
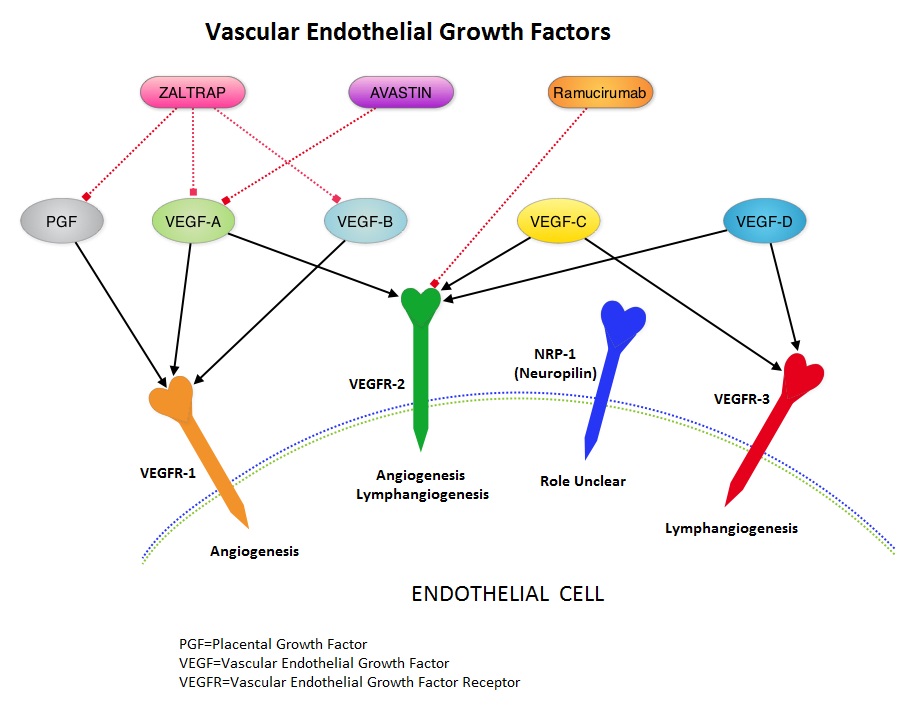
SUMMARY: It is estimated that there were approximately 21,600 new cases and 10,990 deaths from gastric cancer in the United States in 2013. The biology of gastric cancer appears to be different in different parts of the globe. Following progression after first line treatment for metastatic disease, the median survival is approximately 3 months. Ramucirumab is a human IgG1 monoclonal antibody that inhibits VEGF-receptor 2, unlike AVASTIN® (Bevacizumab) which inhibits VEGF-A. The RAINBOW study is an international, placebo-controlled, double-blind, phase III trial in which 665 patients with metastatic gastroesophageal junction or gastric adenocarcinoma, who had disease progression on or within 4 months after first-line platinum and fluoropyrimidine-based combination therapy, were included. Patients were randomly assigned to receive TAXOL® (Paclitaxel) 80 mg/m2 given on D1, 8, 15 along with Placebo (N=335) or the same dose and schedule of TAXOL® given along with Ramucirumab 8 mg/kg IV every 2 weeks (N=330), of a 28 day cycle. Treatment was continued until disease progression or unacceptable toxicities were noted. The primary endpoint was Overall Survival (OS). Secondary endpoints included Progression Free Survival (PFS), Objective Response Rate (ORR) and Time To Progression (TTP). The median OS for the combination of Ramucirumab and TAXOL® was 9.6 months compared to 7.4 months for Placebo and TAXOL® (P=0.016; HR=0.81), resulting in a 19% reduction in the risk of death with the Ramucirumab and TAXOL® combination. The secondary endpoints favored the Ramucirumab and TAXOL® combination as well. The median PFS was 4.4 months and 2.9 months (P<0.0001; HR=0.63), ORR was 28% and 16% (P<0.0001) and median TTP was 5.5 months and 3 months with the Ramucirumab and TAXOL® combination vs Placebo and TAXOL® combination respectively. As one would expect, treatment related adverse events were seen more frequently in the Ramucirumab and TAXOL® combination group. Significant were neutropenia, hypertension, fatigue and asthenia. The incidence of febrile neutropenia in the two treatment groups was however comparable (3.1% vs 2.4%). The authors concluded that the combination of Ramucirumab and TAXOL® significantly improved both progression-free and overall survival, with significantly improved disease control rates, in patients with metastatic gastroesophageal junction or gastric adenocarcinoma. Wilke H, Van Cutsem E, Oh SC, et al. J Clin Oncol 32, 2014 (suppl 3; abstr LBA7)
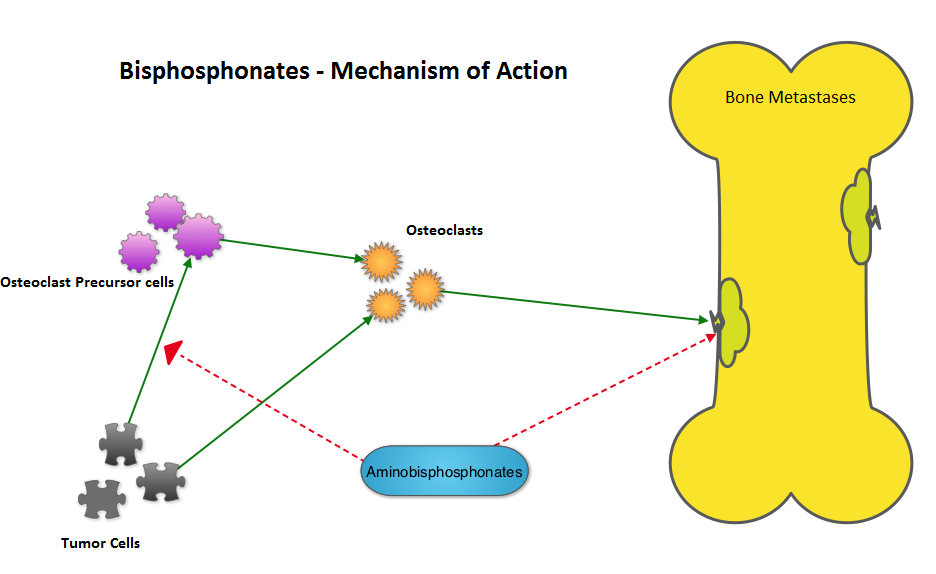 The AZURE investigators conducted a study to determine whether the addition of RECLAST® (Zoledronic acid) to standard adjuvant therapy would improve disease outcomes in patients with early-stage breast cancer. They noted that in the subset analysis, the addition of RECLAST® significantly improved disease free survival and overall survival in postmenopausal patients, independent of estrogen receptor status, tumor stage, and lymph node involvement (N Engl J Med 2011;365:1396-1405). With this background, the authors belonging to the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), conducted a meta-analysis and reviewed data from 15 years of bisphosphonate trials, which included 36 trials of adjuvant bisphosphonates in breast cancer and involved over 17,000 pre and postmenopausal women. RECLAST® (Zoledronic acid) and Clodronate were the most common bisphosphonates used in these trials. The primary outcomes analyzed were time to distant recurrence, local recurrence, new second primary breast cancer (ipsilateral or contralateral), time to first distant recurrence (ignoring any previous locoregional or contralateral recurrences), and breast cancer mortality. Planned subset analyses included site of recurrence, site of first distant metastasis (bone vs other), menopausal status (pre, peri and post) type of bisphosphonate (aminobisphosphonates such as RECLAST® or Clodronate) and drug schedule of bisphosphonate therapy (for bone protection vs advanced cancer). Adjuvant bisphosphonates resulted in a 34% reduction in the risk of bone recurrence (P = 0.00001) and a 17% reduction in the risk of breast cancer death (P =0.004). This benefit was seen regardless of estrogen receptor status, nodal status or whether chemotherapy was used or not. Bisphosphonates had no significant impact on non-breast cancer related deaths, contralateral breast cancer or loco-regional recurrence. In this meta-analysis, all these benefits were only seen in postmenopausal women and premenopausal women had no benefit on any disease outcomes with bisphosphonates. The authors emphasized that low estrogen environment as is seen in postmenopausal women, or women rendered menopausal by suppression of ovarian function is a prerequisite for adjuvant bisphosphonate activity. Based on this large meta-analysis, the authors recommended the use of RECLAST® once every six months or oral Clodronate, where available. Because of paucity of data, they do not recommend the use of weekly dose of oral bisphosphonates, often used to prevent osteoporosis, to achieve these benefits. Coleman R, Gnant M, Paterson A, et al. San Antonio Breast Cancer Symposium 2013; San Antonio, TX. Abstract S4-07.
