
SUMMARY: Breast cancer is the most common cancer among women in the United States and 1 in 8 women will develop invasive breast cancer during their lifetime. Screening mammography complemented by breast self exam and clinical breast exam has resulted in early detection of breast cancer and successful outcomes. Even though mammography is a sensitive screening test, a small percentage of breast cancers may not show up on mammograms but may be palpable on examination by the patient or the clinician. Further, mammograms are less likely to find breast tumors in younger women with dense breast tissue. A breast Magnetic Resonance Imaging (MRI) is more sensitive than mammography although the specificity of a breast MRI is lower, resulting in a higher rate of false-positive findings and potentially unnecessary biopsies. Microcalcifications in the breast can be missed by a breast MRI. Taking these factors into consideration, appropriate utilization of breast MRI becomes relevant.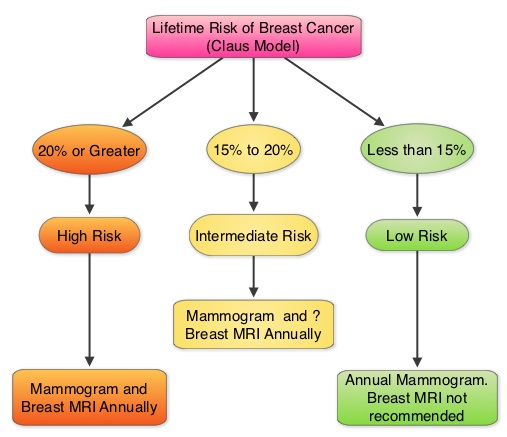
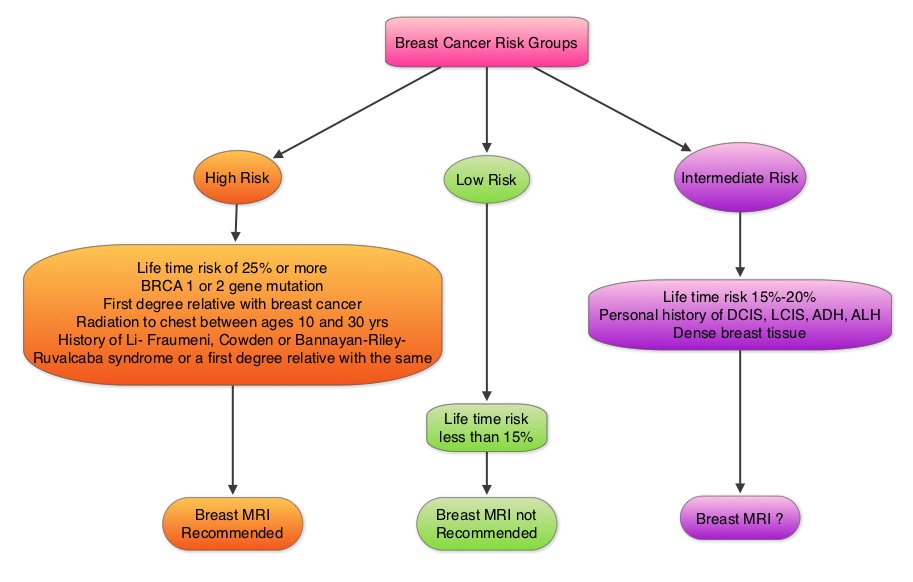
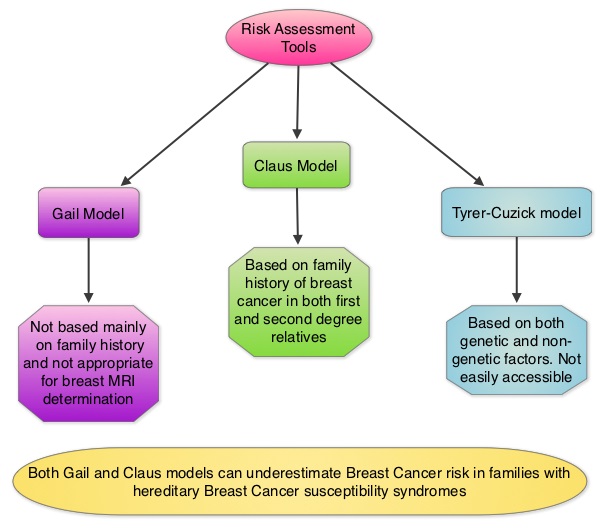 The American Cancer Society (ACS) recommends an annual MRI as an adjunct to screening mammogram and clinical breast exam in certain groups with increased risk of breast cancer (See Figures). The authors conducted this study to determine the utilization of breast (MRI) in community settings. In this retrospective study, the authors reviewed data on 10,518 women from a not-for-profit health plan, and these women had at least one breast MRI between January 2000 and December 2011. The appropriateness of a breast MRI was determined using a prediction model obtained from electronic medical records on a subset of patients. Between 2000 and 2009, there was a 20-fold increase in the use of breast MRI from 6.5 per 10,000 women in the year 2000 to 130.7 per 10,000 in 2009. This increase then declined and stabilized to 104.8 per 10,000 by 2011. With regards to indications for a breast MRI, 51.7% had a family history of breast cancer, 30.1% had a personal history of breast cancer and 3.5% of women had a documented genetic mutation. It is interesting to note that of those who received screening or surveillance breast MRI’s, only 21% fulfilled the American Cancer Society (ACS) criteria for a breast MRI. Conversely, fewer participants (48.4%), with documented deleterious genetic mutations, received breast MRI screening. The authors concluded that breast MRI was over utilized in those who did not fit the ACS criteria and was under utilized in those with documented genetic mutations. It is their opinion that routine breast MRI screening is not recommended for a new breast cancer diagnosis or for breast cancer surveillance and should only be considered for the group of individuals who have the most benefit. Breast MRI is performed preferably between days 7-15 of menstrual cycle for premenopausal women, using a dedicated breast coil, with the ability to perform a biopsy under MRI guidance by experienced radiologists, during the same visit. Stout NK, Nekhlyudov L, Li L, et al. JAMA Intern Med. 2014;174:114-121.
