Late Breaking Abstract – ASCO 2016: Liquid Biopsy Can Rapidly Detect Certain Gene Mutations with High Specificity
SUMMARY: The FDA approved the first “Liquid Biopsy” test on June 1, 2016 for the detection of exon 19 deletions or exon 21 (L858R) substitution mutations in the Epidermal Growth Factor Receptor (EGFR) gene. On the heels of this approval, Zill and colleagues reported the results of the largest liquid biopsy study ever conducted thus far. It has been well established that treatment with EGFR TKIs results in superior outcomes, for patients with tumors harboring exon 19 deletions and exon 21 mutations. The application of precision medicine with targeted therapy requires detection of molecular abnormalities in a tumor specimen, following progression or recurrence. Archived biopsy specimens may not be helpful, as it is important to identify additional mutations in the tumor at the time of recurrence or progression, in order to plan appropriate therapy. Further, recurrent tumors may be inaccessible for a safe biopsy procedure or the clinical condition of the patient may not permit a repeat biopsy. Additionally, the biopsy itself may be subject to sampling error due to tumor heterogeneity. Genotyping cell free DNA in the plasma, also called liquid biopsy, can potentially overcome the shortcomings of repeat biopsies and tissue genotyping, allowing the detection of many more targetable gene mutations, thus resulting in better evaluation of the tumor genome landscape.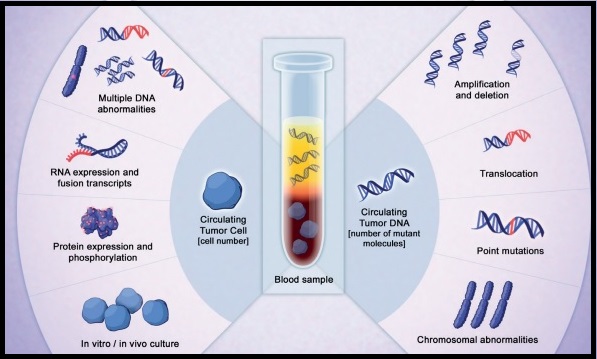
The authors in this study utilized Next Generation Sequencing (NGS) of circulating tumor DNA (ctDNA), isolated from plasma specimens (liquid biopsy specimens) of 15,191 patients of whom 37% had advanced lung cancer, 14% had breast cancer, 10% had colorectal cancer and 39% had other malignancies. Seventy genes were targeted and accuracy of ctDNA sequencing was assessed by comparing with matched tissue tests for 386 patients and frequencies of somatic ctDNA alterations per gene were compared to those previously described in tissue sequencing projects such as data from The Cancer Genome Atlas (TCGA).
It was noted that the ctDNA mutation patterns were highly concordant with tissue analysis as reported by the TCGA. The overall accuracy of ctDNA sequencing in comparison with matched tissue tests was 87% and the accuracy increased to 98% when blood and tumor were collected less than six months apart. Pearson Correlation between sets of data is a measure of how well these sets are related. Between 0.5 and 1.0 is considered high correlation. Pearson correlation for TP53 gene was 0.94, for KRAS was 0.99 and for PIK3CA was 0.99.
The researchers commented on the clinical outcome benefits using liquid biopsy, in four distinct groups:
1) Testing for actionable mutations (ALK fusion, EGFR or BRAF activating mutations in lung; ERBB2 amplification in gastric cancer) in cases with insufficient tissue quantity.
2) Testing for actionable resistance mutations (MET amplification or EGFR T790M in lung cancer), at the time of progression.
3) Genomic evolution upon progression such as ERBB2-amplified metastatic breast cancer in patients with triple negative primary tumor.
4) Tumors with genotypes that need more extensive driver mutation testing such as BRAF V600E in lung.
The authors concluded that there is a high correlation between ctDNA plasma samples and tissue testing with the exception of resistance mutations such as EGFR T790M mutation which evolve while on anti-EGFR inhibitor therapy and consequently may not correlate with the TCGA, probably because patients in the tissue-based population had not yet received the anti-EGFR inhibitor therapy that promotes the mutation. Patients who received treatment based on ctDNA findings also experienced better clinical outcomes. Zill OA, Mortimer S, Banks KC, et al Somatic genomic landscape of over 15,000 patients with advanced-stage cancer from clinical next-generation sequencing analysis of circulating tumor DNA. J Clin Oncol. 2016;34(suppl; abstr LBA11501).
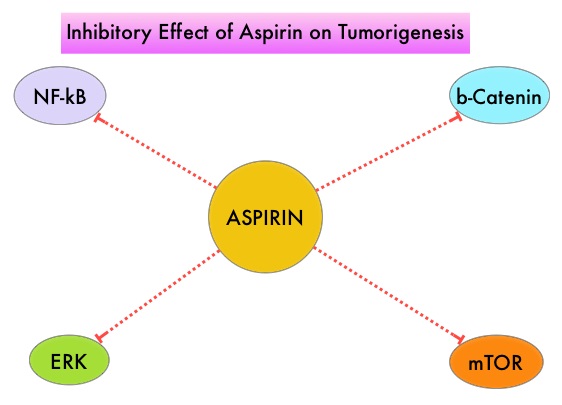
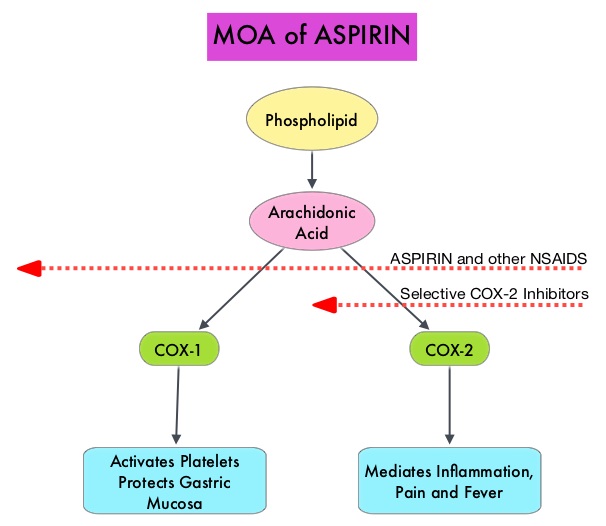 Even though the benefits of Aspirin in the primary prevention of CRC remains well established, the role of Aspirin in secondary prevention in patients with CRC (after the diagnosis of CRC) is unclear. Platelets have long been implicated in the mechanism of tumor metastases. More recent data suggests that platelets may play a role in tumorigenesis as well, through the release of angiogenic and growth factors due to overexpression of COX-2. Daily low dose Aspirin inhibits COX-1 and COX-2. It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties.
Even though the benefits of Aspirin in the primary prevention of CRC remains well established, the role of Aspirin in secondary prevention in patients with CRC (after the diagnosis of CRC) is unclear. Platelets have long been implicated in the mechanism of tumor metastases. More recent data suggests that platelets may play a role in tumorigenesis as well, through the release of angiogenic and growth factors due to overexpression of COX-2. Daily low dose Aspirin inhibits COX-1 and COX-2. It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties.