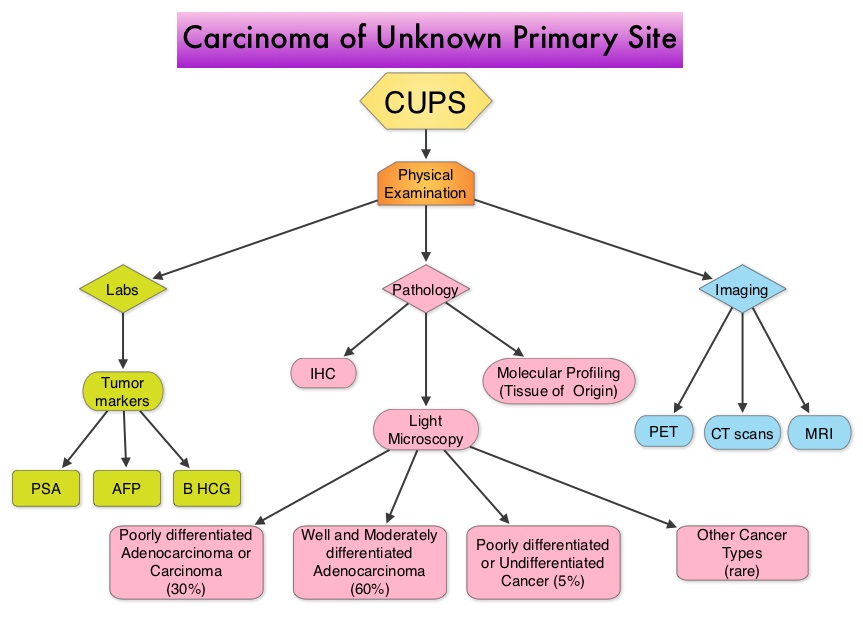 Evaluation of a patient with CUPS starts with gathering and incorporating medical information which includes the patient’s gender, medical history, clinical findings and sites of metastases. A CT scan of the chest, abdomen and pelvis with IV and oral contrast is recommended, although PET (Positron Emission Tomography) or an MRI can be performed in those with renal insufficiency or iodine allergy. PET scan is recommended for those with cervical lymphadenopathy with squamous histology, to help determine the extent of the disease and treatment planning for radiation. PET imaging is also helpful for patients with solitary metastases before locoregional therapies are planned, as well as assessing response in patients with predominantly bone only disease. In women presenting with isolated axillary lymphadenopathy, adenocarcinoma histology, negative mammograms and ultrasound, MRI of the breasts is indicated. With the exception of those patients with CUPS who present with cervical lymphadenopathy, diagnostic procedures such as bronchoscopy, EGD and colonoscopy are not recommended in asymptomatic patients. Tumor markers in general do not have diagnostic value in patients with CUPS although they could be utilized to monitor response to treatment. However, PSA when elevated in a male with adenocarcinoma and osteoblastic metastases, is suggestive of a prostate primary. Similarly an elevated Beta HCG and AFP in a patient with undifferentiated or poorly differentiated carcinoma, is suggestive of an extragonadal germ cell tumor and an elevated AFP is also helpful in making a diagnosis of Hepatoma. Approximately 60% of the patients with CUPS have well or moderately differentiated adenocarcinoma on light microscopy, 30% have poorly differentiated carcinoma or adenocarcinoma, 5% have poorly differentiated or undifferentiated malignancy and 5% have squamous cell carcinoma. Following histological evaluation on light microscopy, the biopsy specimen is further tested using ImmunoHistoChemical stains, using peroxidase labeled antibodies against tumor specific antigens, taking advantage of the similarities in the tumor profiles of primary and metastatic malignancies. After delineating a tumor as carcinoma, lymphoma, sarcoma or melanoma, additional IHC testing can help identify tumors such as a lung primary (postive Thyroid Transcription Factor 1-TTF1and positive CytoKeratin 7- CK7), lower gastrointestinal cancers (positive CK20, positive CDX2 and negative CK7) or a breast primary (positive CK7 and positive Mammaglobin). Tissue-of-Origin molecular profiling is based on the principle that in patients with CUPS, molecular signatures of metastatic tumors are similar to their primary tumor. Tissue-of-Origin molecular profiling is performed using tools such as DNA microarray, quantitative real time polymerase chain reaction assay (rt-PCR) or assays based on messenger RNA (mRNA) or microRNA. These tests are cost-effective and 70% – 90% accurate. This study can be performed on formalin-fixed samples as well as samples from fine needle aspiration. Even though platinum based chemotherapy has been the default regimen for patients with CUPS, histological evaluation of biopsy tissue by light microscopy, IHC testing and molecular profiling assay may complement each other and help guide the Health Care Provider to select site specific therapy. The survival outcomes of CUPS patients with a Tissue-of-Origin molecularly diagnosed profile are comparable to those with similar type advanced cancer with a known primary. The authors concluded that with additional molecular insights into tumor biology and availability of newer therapeutic agents, patients with CUPS and known primary tumors may eventually be treated alike. Varadhachary, GR and Raber, MN. N Engl J Med 2014; 371:757-765