The American Cancer Society (ACS) recommends an annual MRI as an adjunct to screening mammogram and clinical breast exam in certain groups with increased risk of breast cancer (See Figures). The authors conducted this study to determine the utilization of breast (MRI) in community settings. In this retrospective study, the authors reviewed data on 10,518 women from a not-for-profit health plan, and these women had at least one breast MRI between January 2000 and December 2011. The appropriateness of a breast MRI was determined using a prediction model obtained from electronic medical records on a subset of patients. Between 2000 and 2009, there was a 20-fold increase in the use of breast MRI from 6.5 per 10,000 women in the year 2000 to 130.7 per 10,000 in 2009. This increase then declined and stabilized to 104.8 per 10,000 by 2011. With regards to indications for a breast MRI, 51.7% had a family history of breast cancer, 30.1% had a personal history of breast cancer and 3.5% of women had a documented genetic mutation. It is interesting to note that of those who received screening or surveillance breast MRI’s, only 21% fulfilled the American Cancer Society (ACS) criteria for a breast MRI. Conversely, fewer participants (48.4%), with documented deleterious genetic mutations, received breast MRI screening. The authors concluded that breast MRI was over utilized in those who did not fit the ACS criteria and was under utilized in those with documented genetic mutations. It is their opinion that routine breast MRI screening is not recommended for a new breast cancer diagnosis or for breast cancer surveillance and should only be considered for the group of individuals who have the most benefit. Breast MRI is performed preferably between days 7-15 of menstrual cycle for premenopausal women, using a dedicated breast coil, with the ability to perform a biopsy under MRI guidance by experienced radiologists, during the same visit. Stout NK, Nekhlyudov L, Li L, et al. JAMA Intern Med. 2014;174:114-121.
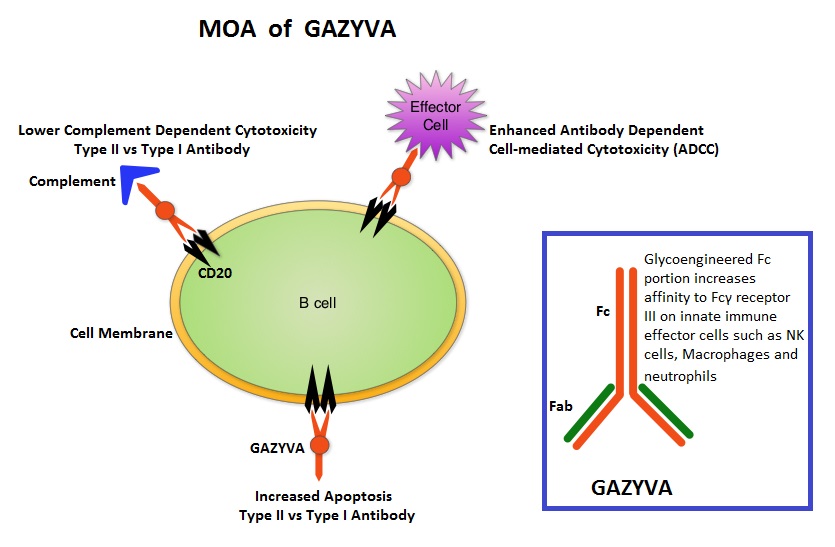 GAZYVA® is glycoengineered, fully humanized, third generation, type II anti-CD20 antibody (IgG1 monoclonal antibody) that selectivity binds to the extracellular domain of the CD20 antigen on malignant human B cells. By virtue of binding affinity of the glycoengineered Fc portion of GAZYVA® to Fcγ receptor III on innate immune effector cells such as natural killer cells, macrophages and neutrophils, antibody-dependent cell-mediated cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis is significantly enhanced, whereas it induces very little complement-dependent cytotoxicity. This is in contrast to RITUXAN® (Rituximab), which is a first generation type I, chimeric anti-CD20 targeted monoclonal antibody that kills CLL cells primarily by complement-dependent cytotoxicity and also ADCC. In this phase III trial, LEUKERAN® (Chlorambucil) was compared with a combination of GAZYVA® plus LEUKERAN® and a combination of RITUXAN® plus LEUKERAN®. Five Hundred and eighty nine (589) treatment naïve CLL patients over 70 years of age with comorbidities were enrolled of whom 118 patients received LEUKERAN® alone, 238 received GAZYVA® plus LEUKERAN® and 233 received RITUXAN® plus LEUKERAN®. The primary endpoint was Progression-Free Survival (PFS). Chemoimmunotherapy with both GAZYVA® plus LEUKERAN® and RITUXAN® plus LEUKERAN® significantly prolonged PFS compared to LEUKERAN® alone. The median PFS was 11.1 months with LEUKERAN® alone compared to 26.7 months for GAZYVA® plus LEUKERAN® (HR=0.18, P<0.001) and 16.3 months for RITUXAN® plus LEUKERAN® (HR=0.44, P<0.001). This benefit was seen in all subgroups except those with del(17) and quality of life in those who received antibody along with LEUKERAN® was not compromised. The combination of GAZYVA® and LEUKERAN®, also prolonged overall survival when compared to LEUKERAN® alone (HR=0.41; P=0.002). This benefit however was not noted with the RITUXAN® plus LEUKERAN® combination. Treatment with GAZYVA® plus LEUKERAN® when compared with RITUXAN® plus LEUKERAN®, resulted in a longer PFS (26.7 vs15.2 months; HR=0.39; P<0.001), higher complete response rates (20.7% vs. 7.0%) and deeper molecular responses. Infusion related reactions were more common in the GAZYVA® plus LEUKERAN® group without increase in the risk for infections. The authors concluded that a combination of GAZYVA® and LEUKERAN® when given to elderly patients with comorbid conditions improved overall survival compared to LEUKERAN® alone and resulted in higher response rates and longer PFS than RITUXAN® plus LEUKERAN®. Goede V, Fischer K, Busch R, et al. N Engl J Med 2014; 370:1101-1110