The AZURE investigators conducted a study to determine whether the addition of RECLAST® (Zoledronic acid) to standard adjuvant therapy would improve disease outcomes in patients with early-stage breast cancer. They noted that in the subset analysis, the addition of RECLAST® significantly improved disease free survival and overall survival in postmenopausal patients, independent of estrogen receptor status, tumor stage, and lymph node involvement (N Engl J Med 2011;365:1396-1405). With this background, the authors belonging to the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), conducted a meta-analysis and reviewed data from 15 years of bisphosphonate trials, which included 36 trials of adjuvant bisphosphonates in breast cancer and involved over 17,000 pre and postmenopausal women. RECLAST® (Zoledronic acid) and Clodronate were the most common bisphosphonates used in these trials. The primary outcomes analyzed were time to distant recurrence, local recurrence, new second primary breast cancer (ipsilateral or contralateral), time to first distant recurrence (ignoring any previous locoregional or contralateral recurrences), and breast cancer mortality. Planned subset analyses included site of recurrence, site of first distant metastasis (bone vs other), menopausal status (pre, peri and post) type of bisphosphonate (aminobisphosphonates such as RECLAST® or Clodronate) and drug schedule of bisphosphonate therapy (for bone protection vs advanced cancer). Adjuvant bisphosphonates resulted in a 34% reduction in the risk of bone recurrence (P = 0.00001) and a 17% reduction in the risk of breast cancer death (P =0.004). This benefit was seen regardless of estrogen receptor status, nodal status or whether chemotherapy was used or not. Bisphosphonates had no significant impact on non-breast cancer related deaths, contralateral breast cancer or loco-regional recurrence. In this meta-analysis, all these benefits were only seen in postmenopausal women and premenopausal women had no benefit on any disease outcomes with bisphosphonates. The authors emphasized that low estrogen environment as is seen in postmenopausal women, or women rendered menopausal by suppression of ovarian function is a prerequisite for adjuvant bisphosphonate activity. Based on this large meta-analysis, the authors recommended the use of RECLAST® once every six months or oral Clodronate, where available. Because of paucity of data, they do not recommend the use of weekly dose of oral bisphosphonates, often used to prevent osteoporosis, to achieve these benefits. Coleman R, Gnant M, Paterson A, et al. San Antonio Breast Cancer Symposium 2013; San Antonio, TX. Abstract S4-07.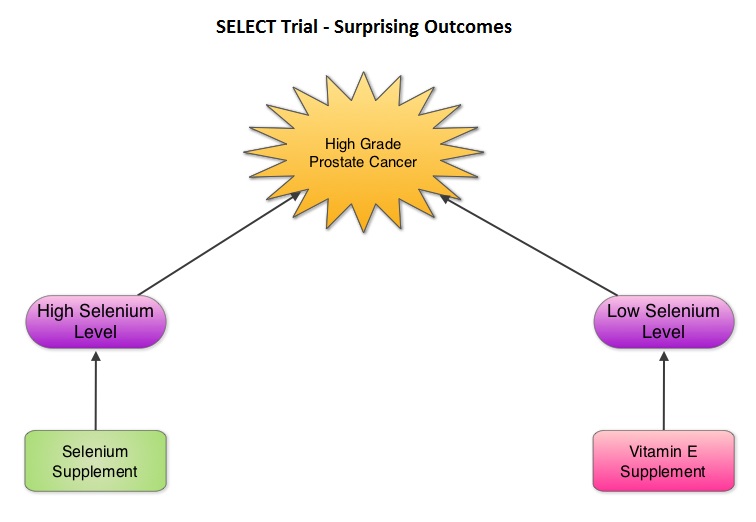 The SELECT trial, which began in 2001, was stopped early in 2008, as Selenium and Vitamin E, taken alone or together for an average of five and a half years did not decrease the incidence of prostate cancer. In 2011, an update on the SELECT trial data suggested that men who were randomized to the vitamin E alone had a 17 percent increased risk of prostate cancer compared to those men taking placebo. The authors in this case–cohort study continued follow up of the SELECT trial participants and with the Selenium levels data from toenail clippings, compared the effect of Selenium and Vitamin E, taken either alone or together, on the risk of prostate cancer, among 1739 men who were diagnosed with prostate cancer, of whom 489 participants developed high-grade prostate cancer. The control group for comparison was a random sample of 3117 men without prostate cancer and they were matched to the cases by race and age. It was noted that an individual’s baseline Selenium