Evaluation of a patient with CUPS starts with gathering and incorporating medical information which includes the patient’s gender, medical history, clinical findings and sites of metastases. A CT scan of the chest, abdomen and pelvis with IV and oral contrast is recommended, although PET (Positron Emission Tomography) or an MRI can be performed in those with renal insufficiency or iodine allergy. PET scan is recommended for those with cervical lymphadenopathy with squamous histology, to help determine the extent of the disease and treatment planning for radiation. PET imaging is also helpful for patients with solitary metastases before locoregional therapies are planned, as well as assessing response in patients with predominantly bone only disease. In women presenting with isolated axillary lymphadenopathy, adenocarcinoma histology, negative mammograms and ultrasound, MRI of the breasts is indicated. With the exception of those patients with CUPS who present with cervical lymphadenopathy, diagnostic procedures such as bronchoscopy, EGD and colonoscopy are not recommended in asymptomatic patients. Tumor markers in general do not have diagnostic value in patients with CUPS although they could be utilized to monitor response to treatment. However, PSA when elevated in a male with adenocarcinoma and osteoblastic metastases, is suggestive of a prostate primary. Similarly an elevated Beta HCG and AFP in a patient with undifferentiated or poorly differentiated carcinoma, is suggestive of an extragonadal germ cell tumor and an elevated AFP is also helpful in making a diagnosis of Hepatoma. Approximately 60% of the patients with CUPS have well or moderately differentiated adenocarcinoma on light microscopy, 30% have poorly differentiated carcinoma or adenocarcinoma, 5% have poorly differentiated or undifferentiated malignancy and 5% have squamous cell carcinoma. Following histological evaluation on light microscopy, the biopsy specimen is further tested using ImmunoHistoChemical stains, using peroxidase labeled antibodies against tumor specific antigens, taking advantage of the similarities in the tumor profiles of primary and metastatic malignancies. After delineating a tumor as carcinoma, lymphoma, sarcoma or melanoma, additional IHC testing can help identify tumors such as a lung primary (postive Thyroid Transcription Factor 1-TTF1and positive CytoKeratin 7- CK7), lower gastrointestinal cancers (positive CK20, positive CDX2 and negative CK7) or a breast primary (positive CK7 and positive Mammaglobin). Tissue-of-Origin molecular profiling is based on the principle that in patients with CUPS, molecular signatures of metastatic tumors are similar to their primary tumor. Tissue-of-Origin molecular profiling is performed using tools such as DNA microarray, quantitative real time polymerase chain reaction assay (rt-PCR) or assays based on messenger RNA (mRNA) or microRNA. These tests are cost-effective and 70% – 90% accurate. This study can be performed on formalin-fixed samples as well as samples from fine needle aspiration. Even though platinum based chemotherapy has been the default regimen for patients with CUPS, histological evaluation of biopsy tissue by light microscopy, IHC testing and molecular profiling assay may complement each other and help guide the Health Care Provider to select site specific therapy. The survival outcomes of CUPS patients with a Tissue-of-Origin molecularly diagnosed profile are comparable to those with similar type advanced cancer with a known primary. The authors concluded that with additional molecular insights into tumor biology and availability of newer therapeutic agents, patients with CUPS and known primary tumors may eventually be treated alike. Varadhachary, GR and Raber, MN. N Engl J Med 2014; 371:757-765
Clinical and Safety Outcomes Associated With Treatment of Acute Venous Thromboembolism A Systematic Review and Meta-analysis
SUMMARY: The Center for Disease Control and Prevention (CDC) estimates that approximately 1-2 per 1000 individuals develop Deep Vein Thrombosis/Pulmonary Embolism (PE) each year in the United States, resulting in 60,000 – 100,000 deaths. VTE is the third leading cause of cardiovascular mortality with a mortality rate of up to 25% in those with untreated acute pulmonary embolism. For decades, Unfractionated Heparin (UFH) also known as standard heparin along with Vitamin K antagonist (Warfarin) has been the established standard, for the treatment of Acute Venous ThromboEmbolism. 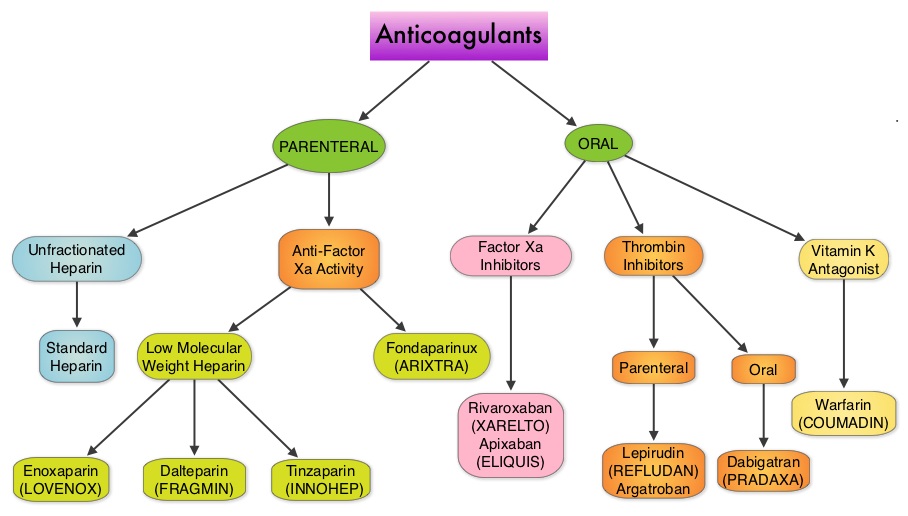 Even though Low Molecular Weight Heparin (LMWH) preparations as well as new oral anticoagulants have been available for the treatment Venous ThromboEmbolism, there has been very little guidance for Health Care Providers on the use of these newer agents. The authors in this analysis compared the efficacy and safety outcomes associated with different anticoagulation regimens for treatment of Venous ThromboEmbolism (VTE). These anticoagulant regimens included Unfractionated Heparin (UFH), Low Molecular Weight Heparin (LMWH) or Fondaparinux in combination with Vitamin K antagonists, LMWH with Dabigatran (PRADAXA®), Rivaroxaban (XARELTO®), Apixaban (ELIQUIS®) or Edoxaban and LMWH alone. This meta analysis included 44,989 patients from 45 randomized trials which reported rates of recurrent VTE and major bleeding in patients with acute VTE. In these Acute Deep Vein Thrombosis and Pulmonary Embolism trials, Rivaroxaban and Apixaban were evaluated without the use of initial LMWH whereas both Dabigatran or Edoxaban were assessed following an initial 5 day treatment with LMWH. This analysis was therefore able to assess clinical and safety outcomes associated with different anticoagulation regimens. The followings findings were noted:
Even though Low Molecular Weight Heparin (LMWH) preparations as well as new oral anticoagulants have been available for the treatment Venous ThromboEmbolism, there has been very little guidance for Health Care Providers on the use of these newer agents. The authors in this analysis compared the efficacy and safety outcomes associated with different anticoagulation regimens for treatment of Venous ThromboEmbolism (VTE). These anticoagulant regimens included Unfractionated Heparin (UFH), Low Molecular Weight Heparin (LMWH) or Fondaparinux in combination with Vitamin K antagonists, LMWH with Dabigatran (PRADAXA®), Rivaroxaban (XARELTO®), Apixaban (ELIQUIS®) or Edoxaban and LMWH alone. This meta analysis included 44,989 patients from 45 randomized trials which reported rates of recurrent VTE and major bleeding in patients with acute VTE. In these Acute Deep Vein Thrombosis and Pulmonary Embolism trials, Rivaroxaban and Apixaban were evaluated without the use of initial LMWH whereas both Dabigatran or Edoxaban were assessed following an initial 5 day treatment with LMWH. This analysis was therefore able to assess clinical and safety outcomes associated with different anticoagulation regimens. The followings findings were noted:
1) Standard Heparin–Vitamin K antagonist combination was associated with an increased risk of recurrent VTE compared with the LMWH–Vitamin K antagonist combination
2) Both new oral anticoagulants and LMWH–vitamin K antagonist combination had similar clinical outcomes. However, the newer oral anticoagulants were associated with a lower risk of major bleeding and this benefit was more pronounced with Rivaroxaban and Apixaban. Compared with LMWH-Dabigatran and LMWH-Edoxaban combinations, Apixaban was associated with a lower risk of bleeding.
This comprehensive analysis lead the authors to conclude that Unfractionated Heparin (Standard Heparin)–Vitamin K antagonist combination is the least effective strategy for the treatment of Acute Venous ThromboEmbolism and Rivaroxaban and Apixaban are associated with the lowest risk for bleeding. Castellucci LA, Cameron C, Le Gal G, et al. JAMA 2014;312:1122-1135
Phase 3 study of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting during repeated moderately emetogenic chemotherapy (MEC) cycles
SUMMARY: Chemotherapy Induced Nausea and Vomiting (CINV) is one of the most common adverse effects of chemotherapy and is experienced by about 80% of patients receiving chemotherapy. The development of effective antiemetic agents has facilitated the administration of majority of the chemotherapy agents in an outpatient setting avoiding hospitalization.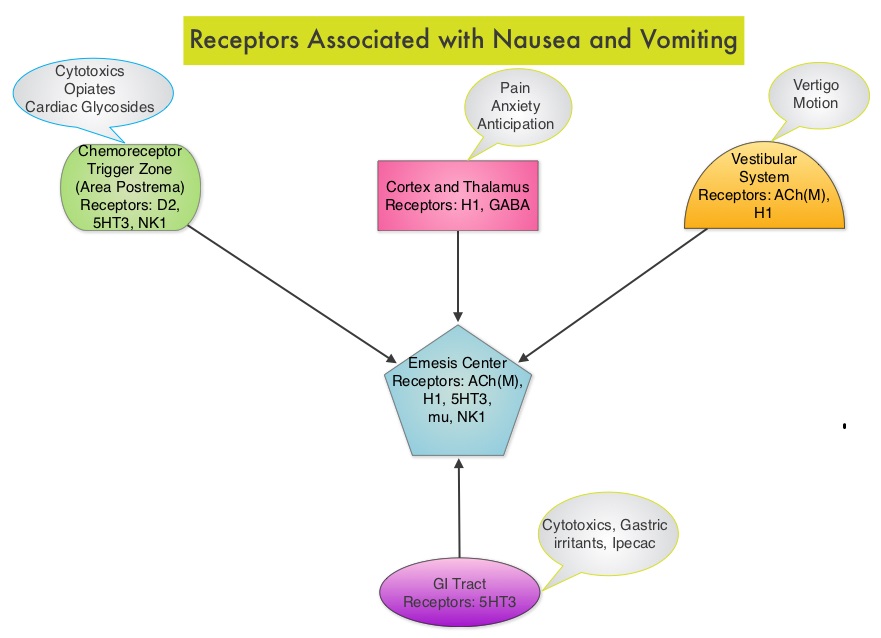 Acute CINV begins within the first 24 hours following chemotherapy administration, with most patients experiencing symptoms within the first four hours of treatment whereas delayed nausea and vomiting occurs more than 24 hours after chemotherapy administration and can persist for several days. Delayed CINV is often underestimated and a third of the patients receiving chemotherapy may experience delayed nausea and vomiting without prior acute nausea or vomiting. Acute nausea and vomiting is dependent on serotonin (5-hydroxytryptamine-5HT3) and its receptors. 5-HT3 receptors are located on vagal afferent pathway, which in turn activates the vomiting center to initiate the vomiting reflex. 5-HT3 receptors are located peripherally on the nerve endings of the vagus and centrally in the Chemoreceptor Trigger Zone of the area Postrema. Chemotherapeutic agents produce nausea and vomiting by stimulating the release of serotonin from the enterochromaffin cells of the small intestine. Delayed nausea and vomiting is associated with the activation of Neurokinin 1 (NK1) receptors by substance P. NK1 receptors are broadly distributed in the central and peripheral nervous systems. Netupitant inhibits substance P mediated responses. ALOXI® (Palonosetron) is a second generation 5-HT3 antagonist and has a 100 fold higher binding affinity to 5-HT3 receptor than other 5-HT3 receptor antagonists. AKYNZEO® (300 mg Netupitant/0.5 mg Palonosetron) is an oral, fixed combination product of Netupitant, a substance P/Neurokinin 1 (NK1) receptor antagonist, and ALOXI®, a serotonin (5- HT3) receptor antagonist.
Acute CINV begins within the first 24 hours following chemotherapy administration, with most patients experiencing symptoms within the first four hours of treatment whereas delayed nausea and vomiting occurs more than 24 hours after chemotherapy administration and can persist for several days. Delayed CINV is often underestimated and a third of the patients receiving chemotherapy may experience delayed nausea and vomiting without prior acute nausea or vomiting. Acute nausea and vomiting is dependent on serotonin (5-hydroxytryptamine-5HT3) and its receptors. 5-HT3 receptors are located on vagal afferent pathway, which in turn activates the vomiting center to initiate the vomiting reflex. 5-HT3 receptors are located peripherally on the nerve endings of the vagus and centrally in the Chemoreceptor Trigger Zone of the area Postrema. Chemotherapeutic agents produce nausea and vomiting by stimulating the release of serotonin from the enterochromaffin cells of the small intestine. Delayed nausea and vomiting is associated with the activation of Neurokinin 1 (NK1) receptors by substance P. NK1 receptors are broadly distributed in the central and peripheral nervous systems. Netupitant inhibits substance P mediated responses. ALOXI® (Palonosetron) is a second generation 5-HT3 antagonist and has a 100 fold higher binding affinity to 5-HT3 receptor than other 5-HT3 receptor antagonists. AKYNZEO® (300 mg Netupitant/0.5 mg Palonosetron) is an oral, fixed combination product of Netupitant, a substance P/Neurokinin 1 (NK1) receptor antagonist, and ALOXI®, a serotonin (5- HT3) receptor antagonist. 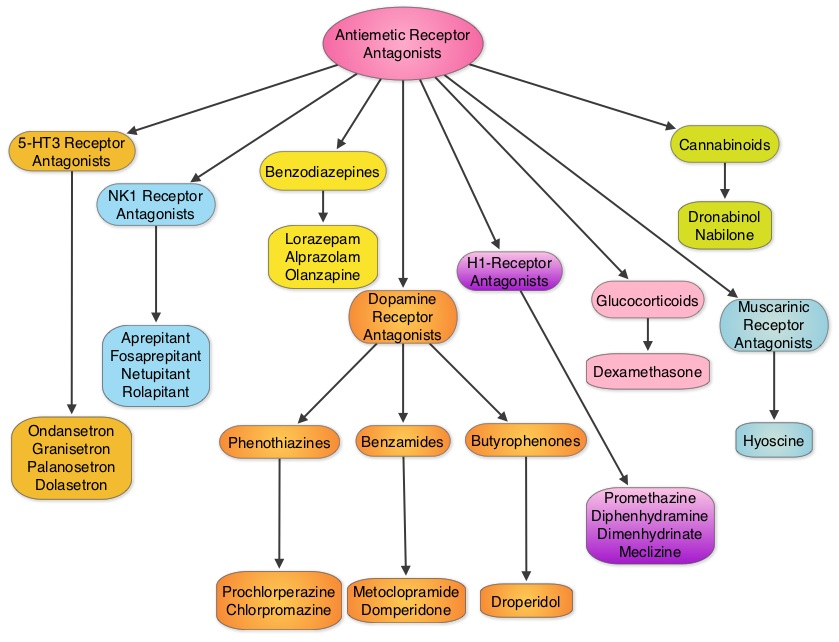 Taking advantage of the different mechanisms of action and synergy between these two agents, a randomized, double-blind, multinational study was conducted, comparing AKYNZEO® with ALOXI® in chemotherapy naive patients receiving anthracycline based chemotherapy regimens. One thousand four hundred and fifty five (N=1455) were randomized to receive either AKYNZEO® or ALOXI® and both groups received oral Dexamethasone as a part of their antiemetic regimen. The primary endpoint was complete response (CR) defined as no emesis, no rescue medication needed and no significant nausea. AKYNZEO® maintained superiority over ALOXI® for overall (0-120 hours) complete response and also maintained superiority over multiple chemotherapy cycles (P < 0.0001). The most common side effects for AKYNZEO® were headache, fatigue and constipation. The authors concluded that AKYNZEO®, by targeting dual antiemetic pathways, significantly improved chemotherapy induced nausea and vomiting compared to ALOXI® alone and this benefit was maintained over multiple cycles of moderately emetogenic chemotherapy. AKYNZEO® capsule can be administered as a single dose, one hour prior to the start of chemotherapy. Aapro MS, Karthaus M, Schwartzberg LS, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 9502)</s