GAZYVA® is glycoengineered, fully humanized, third generation, type II anti-CD20 antibody (IgG1 monoclonal antibody) that selectivity binds to the extracellular domain of the CD20 antigen on malignant human B cells. By virtue of binding affinity of the glycoengineered Fc portion of GAZYVA® to Fcγ receptor III on innate immune effector cells such as natural killer cells, macrophages and neutrophils, antibody-dependent cell-mediated cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis is significantly enhanced, whereas it induces very little complement-dependent cytotoxicity. This is in contrast to RITUXAN® (Rituximab), which is a first generation type I, chimeric anti-CD20 targeted monoclonal antibody that kills CLL cells primarily by complement-dependent cytotoxicity and also ADCC. In this phase III trial, LEUKERAN® (Chlorambucil) was compared with a combination of GAZYVA® plus LEUKERAN® and a combination of RITUXAN® plus LEUKERAN®. Five Hundred and eighty nine (589) treatment naïve CLL patients over 70 years of age with comorbidities were enrolled of whom 118 patients received LEUKERAN® alone, 238 received GAZYVA® plus LEUKERAN® and 233 received RITUXAN® plus LEUKERAN®. The primary endpoint was Progression-Free Survival (PFS). Chemoimmunotherapy with both GAZYVA® plus LEUKERAN® and RITUXAN® plus LEUKERAN® significantly prolonged PFS compared to LEUKERAN® alone. The median PFS was 11.1 months with LEUKERAN® alone compared to 26.7 months for GAZYVA® plus LEUKERAN® (HR=0.18, P<0.001) and 16.3 months for RITUXAN® plus LEUKERAN® (HR=0.44, P<0.001). This benefit was seen in all subgroups except those with del(17) and quality of life in those who received antibody along with LEUKERAN® was not compromised. The combination of GAZYVA® and LEUKERAN®, also prolonged overall survival when compared to LEUKERAN® alone (HR=0.41; P=0.002). This benefit however was not noted with the RITUXAN® plus LEUKERAN® combination. Treatment with GAZYVA® plus LEUKERAN® when compared with RITUXAN® plus LEUKERAN®, resulted in a longer PFS (26.7 vs15.2 months; HR=0.39; P<0.001), higher complete response rates (20.7% vs. 7.0%) and deeper molecular responses. Infusion related reactions were more common in the GAZYVA® plus LEUKERAN® group without increase in the risk for infections. The authors concluded that a combination of GAZYVA® and LEUKERAN® when given to elderly patients with comorbid conditions improved overall survival compared to LEUKERAN® alone and resulted in higher response rates and longer PFS than RITUXAN® plus LEUKERAN®. Goede V, Fischer K, Busch R, et al. N Engl J Med 2014; 370:1101-1110
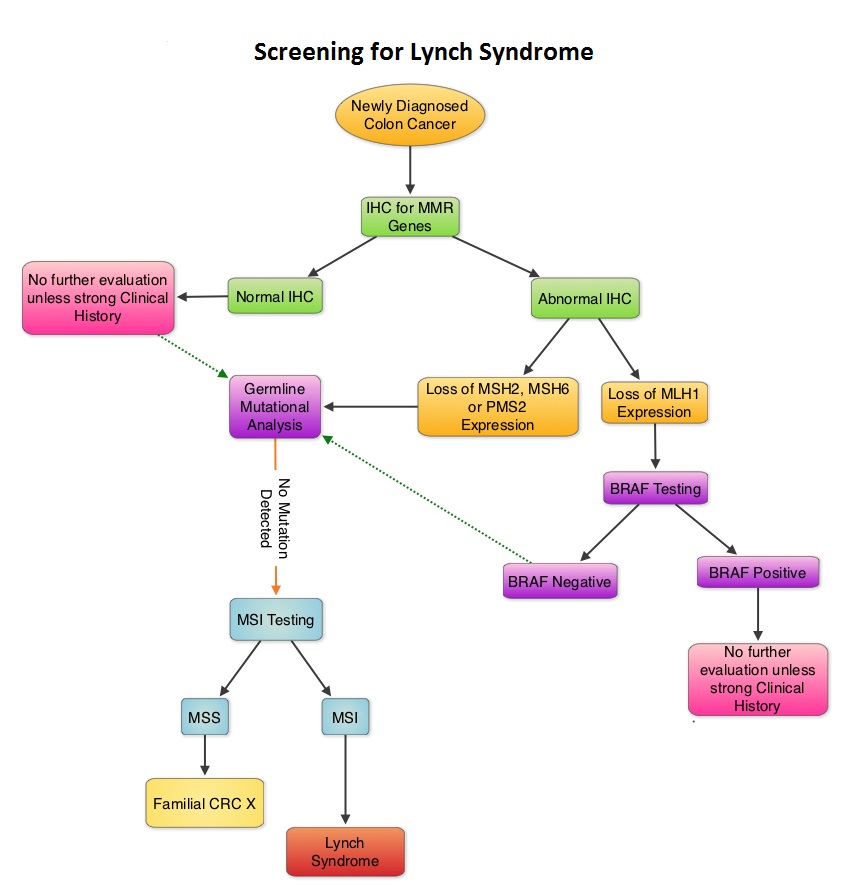 When any of these genes are mutated, repair of DNA replication mistakes is prevented resulting in continuous division of abnormal cells and possibly cancer. The EPCAM gene lies next to the MSH2 gene on chromosome 2 and mutations in the EPCAM gene can cause the MSH2 gene to be inactivated, interrupting DNA repair and leading to accumulation of DNA replication errors and possible malignancy. A Clinical Diagnosis of Lynch Syndrome can be made based on personal and family history if at least three relatives have a malignancy associated with Lynch Syndrome such as colorectal, endometrial, small bowel, ureter or renal pelvis cancer. In addition the following criteria should be met: • One relative must be a first-degree relative of the other two. • At least two successive generations must be affected. • At least one relative with a Lynch syndrome associated cancer should be diagnosed before 50 years of age. • Familial Adenomatous Polyposis should be excluded. • Tumors should be verified whenever possible. Because family history can sometimes be difficult to obtain or confirm NCCN in those circumstances has recommended screening all newly diagnosed colorectal cancer patients for Lynch syndrome. Germline defects/mutations in the mismatch repair genes MLH1, MSH2, MSH6 and PMS2 results in microsatellite instability in tumors. Tumors are described as MSI-High when they have changes in 2 or more, of the 5 microsatellite markers. So, High levels of MSI within a tumor are suggestive of defective DNA mismatch repair. ImmunoHistoChemistry (IHC) staining of tumor tissue is performed for protein expression of the four mismatch repair genes known to be mutated in Lynch Syndrome (MLH1, MSH2, MSH6 and PMS2). IHC test is described as normal when all 4 mismatch repair proteins are normally expressed suggesting that an underlying mismatch repair gene mutation is unlikely. When IHC test is abnormal, it means that that at least one of the 4 mismatch repair proteins is not expressed and an inherited mutation may be present in the gene related to that protein. This can be further confirmed by mutation analysis of the corresponding gene. Screening tests for Lynch syndrome include IHC staining of tumor tissue for protein expression of the four mismatch repair genes and tumor evaluation for MSI. In LS, more than 90% of the tumors are MSI-H (microsatellite instability-high) and/or lack expression of at least one of the mismatch repair proteins by IHC staining and there is a 96% correlation between IHC and MSI when used as a screening test for LS. Approximately 5% of tumors that display