SUMMARY: The American Cancer Society estimates that 61,760 people will be diagnosed with Head and Neck cancer in 2016 and 13,190 patients will die of the disease. Over 90% of these malignancies are Squamous Cell Carcinomas (SCCs). Oropharyngeal Squamous Cell Carcinomas (OPSCC) involve the tonsils and base of the tongue and recent studies have shown that over 70% of these tumors are caused by Human Papilloma Virus (HPV) and HPV-16 is the predominant type present in the tumor cells. The CDC estimates that more than 2,370 new cases of Human Papilloma Virus associated Oropharyngeal Squamous Cell Carcinomas (OPSCC) are diagnosed in women and nearly 9,356 are diagnosed in men, each year in the United States and this incidence has been on the rise. The malignant behavior of these tumors is dependent on the expression of viral E6 and E7 oncoproteins that inactivate the tumor suppressor proteins p53 and the retinoblastoma protein (pRb), respectively. HPV-positive OroPharyngeal Squamous Cell Carcinoma is more common among never smokers or light smokers and patients tend to be younger with better performance status.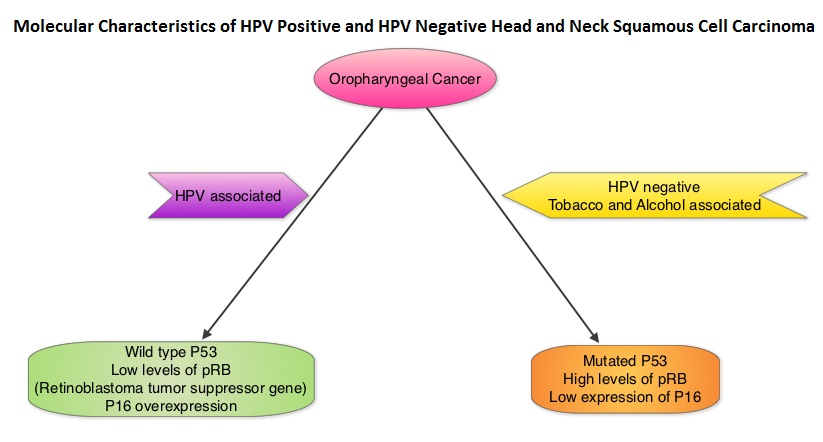
The authors conducted this prospective study to examine the temporal association between HPV DNA detection of alpha, beta and gamma Human Papilloma Virus (HPV) types in the oral samples and risk of Head and Neck Squamous Cell Carcinoma (HNSCC). A nested case-control study was carried out among 96,650 participants, cancer free at baseline, who provided mouthwash samples in 2 large prospective cohorts: the American Cancer Society Cancer Prevention Study II Nutrition Cohort and the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial (PLCO). Molecular Detection of DNA from alpha, beta and gamma HPV types in mouthwash samples was performed by next-generation sequencing method. Associations between oral HPV infection and Head and Neck Squamous Cell Carcinoma (HNSCC) were adjusted for smoking status, pack-years and number of alcoholic drinks per week, which are all known and established risk factors for HNSCC.
During an average follow up of 3.9 years in both cohorts, 132 cases of HNSCC were identified which included cancers of the Oropharynx, Oral cavity and Larynx. The authors after analyzing the 132 cases of HNSCC and 396 controls nested within 2 prospective cohorts, found that detection of oral HPV-16 DNA was associated with a 22.4 fold increased risk of incident Oropharyngeal Cancer. Detection of oral beta1-HPV-5 type and gamma11-HPV and gamma12-HPV species was associated with a 3.3 to 5.5 fold higher risk of HNSCC.
The authors concluded that HPV-16 detection in the oral cavity precedes the incidence of Oropharyngeal Squamous Cell Carcinoma and this is the first study to demonstrate a temporal association between HPV DNA detection in mouthwash specimens and risk of HNSCC. Further, other HPVs including beta and gamma species may also play a role in the etiology of HNSCC. Detection of HPV DNA in the oral cavity may have important implications for its use in Oropharygeal cancer screening program. Associations of Oral α-, β-, and γ-Human Papillomavirus Types with Risk of Incident Head and Neck Cancer. Agalliu I, Gapstur S, Chen Z, et al. JAMA Oncol. 2016;2:599-606