Taking advantage of the different mechanisms of action and synergy between these two agents, a randomized, double-blind, multinational study was conducted, comparing AKYNZEO® with ALOXI® in chemotherapy naive patients receiving anthracycline based chemotherapy regimens. One thousand four hundred and fifty five (N=1455) were randomized to receive either AKYNZEO® or ALOXI® and both groups received oral Dexamethasone as a part of their antiemetic regimen. The primary endpoint was complete response (CR) defined as no emesis, no rescue medication needed and no significant nausea. AKYNZEO® maintained superiority over ALOXI® for overall (0-120 hours) complete response and also maintained superiority over multiple chemotherapy cycles (P < 0.0001). The most common side effects for AKYNZEO® were headache, fatigue and constipation. The authors concluded that AKYNZEO®, by targeting dual antiemetic pathways, significantly improved chemotherapy induced nausea and vomiting compared to ALOXI® alone and this benefit was maintained over multiple cycles of moderately emetogenic chemotherapy. AKYNZEO® capsule can be administered as a single dose, one hour prior to the start of chemotherapy. Aapro MS, Karthaus M, Schwartzberg LS, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 9502)</s
Phase 3 study of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting during repeated moderately emetogenic chemotherapy (MEC) cycles
SUMMARY: Chemotherapy Induced Nausea and Vomiting (CINV) is one of the most common adverse effects of chemotherapy and is experienced by about 80% of patients receiving chemotherapy. The development of effective antiemetic agents has facilitated the administration of majority of the chemotherapy agents in an outpatient setting avoiding hospitalization. Acute CINV begins within the first 24 hours following chemotherapy administration, with most patients experiencing symptoms within the first four hours of treatment whereas delayed nausea and vomiting occurs more than 24 hours after chemotherapy administration and can persist for several days. Delayed CINV is often underestimated and a third of the patients receiving chemotherapy may experience delayed nausea and vomiting without prior acute nausea or vomiting. Acute nausea and vomiting is dependent on serotonin (5-hydroxytryptamine-5HT3) and its receptors. 5-HT3 receptors are located on vagal afferent pathway, which in turn activates the vomiting center to initiate the vomiting reflex. 5-HT3 receptors are located peripherally on the nerve endings of the vagus and centrally in the Chemoreceptor Trigger Zone of the area Postrema. Chemotherapeutic agents produce nausea and vomiting by stimulating the release of serotonin from the enterochromaffin cells of the small intestine. Delayed nausea and vomiting is associated with the activation of Neurokinin 1 (NK1) receptors by substance P. NK1 receptors are broadly distributed in the central and peripheral nervous systems. Netupitant inhibits substance P mediated responses. ALOXI® (Palonosetron) is a second generation 5-HT3 antagonist and has a 100 fold higher binding affinity to 5-HT3 receptor than other 5-HT3 receptor antagonists. AKYNZEO® (300 mg Netupitant/0.5 mg Palonosetron) is an oral, fixed combination product of Netupitant, a substance P/Neurokinin 1 (NK1) receptor antagonist, and ALOXI®, a serotonin (5- HT3) receptor antagonist. Taking advantage of the different mechanisms of action and synergy between these two agents, a randomized, double-blind, multinational study was conducted, comparing AKYNZEO® with ALOXI® in chemotherapy naive patients receiving anthracycline based chemotherapy regimens. One thousand four hundred and fifty five (N=1455) were randomized to receive either AKYNZEO® or ALOXI® and both groups received oral Dexamethasone as a part of their antiemetic regimen. The primary endpoint was complete response (CR) defined as no emesis, no rescue medication needed and no significant nausea. AKYNZEO® maintained superiority over ALOXI® for overall (0-120 hours) complete response and also maintained superiority over multiple chemotherapy cycles (P < 0.0001). The most common side effects for AKYNZEO® were headache, fatigue and constipation. The authors concluded that AKYNZEO®, by targeting dual antiemetic pathways, significantly improved chemotherapy induced nausea and vomiting compared to ALOXI® alone and this benefit was maintained over multiple cycles of moderately emetogenic chemotherapy. AKYNZEO® capsule can be administered as a single dose, one hour prior to the start of chemotherapy. Aapro MS, Karthaus M, Schwartzberg LS, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 9502)</s
AR-V7 and Resistance to Enzalutamide and Abiraterone in Prostate Cancer