level, in the absence of supplementation, was not associated with prostate cancer risk. However, in men who had high baseline Selenium levels, Selenium supplements almost doubled (91%) the risk of high grade prostate cancer (P=0.007). Conversely, Vitamin E supplements had no effect among men with high baseline Selenium levels but doubled the risk of high grade prostate cancer among men with low baseline Selenium levels. Frankel et al. in an accompanying editorial point out that the dose of Vitamin E in the SELECT trial was significantly higher (400 IU/day) than the dose that was selected in the Alpha-Tocopherol Beta Carotene (ATBC) Cancer Prevention trial (50 IU/day), a study that was designed to test Vitamin E and beta carotene for lung cancer prevention in smokers. In the ATBC trial, a decrease in the incidence of prostate cancer incidence was observed, although this was a secondary finding and this study was not designed to determine prostate cancer risk. They comment that high doses of Vitamin E (Alpha-Tocopherol), suppresses the more potentially beneficial serum Gamma-Tocopherol which is the prevalent dietary form of Vitamin E in the United States. Selenium deficiency in the U.S. is not common and any benefit with Selenium supplements can only be seen in those who are Selenium deficient and high doses may be detrimental. The authors concluded that in the SELECT trial, the combination of both Vitamin E and Selenium did not reduce the risk of prostate cancer or any other cancer or heart disease and was in fact harmful for a significant number of individuals. Therefore, men 55 years of age or more should avoid Vitamin E or Selenium supplements at doses that exceed the recommended dietary intake. Kristal AR, Darke AK, Morris JS, et al. J Natl Cancer Inst; First published online 22 February 2014, doi: 10.1093/jnci/djt456
The SELECT trial, which began in 2001, was stopped early in 2008, as Selenium and Vitamin E, taken alone or together for an average of five and a half years did not decrease the incidence of prostate cancer. In 2011, an update on the SELECT trial data suggested that men who were randomized to the vitamin E alone had a 17 percent increased risk of prostate cancer compared to those men taking placebo. The authors in this case–cohort study continued follow up of the SELECT trial participants and with the Selenium levels data from toenail clippings, compared the effect of Selenium and Vitamin E, taken either alone or together, on the risk of prostate cancer, among 1739 men who were diagnosed with prostate cancer, of whom 489 participants developed high-grade prostate cancer. The control group for comparison was a random sample of 3117 men without prostate cancer and they were matched to the cases by race and age. It was noted that an individual’s baseline Selenium level, in the absence of supplementation, was not associated with prostate cancer risk. However, in men who had high baseline Selenium levels, Selenium supplements almost doubled (91%) the risk of high grade prostate cancer (P=0.007). Conversely, Vitamin E supplements had no effect among men with high baseline Selenium levels but doubled the risk of high grade prostate cancer among men with low baseline Selenium levels. Frankel et al. in an accompanying editorial point out that the dose of Vitamin E in the SELECT trial was significantly higher (400 IU/day) than the dose that was selected in the Alpha-Tocopherol Beta Carotene (ATBC) Cancer Prevention trial (50 IU/day), a study that was designed to test Vitamin E and beta carotene for lung cancer prevention in smokers. In the ATBC trial, a decrease in the incidence of prostate cancer incidence was