MSI may have normal protein expression for the four mismatch repair genes. It should be noted that an abnormal MSI and/or IHC test in colon cancer patients is not diagnostic of Lynch syndrome but can be a useful screening test. This is because even though MSI in the tumor tissue is pathognomonic of Lynch syndrome, approximately 15% of patients with sporadic colorectal cancers exhibit tumors with high MSI as a result of somatic MLH1 promoter hypermethylation. Further, the majority of colon cancer tumors that lack protein expression on IHC staining of MLH1 (often coexisting with loss of PMS2) are often due to an acquired genetic defect. If the IHC indicates absence of MLH1 protein expression, tumor should be tested for BRAF mutation V600E which can be seen in sporadic colorectal cancers but rarely found in patients who have Lynch Syndrome. Once a diagnosis of Lynch Syndrome is made, at risk family members should undergo colonoscopic evaluation at 20-25 years of age or 2-5 years prior to the earliest colon cancer, if it is diagnosed before age 25 and is repeated every 1-2 years. Prophylactic hysterectomy and bilateral salpingo-oophorectomy (BSO) should be considered by women who have completed childbearing. NCCN Guidelines Version 1.2014 Lynch Syndrome
When any of these genes are mutated, repair of DNA replication mistakes is prevented resulting in continuous division of abnormal cells and possibly cancer. The EPCAM gene lies next to the MSH2 gene on chromosome 2 and mutations in the EPCAM gene can cause the MSH2 gene to be inactivated, interrupting DNA repair and leading to accumulation of DNA replication errors and possible malignancy. A Clinical Diagnosis of Lynch Syndrome can be made based on personal and family history if at least three relatives have a malignancy associated with Lynch Syndrome such as colorectal, endometrial, small bowel, ureter or renal pelvis cancer. In addition the following criteria should be met: • One relative must be a first-degree relative of the other two. • At least two successive generations must be affected. • At least one relative with a Lynch syndrome associated cancer should be diagnosed before 50 years of age. • Familial Adenomatous Polyposis should be excluded. • Tumors should be verified whenever possible. Because family history can sometimes be difficult to obtain or confirm NCCN in those circumstances has recommended screening all newly diagnosed colorectal cancer patients for Lynch syndrome. Germline defects/mutations in the mismatch repair genes MLH1, MSH2, MSH6 and PMS2 results in microsatellite instability in tumors. Tumors are described as MSI-High when they have changes in 2 or more, of the 5 microsatellite markers. So, High levels of MSI within a tumor are suggestive of defective DNA mismatch repair. ImmunoHistoChemistry (IHC) staining of tumor tissue is performed for protein expression of the four mismatch repair genes known to be mutated in Lynch Syndrome (MLH1, MSH2, MSH6 and PMS2). IHC test is described as normal when all 4 mismatch repair proteins are normally expressed suggesting that an underlying mismatch repair gene mutation is unlikely. When IHC test is abnormal, it means that that at least one of the 4 mismatch repair proteins is not expressed and an inherited mutation may be present in the gene related to that protein. This can be further confirmed by mutation analysis of the corresponding gene. Screening tests for Lynch syndrome include IHC staining of tumor tissue for protein expression of the four mismatch repair genes and tumor evaluation for MSI. In LS, more than 90% of the tumors are MSI-H (microsatellite instability-high) and/or lack expression of at least one of the mismatch repair proteins by IHC staining and there is a 96% correlation between IHC and MSI when used as a screening test for LS. Approximately 5% of tumors that display MSI may have normal protein expression for the four mismatch repair genes. It should be noted that an abnormal MSI and/or IHC test in colon cancer patients is not diagnostic of Lynch syndrome but can be a useful screening test. This is because even though MSI in the tumor tissue is pathognomonic of Lynch syndrome, approximately 15% of patients with sporadic colorectal cancers exhibit tumors with high MSI as a result of somatic MLH1 promoter hypermethylation. Further, the majority of colon cancer tumors that lack protein expression on IHC staining of MLH1 (often coexisting with loss of PMS2) are often due to an acquired genetic defect. If the IHC indicates absence of MLH1 protein expression, tumor should be tested for BRAF mutation V600E which can be seen in sporadic colorectal cancers but rarely found in patients who have Lynch Syndrome. Once a diagnosis of Lynch Syndrome is made, at risk family members should undergo colonoscopic evaluation at 20-25 years of age or 2-5 years prior to the earliest colon cancer, if it is diagnosed before age 25 and is repeated every 1-2 years. Prophylactic hysterectomy and bilateral salpingo-oophorectomy (BSO) should be considered by women who have completed childbearing. NCCN Guidelines Version 1.2014 Lynch Syndrome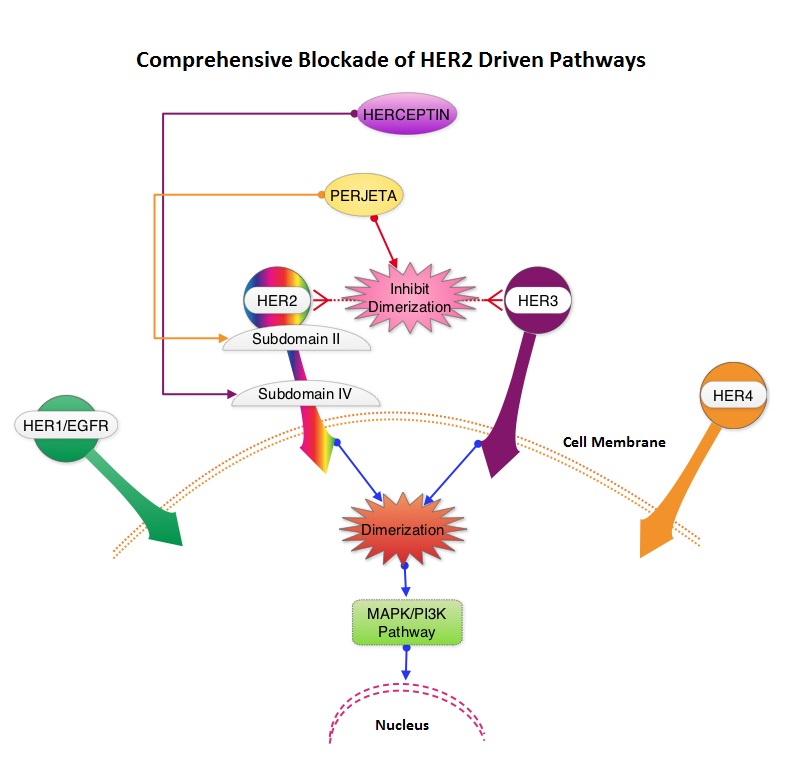 These proteins are transmembrane tyrosine kinases and are involved in normal cell growth and differentiation. HER1 is also known as Epidermal Growth Factor Receptor or EGFR. These receptors are activated following ligand binding, receptor pairing or dimerization and phosphorylation. This dimerization (receptor pairing) occurs often within the HER family of receptors. This has been no ligand identified for HER2 receptor, although it is able to form homo and heterodimers with other members of the HER family readily. Dimerization of HER2 and HER3 is believed to produce the strongest mitogenic signaling and activates two important pathways that regulate cell survival and growth – Mitogen Activated Protein Kinase (MAPK) pathway and PhosphoInositide 3-Kinase (PI3K) pathway. For this reason inhibiting HER2 dimerization appears to be an important step in the treatment of cancer. Overexpression of HER2 in breast cancer has been associated with higher risk for relapse as well as overall survival. Approximately 20 percent of breast cancers are HER2-positive. HERCEPTIN® is a humanized monoclonal antibody targeting HER2. It binds to the extracellular subdomain IV of the receptor and disrupts ligand independent HER2 downstream cell signaling pathways. PERJETA® is a recombinant, humanized, monoclonal antibody that binds to the HER2 subdomain II and blocks ligand dependent HER2 heterodimerization with other HER receptors, ie. HER3, HER1 and HER4. Thus HERCEPTIN® along with PERJETA® provide a more comprehensive blockade of HER2 driven signaling pathways. The accelerated approval of PERJETA® for the neoadjuvant treatment of breast cancer was based on a randomized, multicenter, open-label, phase II trial, in which 417 patients with HER2-positive, operable, locally advanced or inflammatory breast cancer (T2-4d), were randomly assigned to receive preoperative therapy with either HERCEPTIN® plus TAXOTERE® (Docetaxel), PERJETA® plus HERCEPTIN® and TAXOTERE®, PERJETA® plus HERCEPTIN® or PERJETA® plus TAXOTERE®. Patients in the three drug group received preoperative therapy with PERJETA®, HERCEPTIN® and TAXOTERE® every 3 weeks for a total of 4 cycles and following surgery, all patients received 3 cycles of Fluorouracil, ELLENCE® (Epirubicin), and CYTOXAN® (Cyclophosphamide) – (FEC) IV every 3 weeks and HERCEPTIN® was continued every 3 weeks for a total of one year of therapy. The primary endpoint was pathological Complete Response (pCR) rate defined as the absence of invasive cancer in the breast. The FDA definition of pCR is the absence of invasive cancer in the breast and lymph nodes. All treatment groups were well balanced. Seven percent of patients had inflammatory breast cancer, 32% had locally advanced cancer and 70% had clinically node-positive breast cancer. Forty-seven percent of the patients had hormone receptor-positive disease. The FDA defined pCR rates were 39.3% in the PERJETA® plus HERCEPTIN® and TAXOTERE® group and 21.5% in the HERCEPTIN® plus TAXOTERE® group (P=0.0063). Of Interest, the pCR rates in the three drug group were lower in patients with hormone receptor positive tumors compared to patients with hormone receptor negative tumors. The most common adverse events in the three drug group were alopecia, diarrhea, nausea and neutropenia. Other significant side effects included decreased cardiac function, infusion-related reactions, hypersensitivity reactions and anaphylaxis. Based on clinical studies, for the neoadjuvant treatment of breast cancer, PERJETA® should be administered every 3 weeks for 3 to 6 cycles as part of one of the following treatment regimens for early breast cancer. • Four preoperative cycles of PERJETA® in combination with HERCEPTIN® and TAXOTERE® followed by 3 postoperative cycles of Fluorouracil, ELLENCE® and CYTOXAN® (FEC). • Three preoperative cycles of FEC alone followed by 3 preoperative cycles of PERJETA® in combination with TAXOTERE® and HERCEPTIN®. • Six preoperative cycles of PERJETA® in combination with TAXOTERE®, Carboplatin, and HERCEPTIN® (TCH). Following surgery, patients should continue to receive HERCEPTIN® to complete 1 year of treatment. The accelerated approval by the FDA was based solely on the improved pCR rate with the three drug combination with no demonstrable improvement in event-free survival or overall survival. A confirmatory phase III trial is underway, with results expected in 2016. Gianni L, Pienkowski T, Im YH, et al. Lancet Oncol. 2012;13:25-32
These proteins are transmembrane tyrosine kinases and are involved in normal cell growth and differentiation. HER1 is also known as Epidermal Growth Factor Receptor or EGFR. These receptors are activated following ligand binding, receptor pairing or dimerization and phosphorylation. This dimerization (receptor pairing) occurs often within the HER family of receptors. This has been no ligand identified for HER2 receptor, although it is able to form homo and heterodimers with other members of the HER family readily. Dimerization of HER2 and HER3 is believed to produce the strongest mitogenic signaling and activates two important pathways that regulate cell survival and growth – Mitogen Activated Protein Kinase (MAPK) pathway and PhosphoInositide 3-Kinase (PI3K) pathway. For this reason inhibiting HER2 dimerization appears to be an important step in the treatment of cancer. Overexpression of HER2 in breast cancer has been associated with higher risk for relapse as well as overall survival. Approximately 20 percent of breast cancers are HER2-positive. HERCEPTIN® is a humanized monoclonal antibody targeting HER2. It binds to the extracellular subdomain IV of the receptor and disrupts ligand independent HER2 downstream cell signaling pathways. PERJETA® is a recombinant, humanized, monoclonal antibody that binds to the HER2 subdomain II and blocks ligand dependent HER2 heterodimerization with other HER receptors, ie. HER3, HER1 and HER4. Thus HERCEPTIN® along with PERJETA® provide a more comprehensive blockade of HER2 driven signaling pathways. The accelerated approval of PERJETA® for the neoadjuvant treatment of breast cancer was based on a randomized, multicenter, open-label, phase II trial, in which 417 patients with HER2-positive, operable, locally advanced or inflammatory breast cancer (T2-4d), were randomly assigned to receive preoperative therapy with either HERCEPTIN® plus TAXOTERE® (Docetaxel), PERJETA® plus HERCEPTIN® and TAXOTERE®, PERJETA® plus HERCEPTIN® or PERJETA® plus TAXOTERE®. Patients in the three drug group received preoperative therapy with PERJETA®, HERCEPTIN® and TAXOTERE® every 3 weeks for a total of 4 cycles and following surgery, all patients received 3 cycles of Fluorouracil, ELLENCE® (Epirubicin), and CYTOXAN® (Cyclophosphamide) – (FEC) IV every 3 weeks and HERCEPTIN® was continued every 3 weeks for a total of one year of therapy. The primary endpoint was pathological Complete Response (pCR) rate defined as the absence of invasive cancer in the breast. The FDA definition of pCR is the absence of invasive cancer in the breast and lymph nodes. All treatment groups were well balanced. Seven percent of patients had inflammatory breast cancer, 32% had locally advanced cancer and 70% had clinically node-positive breast cancer. Forty-seven percent of the patients had hormone receptor-positive disease. The FDA defined pCR rates were 39.3% in the PERJETA® plus HERCEPTIN® and TAXOTERE® group and 21.5% in the HERCEPTIN® plus TAXOTERE® group (P=0.0063). Of Interest, the pCR rates in the three drug group were lower in patients with hormone receptor positive tumors compared to patients with hormone receptor negative tumors. The most common adverse events in the three drug group were alopecia, diarrhea, nausea and neutropenia. Other significant side effects included decreased cardiac function, infusion-related reactions, hypersensitivity reactions and anaphylaxis. Based on clinical studies, for the neoadjuvant treatment of breast cancer, PERJETA® should be administered every 3 weeks for 3 to 6 cycles as part of one of the following treatment regimens for early breast cancer. • Four preoperative cycles of PERJETA® in combination with HERCEPTIN® and TAXOTERE® followed by 3 postoperative cycles of Fluorouracil, ELLENCE® and CYTOXAN® (FEC). • Three preoperative cycles of FEC alone followed by 3 preoperative cycles of PERJETA® in combination with TAXOTERE® and HERCEPTIN®. • Six preoperative cycles of PERJETA® in combination with TAXOTERE®, Carboplatin, and HERCEPTIN® (TCH). Following surgery, patients should continue to receive HERCEPTIN® to complete 1 year of treatment. The accelerated approval by the FDA was based solely on the improved pCR rate with the three drug combination with no demonstrable improvement in event-free survival or overall survival. A confirmatory phase III trial is underway, with results expected in 2016. Gianni L, Pienkowski T, Im YH, et al. Lancet Oncol. 2012;13:25-32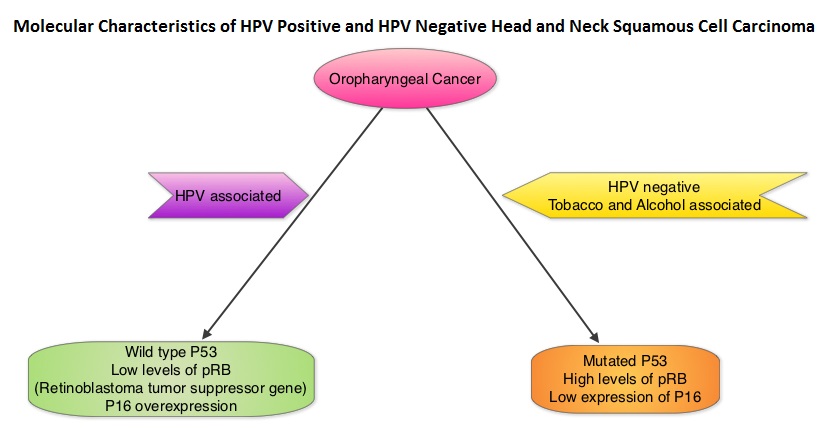 Chronic immunosuppression as seen in patients with HIV and in patients undergoing solid organ transplantation, may increase the risk for HPV infections. Patients with HPV associated oropharyngeal cancer typically are younger males, tend not to smoke or drink and present with poorly differentiated, non keratinizing tumors with basaloid morphology, compared to those with HPV negative tumors. Clinical characteristics of HPV positive oropharyngeal cancer patients with best outcomes include, those with fewer than 10 pack year smoking history and lower tumor stage. Several retrospective trials as well as some small prospective studies have shown that HPV positive oropharygeal cancers when treated with chemoradiation have significantly higher