SUMMARY: Prostate cancer is the most common cancer in American men excluding skin cancer and 1 in 7 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, over 230,000 new cases of prostate cancer will be diagnosed in 2014 and close to 30,000 men will die of the disease. Prostate cancer is driven by Androgen Receptor (AR) and its signaling pathways. Initial treatment strategies for patients with metastatic prostate cancer include lowering the levels of circulating androgens with medical or surgical castration or blocking the binding of androgens to the androgen receptor. 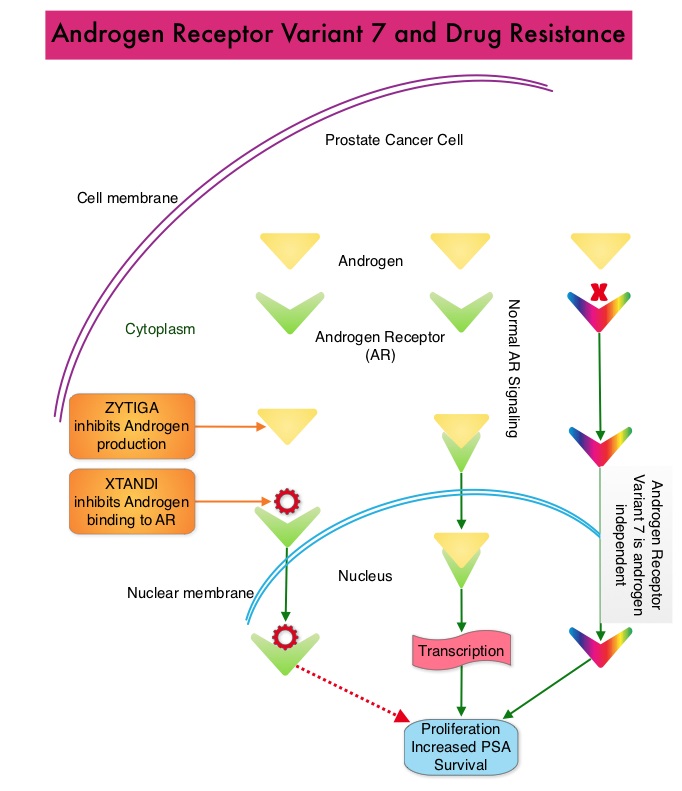 Upon progression {described as Castrate Resistant Prostate Cancer (CRPC), as these tumors are not androgen independent and continue to rely on Androgen Receptor signaling} two agents are presently available for metastatic CRPC. They include ZYTIGA® (Abiraterone) and XTANDI® (Enzalutamide). Both these agents have been shown to improve survival in metastatic CRPC. ZYTIGA® inhibits CYP 17A1 enzyme and depletes adrenal and intratumoral androgens, thereby impairing AR signaling. XTANDI® competes with Testosterone and Dihydrotestosterone and avidly binds to the Androgen Receptor, thereby inhibiting AR signaling and in addition inhibits translocation of the AR into the nucleus and thus inhibits the transcriptional activities of the AR. About 20-40% of the patients do not respond to these newer agents and even those who respond will invariably develop resistance to these drugs. This again has been attributed to persistent AR signaling by variant forms of Androgen Receptor, generated through somatic mutation or aberrant RNA splicing. Androgen Receptor Variant AR-V7 can be detected in the circulating tumor cells. AR-V7 does not have the domain to bind androgens and may be associated with resistance to XTANDI®. Further AR-V7 is constitutively active and can independently activate transcription factors and therefore is not effected by androgen depleting agents including ZYTIGA®. With this background, the authors hypothesized that detection of Androgen Receptor variant AR-V7 in circulating tumor cells from men with metastatic prostate cancer would be associated with resistance to both ZYTIGA® and XTANDI®. In this prospective study which enrolled patients with Castrate Resistant Prostate Cancer (CRPC), 31 patients received treatment with ZYTIGA® and 31 patients received treatment with XTANDI®. Levels of AR-V7 in circulating tumor cells of these patients were analyzed using quantitative Reverse Transcriptase – Polymerase Chain Reaction assay. The primary endpoint was association between AR-V7 status (positive versus negative) and Prostate Specific Antigen (PSA) response rates and secondary endpoints included freedom from PSA progression (PSA Progression Free Survival), clinical or radiographic Progression Free Survival, and Overall Survival. The authors noted that patients with detectable AR-V7 in circulating tumor cells had no response to ZYTIGA® or XTANDI® as measured by serum PSA level reduction of 50% or more and also had a shorter Progression Free Survival and Overall Survival. Also of interest, the prevalence of detectable AR-V7 in circulating tumor cells before treatment with ZYTIGA® and XTANDI® was 9-15% whereas it increased to approximately 50% after disease progressed during treatment with either of these two drugs. This suggested a common mechanism of resistance to both drugs. The authors concluded that detection of AR-V7 in circulating tumor cells from patients with Castration Resistant Prostate Cancer, may be associated with resistance to ZYTIGA® and XTANDI® and if further validated, could be used as a biomarker. Antonarakis ES, Lu C, Wang H, et al. N Engl J Med 2014; 371:1028-1038
Upon progression {described as Castrate Resistant Prostate Cancer (CRPC), as these tumors are not androgen independent and continue to rely on Androgen Receptor signaling} two agents are presently available for metastatic CRPC. They include ZYTIGA® (Abiraterone) and XTANDI® (Enzalutamide). Both these agents have been shown to improve survival in metastatic CRPC. ZYTIGA® inhibits CYP 17A1 enzyme and depletes adrenal and intratumoral androgens, thereby impairing AR signaling. XTANDI® competes with Testosterone and Dihydrotestosterone and avidly binds to the Androgen Receptor, thereby inhibiting AR signaling and in addition inhibits translocation of the AR into the nucleus and thus inhibits the transcriptional activities of the AR. About 20-40% of the patients do not respond to these newer agents and even those who respond will invariably develop resistance to these drugs. This again has been attributed to persistent AR signaling by variant forms of Androgen Receptor, generated through somatic mutation or aberrant RNA splicing. Androgen Receptor Variant AR-V7 can be detected in the circulating tumor cells. AR-V7 does not have the domain to bind androgens and may be associated with resistance to XTANDI®. Further AR-V7 is constitutively active and can independently activate transcription factors and therefore is not effected by androgen depleting agents including ZYTIGA®. With this background, the authors hypothesized that detection of Androgen Receptor variant AR-V7 in circulating tumor cells from men with metastatic prostate cancer would be associated with resistance to both ZYTIGA® and XTANDI®. In this prospective study which enrolled patients with Castrate Resistant Prostate Cancer (CRPC), 31 patients received treatment with ZYTIGA® and 31 patients received treatment with XTANDI®. Levels of AR-V7 in circulating tumor cells of these patients were analyzed using quantitative Reverse Transcriptase – Polymerase Chain Reaction assay. The primary endpoint was association between AR-V7 status (positive versus negative) and Prostate Specific Antigen (PSA) response rates and secondary endpoints included freedom from PSA progression (PSA Progression Free Survival), clinical or radiographic Progression Free Survival, and Overall Survival. The authors noted that patients with detectable AR-V7 in circulating tumor cells had no response to ZYTIGA® or XTANDI® as measured by serum PSA level reduction of 50% or more and also had a shorter Progression Free Survival and Overall Survival. Also of interest, the prevalence of detectable AR-V7 in circulating tumor cells before treatment with ZYTIGA® and XTANDI® was 9-15% whereas it increased to approximately 50% after disease progressed during treatment with either of these two drugs. This suggested a common mechanism of resistance to both drugs. The authors concluded that detection of AR-V7 in circulating tumor cells from patients with Castration Resistant Prostate Cancer, may be associated with resistance to ZYTIGA® and XTANDI® and if further validated, could be used as a biomarker. Antonarakis ES, Lu C, Wang H, et al. N Engl J Med 2014; 371:1028-1038
Rituximab Extended Schedule or Re-Treatment Trial for Low–Tumor Burden Follicular Lymphoma Eastern Cooperative Oncology Group Protocol E4402
SUMMARY: Non-Hodgkin Lymphoma (NHL) is one of the most common cancers in the United States and the American Cancer Society estimates that in 2014, about 70,800 people will be diagnosed with NHL in the US and close to 19,000 people will die of the disease. RITUXAN® (Rituximab) is a first generation type I, chimeric anti-CD20 targeted monoclonal antibody that destroys malignant human B cells primarily by complement-dependent cytotoxicity (CDC) and Antibody-Dependent Cell-Mediated Cytotoxicity (ADCC).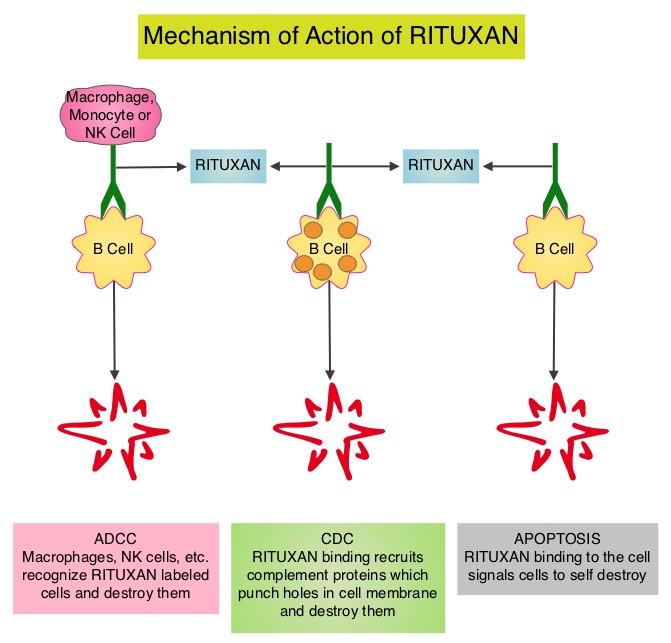 Since its approval in 1997, immunochemotherapy regimens incorporating RITUXAN® has had a major impact in treatment outcomes for patients with Follicular Lymphomas both in first line as well as relapsed settings. Two years of RITUXAN® maintenance therapy after induction immunochemotherapy as first-line treatment for high tumor burden Follicular Lymphoma, significantly improved Progression Free Survival, as was shown in the PRIMA study. Similarly, maintenance RITUXAN® has been shown to improve Progression Free Survival when compared with observation, in patients with low tumor burden Follicular Lymphoma. Whether maintenance RITUXAN® provides superior long term disease control compared with retreatment with RITUXAN® when disease progression is noted, has remained unclear. RESORT [Rituximab Extended Schedule or Re-Treatment Trial] is a randomized trial designed to determine whether maintenance treatment with RITUXAN® provided superior disease control compared with retreatment with RITUXAN® at disease progression, in patients with previously untreated low tumor burden Follicular Lymphoma. Low tumor burden was defined as no mass more than 7 cm, fewer than three masses more than 3 cm, no B symptoms, spleen size less than 16 cm by CT scan, no evidence of organ compromise, circulating lymphocytes less 5,000/μL, and no evidence of cytopenias defined as platelets less than 100,000/μL, hemoglobin less than 10 g/dL, or absolute neutrophil count less than 1,500/μL. Of the 408 patients with Follicular Lymphoma included in this study, 289 patients responded to induction treatment with 4 weekly doses of RITUXAN® given at 375mg/m2. These patients were then randomly assigned to maintenance RITUXAN® (N= 146) or retreatment with RITUXAN® (N=143) at each disease progression, until treatment failure. Maintenance RITUXAN® treatment consisted of a single dose of RITUXAN® given every 3 months until treatment failure. The primary end point of this study was time to treatment failure. Secondary end points included time to first cytotoxic therapy, toxicity, and health-related quality of life (HRQOL). With a median follow-up of 4.5 years, there was no difference in the median time to treatment failure amongst the maintenance RITUXAN® and retreatment RITUXAN® groups (4.3 years vs 3.9 years, P=0.54). The median number of RITUXAN® doses was 18 for those receiving maintenance RITUXAN® compared to 4 for those receiving retreatment RITUXAN®. Grade 3 or 4 toxicities were uncommon in both treatment groups and there was no difference in health-related quality of life. The authors concluded that in low tumor burden Follicular Lymphoma, a retreatment strategy at disease progression utilizes fewer doses of RITUXAN® with outcomes equivalent to that achieved with maintenance RITUXAN®. Kahl BS, Hong F, Williams ME, et al. J Clin Oncol 2014;32:3096-3102
Since its approval in 1997, immunochemotherapy regimens incorporating RITUXAN® has had a major impact in treatment outcomes for patients with Follicular Lymphomas both in first line as well as relapsed settings. Two years of RITUXAN® maintenance therapy after induction immunochemotherapy as first-line treatment for high tumor burden Follicular Lymphoma, significantly improved Progression Free Survival, as was shown in the PRIMA study. Similarly, maintenance RITUXAN® has been shown to improve Progression Free Survival when compared with observation, in patients with low tumor burden Follicular Lymphoma. Whether maintenance RITUXAN® provides superior long term disease control compared with retreatment with RITUXAN® when disease progression is noted, has remained unclear. RESORT [Rituximab Extended Schedule or Re-Treatment Trial] is a randomized trial designed to determine whether maintenance treatment with RITUXAN® provided superior disease control compared with retreatment with RITUXAN® at disease progression, in patients with previously untreated low tumor burden Follicular Lymphoma. Low tumor burden was defined as no mass more than 7 cm, fewer than three masses more than 3 cm, no B symptoms, spleen size less than 16 cm by CT scan, no evidence of organ compromise, circulating lymphocytes less 5,000/μL, and no evidence of cytopenias defined as platelets less than 100,000/μL, hemoglobin less than 10 g/dL, or absolute neutrophil count less than 1,500/μL. Of the 408 patients with Follicular Lymphoma included in this study, 289 patients responded to induction treatment with 4 weekly doses of RITUXAN® given at 375mg/m2. These patients were then randomly assigned to maintenance RITUXAN® (N= 146) or retreatment with RITUXAN® (N=143) at each disease progression, until treatment failure. Maintenance RITUXAN® treatment consisted of a single dose of RITUXAN® given every 3 months until treatment failure. The primary end point of this study was time to treatment failure. Secondary end points included time to first cytotoxic therapy, toxicity, and health-related quality of life (HRQOL). With a median follow-up of 4.5 years, there was no difference in the median time to treatment failure amongst the maintenance RITUXAN® and retreatment RITUXAN® groups (4.3 years vs 3.9 years, P=0.54). The median number of RITUXAN® doses was 18 for those receiving maintenance RITUXAN® compared to 4 for those receiving retreatment RITUXAN®. Grade 3 or 4 toxicities were uncommon in both treatment groups and there was no difference in health-related quality of life. The authors concluded that in low tumor burden Follicular Lymphoma, a retreatment strategy at disease progression utilizes fewer doses of RITUXAN® with outcomes equivalent to that achieved with maintenance RITUXAN®. Kahl BS, Hong F, Williams ME, et al. J Clin Oncol 2014;32:3096-3102