observed, although this was a secondary finding and this study was not designed to determine prostate cancer risk. They comment that high doses of Vitamin E (Alpha-Tocopherol), suppresses the more potentially beneficial serum Gamma-Tocopherol which is the prevalent dietary form of Vitamin E in the United States. Selenium deficiency in the U.S. is not common and any benefit with Selenium supplements can only be seen in those who are Selenium deficient and high doses may be detrimental. The authors concluded that in the SELECT trial, the combination of both Vitamin E and Selenium did not reduce the risk of prostate cancer or any other cancer or heart disease and was in fact harmful for a significant number of individuals. Therefore, men 55 years of age or more should avoid Vitamin E or Selenium supplements at doses that exceed the recommended dietary intake. Kristal AR, Darke AK, Morris JS, et al. J Natl Cancer Inst; First published online 22 February 2014, doi: 10.1093/jnci/djt456
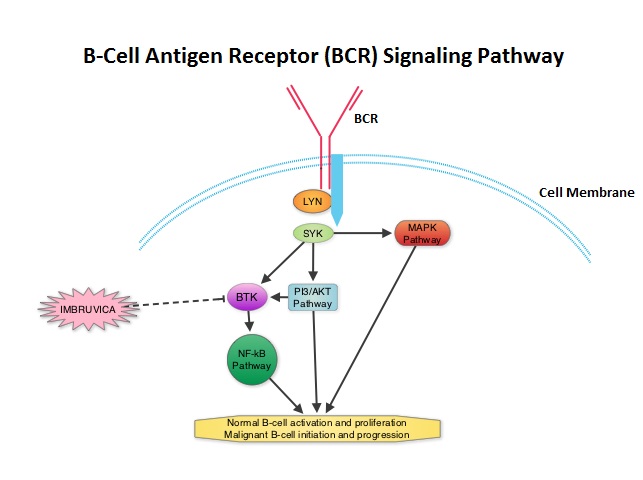 The FDA granted accelerated approval of IMBRUVICA® for the treatment of patients with Chronic Lymphocytic Leukemia (CLL) who had received at least one prior therapy. This approval was based on the outcomes in a select group of 48 patients who were a part of a larger group of 85 patients, enrolled in a multicenter single arm phase Ib/II trial. The median age was 67 years and 71% were male. Patients had a median number of 4 prior treatments and had an ECOG PS of 0-1. Patients in this group received IMBRUVICA® 420 mg PO daily until disease progression or unacceptable toxicity. The overall response rate was 58.3% as assessed by an independent review committee. No complete responses were seen and the response duration ranged from 5.6 to over 24 months. This analysis did not include data from those patients enrolled in the trial who received IMBRUVICA® 840 mg PO daily or those with Small Lymphocytic Lymphoma (N=37). The most common toxicities included fatigue, myalgias and arthralgias, cytopenias, nausea, diarrhea, fever and rash. Transient asymptomatic increase in lymphocyte count with resolution of lymphadenopathy and splenomegaly was common but resolved with continued treatment. The confirmatory RESONATE trial is a multicenter, randomized, open-label Phase III study in which single agent IMBRUVICA® was compared to single agent ARZERRA® (Ofatumumab) in patients with relapsed or refractory CLL or Small Lymphocytic Lymphoma . This was a part of the requirement by the FDA. Enrolled patients had measurable nodal disease and were not eligible for treatment with purine analog-based therapy. In this study, 391 patients who had received at least one prior therapy, were enrolled and randomized to receive 420 mg of IMBRUVICA® orally once daily or ARZERRA® given intravenously. Treatment was given over a period of 24 weeks until disease progression or unacceptable toxicity. Patients randomized to the ARZERRA® group on disease progression were allowed to receive treatment with IMBRUVICA®. The primary endpoint of this study was progression-free survival and the secondary endpoint was overall survival. Following recommendations from the Independent Data Monitoring Committee (IDMC), the study was stopped earlier, as the primary endpoint as well as an important secondary endpoint of the study were met. At the planned interim analysis, patients in the IMBRUVICA® group showed a statistically significant improvement in progression-free survival, the primary endpoint of the study as well as a statistically significant improvement in overall survival, the secondary endpoint of the trial. This data confirmed the efficacy of IMBRUVICA® and gives patients with CLL, an important new treatment option. Byrd JC, Furman RR, Coutre SE, et al. N Engl J Med 2013; 369:32-42