response rates, progression free survival, overall survival and better local and regional disease control. In the TAX 324 randomized phase III trial, patients received induction treatment with 3 cycles of TAXOTERE®, Cisplatin and 5-Fluorouracil (5-FU) or Cisplatin and 5-FU followed by chemoradiation with concurrent PARAPLATIN® (Carboplatin). Even though the 3 drug induction treatment group had superior outcomes compared to those who received 2 drug induction regimen in the intent to treat population, on retrospective analysis, patients with HPV positive oropharyngeal cancer had a significantly longer 5 year progression free survival (78% vs 28%) and overall survival, with an 80% reduction in mortality (HR=0.20, P<0.0001), compared to HPV negative patients, regardless of induction treatment. Other studies have shown that HPV positive patients who undergo surgery alone for oropharyngeal cancer do not appear to reap these favorable benefits, suggesting that the improved prognosis in the HPV positive patients with oropharyngeal cancer is related to chemotherapy and radiation. It also appears that HPV positive patients with oropharyngeal cancer have a better prognosis with treatment when their tumors are P53 wild type and express P16. With regards to EGFR and P16, there appears to be an inverse correlation between P16 and EGFR expression and patients with tumors expressing P16 and not EGFR have a significantly higher 5 year disease free and overall survival compared to those whose tumors overexpress EGFR but not P16. This information may have significant therapeutic implications and studies are underway trying to address this group of patients with targeted and less intense treatments. It should be noted that HPV positive status has a favorable prognostic value only for oropharyngeal primary cancers and not for other cancers of the head and neck.
Chronic immunosuppression as seen in patients with HIV and in patients undergoing solid organ transplantation, may increase the risk for HPV infections. Patients with HPV associated oropharyngeal cancer typically are younger males, tend not to smoke or drink and present with poorly differentiated, non keratinizing tumors with basaloid morphology, compared to those with HPV negative tumors. Clinical characteristics of HPV positive oropharyngeal cancer patients with best outcomes include, those with fewer than 10 pack year smoking history and lower tumor stage. Several retrospective trials as well as some small prospective studies have shown that HPV positive oropharygeal cancers when treated with chemoradiation have significantly higher response rates, progression free survival, overall survival and better local and regional disease control. In the TAX 324 randomized phase III trial, patients received induction treatment with 3 cycles of TAXOTERE®, Cisplatin and 5-Fluorouracil (5-FU) or Cisplatin and 5-FU followed by chemoradiation with concurrent PARAPLATIN® (Carboplatin). Even though the 3 drug induction treatment group had superior outcomes compared to those who received 2 drug induction regimen in the intent to treat population, on retrospective analysis, patients with HPV positive oropharyngeal cancer had a significantly longer 5 year progression free survival (78% vs 28%) and overall survival, with an 80% reduction in mortality (HR=0.20, P<0.0001), compared to HPV negative patients, regardless of induction treatment. Other studies have shown that HPV positive patients who undergo surgery alone for oropharyngeal cancer do not appear to reap these favorable benefits, suggesting that the improved prognosis in the HPV positive patients with oropharyngeal cancer is related to chemotherapy and radiation. It also appears that HPV positive patients with oropharyngeal cancer have a better prognosis with treatment when their tumors are P53 wild type and express P16. With regards to EGFR and P16, there appears to be an inverse correlation between P16 and EGFR expression and patients with tumors expressing P16 and not EGFR have a significantly higher 5 year disease free and overall survival compared to those whose tumors overexpress EGFR but not P16. This information may have significant therapeutic implications and studies are underway trying to address this group of patients with targeted and less intense treatments. It should be noted that HPV positive status has a favorable prognostic value only for oropharyngeal primary cancers and not for other cancers of the head and neck.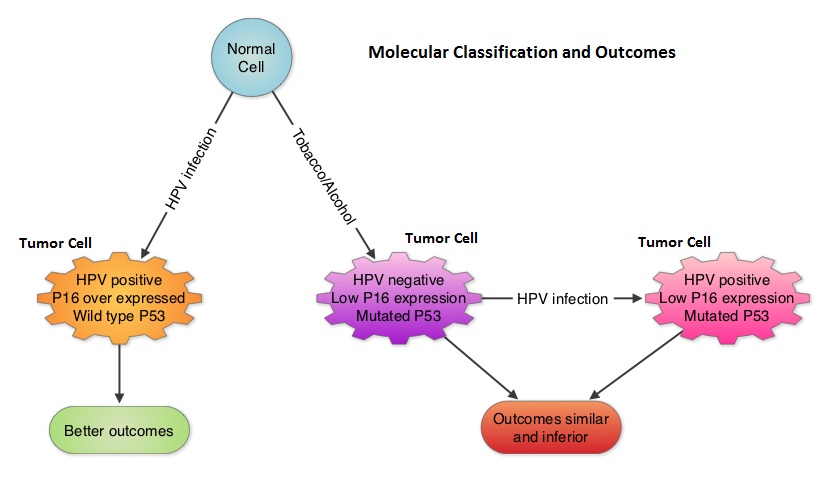
