
The FDA on April 28, 2017 approved RYDAPT® (Midostaurin), a multikinase inhibitor, for the treatment of adult patients with newly diagnosed Acute Myeloid Leukemia (AML), who are FLT3 mutation-positive (FLT3+), as detected by an FDA-approved test, in combination with standard Cytarabine and Daunorubicin induction and Cytarabine consolidation. Activating mutations in the FLT3 receptor is the most common genetic abnormality in AML and is detected in approximately 30% of the patients. RYDAPT® along with chemotherapy significantly improved Overall Survival and represents a new standard of care for FLT3-mutated AML patients.
Tag: Acute Myeloid Leukemia
RYDAPT® (Midostaurin)
The FDA on April 28, 2017 approved RYDAPT® for the treatment of adult patients with newly diagnosed Acute Myeloid Leukemia (AML) who are FLT3 mutation-positive (FLT3+), as detected by an FDA-approved test, in combination with standard Cytarabine and Daunorubicin induction and Cytarabine consolidation. RYDAPT® is a product of Novartis Pharmaceuticals Corp.
FDA Approves RYDAPT®, A Targeted Multikinase Inhibitor for FLT3-Mutated Acute Myeloid leukemia
SUMMARY: The FDA on April 28, 2017 approved RYDAPT® for the treatment of adult patients with newly diagnosed Acute Myeloid Leukemia (AML) who are FLT3 mutation-positive (FLT3+), as detected by an FDA-approved test, in combination with standard Cytarabine and Daunorubicin induction and Cytarabine consolidation. The American Cancer Society estimates that in 2017, 21,380 new cases of Acute Myeloid Leukemia (AML) will be diagnosed in the United States and 10,590 patients will die of the disease. AML can be considered as a group of heterogeneous diseases with different clinical behavior and outcomes. Cytogenetic analysis has been part of routine evaluation when caring for patients with AML. By predicting resistance to therapy, tumor cytogenetics will stratify patients, based on risk and help manage them accordingly. Even though cytotoxic chemotherapy may lead to long term remission and cure in a minority of patients with favorable cytogenetics, patients with high risk features such as unfavorable cytogenetics, molecular abnormalities, prior myelodysplasia and advanced age, have poor outcomes with conventional chemotherapy alone.
The Fms-Like Tyrosine kinase 3 (FLT3) is a receptor tyrosine kinase in the PDGF family of growth factor receptors located on the cell surface (transmembrane) and plays an important role in both normal and malignant hematopoiesis by activating key signaling pathways. Activating mutations in the FLT3 receptor is the most common genetic abnormality in AML and is detected in approximately 30% of the patients. The three FLT3 mutation subtypes include Tyrosine Kinase Domain (TKD), Internal Tandem Duplications (ITD) high and ITD low. The most common FLT3 mutation is the FLT3-ITD accounting for about 75% of patients with a FLT3 mutation. The presence of FLT3-ITD mutations can negate the benefit of any other favorable molecular and cytogenetic features. Patients with FLT3-ITD mutations are predicted to have poor outcomes with shorter remission duration and significantly decreased leukemia free and overall survival. These mutations are detected using Polymerase Chain Reaction (PCR) based molecular diagnostic DNA testing.

VYXEOS® – A Novel First Line Treatment for High Risk Acute Myeloid Leukemia