The FDA granted accelerated approval of IMBRUVICA® for the treatment of patients with Chronic Lymphocytic Leukemia (CLL) who had received at least one prior therapy. This approval was based on the outcomes in a select group of 48 patients who were a part of a larger group of 85 patients, enrolled in a multicenter single arm phase Ib/II trial. The median age was 67 years and 71% were male. Patients had a median number of 4 prior treatments and had an ECOG PS of 0-1. Patients in this group received IMBRUVICA® 420 mg PO daily until disease progression or unacceptable toxicity. The overall response rate was 58.3% as assessed by an independent review committee. No complete responses were seen and the response duration ranged from 5.6 to over 24 months. This analysis did not include data from those patients enrolled in the trial who received IMBRUVICA® 840 mg PO daily or those with Small Lymphocytic Lymphoma (N=37). The most common toxicities included fatigue, myalgias and arthralgias, cytopenias, nausea, diarrhea, fever and rash. Transient asymptomatic increase in lymphocyte count with resolution of lymphadenopathy and splenomegaly was common but resolved with continued treatment. The confirmatory RESONATE trial is a multicenter, randomized, open-label Phase III study in which single agent IMBRUVICA® was compared to single agent ARZERRA® (Ofatumumab) in patients with relapsed or refractory CLL or Small Lymphocytic Lymphoma . This was a part of the requirement by the FDA. Enrolled patients had measurable nodal disease and were not eligible for treatment with purine analog-based therapy. In this study, 391 patients who had received at least one prior therapy, were enrolled and randomized to receive 420 mg of IMBRUVICA® orally once daily or ARZERRA® given intravenously. Treatment was given over a period of 24 weeks until disease progression or unacceptable toxicity. Patients randomized to the ARZERRA® group on disease progression were allowed to receive treatment with IMBRUVICA®. The primary endpoint of this study was progression-free survival and the secondary endpoint was overall survival. Following recommendations from the Independent Data Monitoring Committee (IDMC), the study was stopped earlier, as the primary endpoint as well as an important secondary endpoint of the study were met. At the planned interim analysis, patients in the IMBRUVICA® group showed a statistically significant improvement in progression-free survival, the primary endpoint of the study as well as a statistically significant improvement in overall survival, the secondary endpoint of the trial. This data confirmed the efficacy of IMBRUVICA® and gives patients with CLL, an important new treatment option. Byrd JC, Furman RR, Coutre SE, et al. N Engl J Med 2013; 369:32-42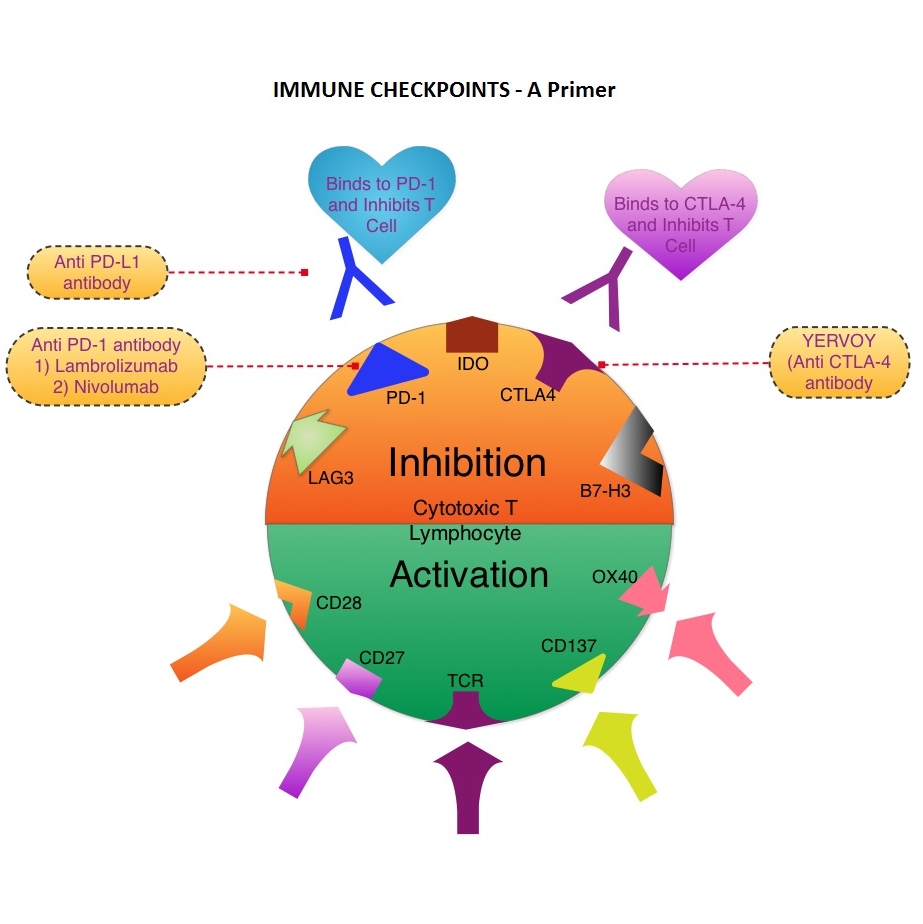 The T cells of the immune system play a very important role in modulating the immune system. EFFECTOR T cells include Cytotoxic T cells, Helper T cells, and Natural Killer (NK) cells, that enable the immune system to destroy cancer cells and pathogens. The REGULATORY T cells however, suppress immune response. Under normal circumstances, inhibition of an intense immune response and switching off the EFFECTOR T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. The mechanism can be compared to a lock and key where the appropriate Ligand (KEY) binds to the Immune checkpoint protein/receptor (LOCK) and activates or inhibits a T lymphocyte. With the ongoing understanding of tumor immunology and the recognition of Immune checkpoint proteins, researchers have focused on the development of antibodies that either target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4, PD-1, IDO, etc. (LOCK) or target the inhibitory soluble Ligands or antigens that are located on the surface of certain cancer cells (KEY) that bind to these Immune check point proteins/receptors. By doing so, one would expect to unleash the EFFECTOR T cells resulting in T cell proliferation, activation and a therapeutic response. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA-4, was approved by the FDA in March 2011 and has been shown to prolong overall survival in patients with previously treated unresectable or metastatic melanoma. The next immune check point protein/receptor studied for targeted therapy was PD-1. Lambrolizumab (MK-3475) is a humanized anti–PD-1 monoclonal antibody that demonstrated a 38% rapid and durable response rate and a more than 7 month median progression-free survival in patients with advanced melanoma, regardless of their prior therapy with YERVOY®. Nivolumab, another PD-1 targeted antibody demonstrated remarkable efficacy in a Phase I study with an overall response rate of 30%, median survival of 16.8 months and a 2 year survival of 44%. Based on this provocative data, a combination of Nivolumab and YERVOY® were studied in patients with advanced Stage III or IV melanoma who had received up to three prior therapies.. The idea was to block both the Immune checkpoints, PD-1 and CTLA-4, for improved efficacy. Fifty three (N=53) patients were treated with a combination of these two agents and 33 patients received these agents sequentially. Indeed, the highest response rate was over 50% in the combination group with 30% of these patients experienced a more than 80% response rate at 12 weeks of treatment whereas the response rate in the sequential treatment group was 20%. This preliminary study confirmed that blocking multiple Immune checkpoint proteins/receptors may result in rapid and durable responses in patients with advanced malignant melanoma. Phase III studies are underway to confirm this efficacy data and this concept is also being studied in other tumor types. Targeting/inhibiting the ligands (KEY) and preventing their binding to the Immune checkpoint protein/receptor, is another approach to stimulate antitumor immune response. PD-L1 protein (Ligand) which is often elevated in melanoma tumor cells, bind to PD-1 check point protein/receptor and can inhibit T cells and escape immune surveillance. An investigational PD-L1 targeted (Ligand targeted) engineered antibody (MPDL3280A) demonstrated a rapid response in 26% of the 45 patients with metastatic melanoma and the benefit was more so in those tumors expressing PD-L1. Promising activity has also been seen in advanced renal cell carcinoma. Antibodies targeting the Immune checkpoint receptor/protein or the Ligands binding to these receptors, are being developed, to carry payloads that are lethal to the checkpoint protein/receptor or Ligand. In conclusion, identifying as well as inhibiting certain Immune checkpoint proteins/receptors and/or Ligands that bind to these receptors, may give us new insights in the field of tumor immunology, resulting in better outcome for our cancer patients. Patel JD, Krilov L, Adams S, et al. J Clin Oncol 2013;32:129-160
The T cells of the immune system play a very important role in modulating the immune system. EFFECTOR T cells include Cytotoxic T cells, Helper T cells, and Natural Killer (NK) cells, that enable the immune system to destroy cancer cells and pathogens. The REGULATORY T cells however, suppress immune response. Under normal circumstances, inhibition of an intense immune response and switching off the EFFECTOR T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. The mechanism can be compared to a lock and key where the appropriate Ligand (KEY) binds to the Immune checkpoint protein/receptor (LOCK) and activates or inhibits a T lymphocyte. With the ongoing understanding of tumor immunology and the recognition of Immune checkpoint proteins, researchers have focused on the development of antibodies that either target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4, PD-1, IDO, etc. (LOCK) or target the inhibitory soluble Ligands or antigens that are located on the surface of certain cancer cells (KEY) that bind to these Immune check point proteins/receptors. By doing so, one would expect to unleash the EFFECTOR T cells resulting in T cell proliferation, activation and a therapeutic response. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA-4, was approved by the FDA in March 2011 and has been shown to prolong overall survival in patients with previously treated unresectable or metastatic melanoma. The next immune check point protein/receptor studied for targeted therapy was PD-1. Lambrolizumab (MK-3475) is a humanized anti–PD-1 monoclonal antibody that demonstrated a 38% rapid and durable response rate and a more than 7 month median progression-free survival in patients with advanced melanoma, regardless of their prior therapy with YERVOY®. Nivolumab, another PD-1 targeted antibody demonstrated remarkable efficacy in a Phase I study with an overall response rate of 30%, median survival of 16.8 months and a 2 year survival of 44%. Based on this provocative data, a combination of Nivolumab and YERVOY® were studied in patients with advanced Stage III or IV melanoma who had received up to three prior therapies.. The idea was to block both the Immune checkpoints, PD-1 and CTLA-4, for improved efficacy. Fifty three (N=53) patients were treated with a combination of these two agents and 33 patients received these agents sequentially. Indeed, the highest response rate was over 50% in the combination group with 30% of these patients experienced a more than 80% response rate at 12 weeks of treatment whereas the response rate in the sequential treatment group was 20%. This preliminary study confirmed that blocking multiple Immune checkpoint proteins/receptors may result in rapid and durable responses in patients with advanced malignant melanoma. Phase III studies are underway to confirm this efficacy data and this concept is also being studied in other tumor types. Targeting/inhibiting the ligands (KEY) and preventing their binding to the Immune checkpoint protein/receptor, is another approach to stimulate antitumor immune response. PD-L1 protein (Ligand) which is often elevated in melanoma tumor cells, bind to PD-1 check point protein/receptor and can inhibit T cells and escape immune surveillance. An investigational PD-L1 targeted (Ligand targeted) engineered antibody (MPDL3280A) demonstrated a rapid response in 26% of the 45 patients with metastatic melanoma and the benefit was more so in those tumors expressing PD-L1. Promising activity has also been seen in advanced renal cell carcinoma. Antibodies targeting the Immune checkpoint receptor/protein or the Ligands binding to these receptors, are being developed, to carry payloads that are lethal to the checkpoint protein/receptor or Ligand. In conclusion, identifying as well as inhibiting certain Immune checkpoint proteins/receptors and/or Ligands that bind to these receptors, may give us new insights in the field of tumor immunology, resulting in better outcome for our cancer patients. Patel JD, Krilov L, Adams S, et al. J Clin Oncol 2013;32:129-160