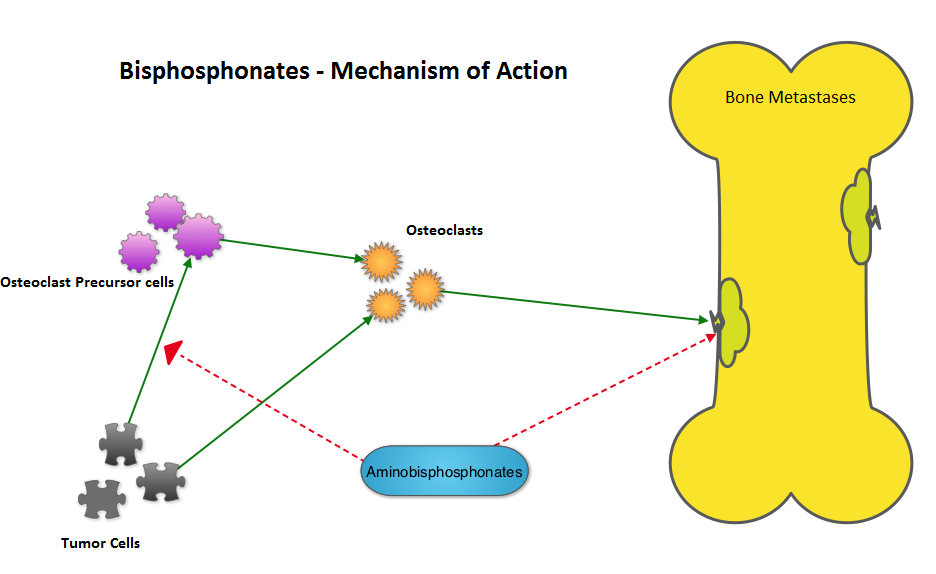 The AZURE investigators conducted a study to determine whether the addition of RECLAST® (Zoledronic acid) to standard adjuvant therapy would improve disease outcomes in patients with early-stage breast cancer. They noted that in the subset analysis, the addition of RECLAST® significantly improved disease free survival and overall survival in postmenopausal patients, independent of estrogen receptor status, tumor stage, and lymph node involvement (N Engl J Med 2011;365:1396-1405). With this background, the authors belonging to the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), conducted a meta-analysis and reviewed data from 15 years of bisphosphonate trials, which included 36 trials of adjuvant bisphosphonates in breast cancer and involved over 17,000 pre and postmenopausal women. RECLAST® (Zoledronic acid) and Clodronate were the most common bisphosphonates used in these trials. The primary outcomes analyzed were time to distant recurrence, local recurrence, new second primary breast cancer (ipsilateral or contralateral), time to first distant recurrence (ignoring any previous locoregional or contralateral recurrences), and breast cancer mortality. Planned subset analyses included site of recurrence, site of first distant metastasis (bone vs other), menopausal status (pre, peri and post) type of bisphosphonate (aminobisphosphonates such as RECLAST® or Clodronate) and drug schedule of bisphosphonate therapy (for bone protection vs advanced cancer). Adjuvant bisphosphonates resulted in a 34% reduction in the risk of bone recurrence (P = 0.00001) and a 17% reduction in the risk of breast cancer death (P =0.004). This benefit was seen regardless of estrogen receptor status, nodal status or whether chemotherapy was used or not. Bisphosphonates had no significant impact on non-breast cancer related deaths, contralateral breast cancer or loco-regional recurrence. In this meta-analysis, all these benefits were only seen in postmenopausal women and premenopausal women had no benefit on any disease outcomes with bisphosphonates. The authors emphasized that low estrogen environment as is seen in postmenopausal women, or women rendered menopausal by suppression of ovarian function is a prerequisite for adjuvant bisphosphonate activity. Based on this large meta-analysis, the authors recommended the use of RECLAST® once every six months or oral Clodronate, where available. Because of paucity of data, they do not recommend the use of weekly dose of oral bisphosphonates, often used to prevent osteoporosis, to achieve these benefits. Coleman R, Gnant M, Paterson A, et al. San Antonio Breast Cancer Symposium 2013; San Antonio, TX. Abstract S4-07.
The AZURE investigators conducted a study to determine whether the addition of RECLAST® (Zoledronic acid) to standard adjuvant therapy would improve disease outcomes in patients with early-stage breast cancer. They noted that in the subset analysis, the addition of RECLAST® significantly improved disease free survival and overall survival in postmenopausal patients, independent of estrogen receptor status, tumor stage, and lymph node involvement (N Engl J Med 2011;365:1396-1405). With this background, the authors belonging to the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), conducted a meta-analysis and reviewed data from 15 years of bisphosphonate trials, which included 36 trials of adjuvant bisphosphonates in breast cancer and involved over 17,000 pre and postmenopausal women. RECLAST® (Zoledronic acid) and Clodronate were the most common bisphosphonates used in these trials. The primary outcomes analyzed were time to distant recurrence, local recurrence, new second primary breast cancer (ipsilateral or contralateral), time to first distant recurrence (ignoring any previous locoregional or contralateral recurrences), and breast cancer mortality. Planned subset analyses included site of recurrence, site of first distant metastasis (bone vs other), menopausal status (pre, peri and post) type of bisphosphonate (aminobisphosphonates such as RECLAST® or Clodronate) and drug schedule of bisphosphonate therapy (for bone protection vs advanced cancer). Adjuvant bisphosphonates resulted in a 34% reduction in the risk of bone recurrence (P = 0.00001) and a 17% reduction in the risk of breast cancer death (P =0.004). This benefit was seen regardless of estrogen receptor status, nodal status or whether chemotherapy was used or not. Bisphosphonates had no significant impact on non-breast cancer related deaths, contralateral breast cancer or loco-regional recurrence. In this meta-analysis, all these benefits were only seen in postmenopausal women and premenopausal women had no benefit on any disease outcomes with bisphosphonates. The authors emphasized that low estrogen environment as is seen in postmenopausal women, or women rendered menopausal by suppression of ovarian function is a prerequisite for adjuvant bisphosphonate activity. Based on this large meta-analysis, the authors recommended the use of RECLAST® once every six months or oral Clodronate, where available. Because of paucity of data, they do not recommend the use of weekly dose of oral bisphosphonates, often used to prevent osteoporosis, to achieve these benefits. Coleman R, Gnant M, Paterson A, et al. San Antonio Breast Cancer Symposium 2013; San Antonio, TX. Abstract S4-07.