SUMMARY: The American Cancer Society estimates that in 2016, 19,950 new cases of Acute Myeloid Leukemia (AML) will be diagnosed in the United States and 10,430 patients will die of the disease. Acute Myeloid Leukemia in general is a disease of the elderly and the average age of a patient with AML is about 66 years. AML can be considered as a group of heterogeneous diseases with different clinical behavior and outcomes. In general, only 40% of patients younger than 60 years of age survive more than 5 years and 5 year survival for those who relapse after achieving a complete remission (CR) is dismal. Treatment with conventional chemotherapy regimens in elderly patients with secondary AML (sAML) have resulted in poor outcomes. Even though rapid development of new agents against genetic and epigenetic targets is underway, modifications and reformulations of conventional chemotherapy have demonstrated improved outcomes in patients with AML.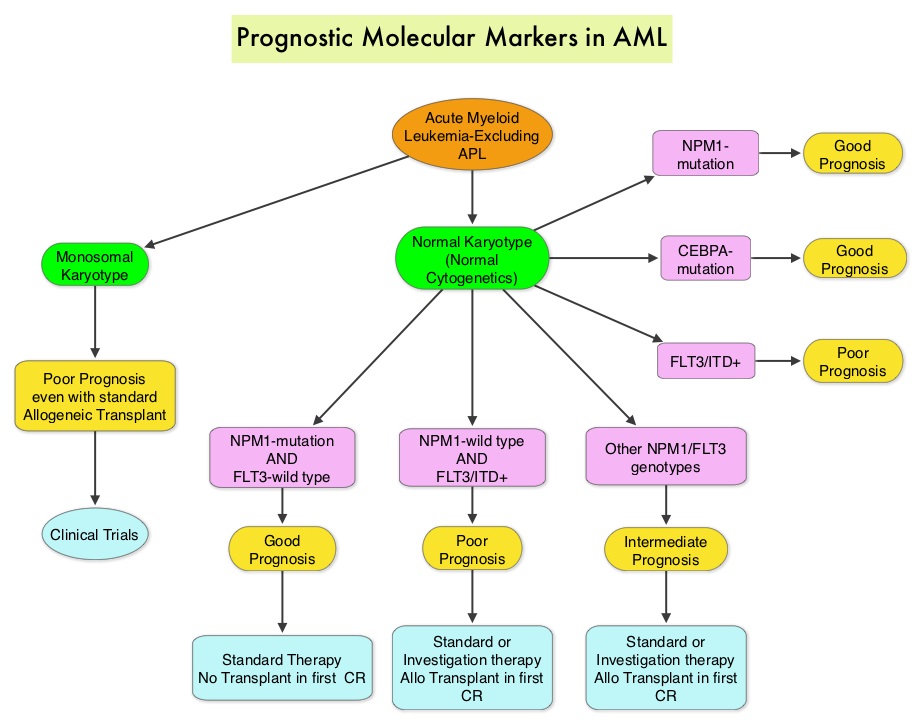
CPX-351 (VYXEOS®) is a liposomal formulation of a fixed combination of Cytarabine and Daunorubicin in a 5:1 molar ratio, developed using a platform known as “CombiPlex”. In vitro studies have demonstrated that this ratio maximizes synergy with the lowest level of antagonism and results in preferential uptake of the drug into leukemic cells. In a randomized, open label phase II trial involving patients with or without secondary AML (sAML), CPX-351 improved the composite CR (CRc) rate (Complete Remission and CR with incomplete blood count recovery – CRi) when compared to conventional induction chemotherapy with Daunorubicin and Cytarabine. Those patients with a higher rate of CRc (CR + CRi) had a statistically significant 6 month survival benefit. In another study of AML patients in first relapse, CPX-351 improved median Overall Survival (OS) in poor-risk patients when compared to investigator’s choice of salvage regimens.
On the basis of these studies, the authors conducted a randomized, open-label, phase III trial of first-line CPX-351 in patients with high-risk sAML. Enrolled patients (N=309) were stratified based on AML type (therapy-related AML, AML with a history of MDS with and without prior Hypo Methylating Agent therapy, AML with a history of CMML, or de novo AML with MDS karyotype) and age (60-69 yrs or 70-75yrs). Patients were randomized in a 1:1 ratio to receive either CPX-351 (N=153) 100 units/m2, days 1, 3, 5 or the standard 7+3 (Cytarabine 100 mg/m2/day x 7 days, Daunorubicin 60 mg/m2 days 1, 2, 3) induction therapy (N=156). Both treatment groups were well balanced. The primary end point was Overall Survival (OS) and secondary endpoints included Event Free Survival (EFS), independent blinded assessment of CR+CRi, and 60-day mortality.
The final analysis began after a minimum follow up of 13.7 months. Patients in the CPX-351 group had a significant improvement in Overall Survival compared with standard treatment (HR=0.69; P=0.005; median OS, 9.56 versus 5.95 months). Additionally, there was a significant improvement in Event Free Survival for the CPX-351 group compared to standard therapy (HR=0.74; P=0.021), as well as CR+CRi response (47.7% versus 33.3%; P=0.016) and 60-day mortality (13.7% versus 21.2%). The Complete Remission rates alone were 37.3% and 25.6%, in favor of CPX-351 (P=0.04). Grade 3-5 Adverse Events were similar in frequency and severity in both arms (92% versus 91%) and similar numbers of patients underwent transplantation in both treatment groups.
The authors concluded that treatment with CPX-351 (VYXEOS®) significantly improved Overall Survival, Event Free Survival and Response Rates, without an increase in 60-day mortality or Adverse Events, in elderly patients with high risk secondary AML, when compared with standard induction therapy. CPX-351 reduced the risk of death by 31%. Final results of a phase III randomized trial of CPX-351 versus 7+3 in older patients with newly diagnosed high risk (secondary) AML. Lancet JE, Uy GL, Cortes JE, et al. J Clin Oncol 34, 2016 (suppl; abstr 7000).
Prognostic significance of FLT3 internal tandem duplication, nucleophosmin 1, and CEBPA gene mutations for acute myeloid leukemia patients with normal karyotype and younger than 60 years a systematic review and meta-analysis
SUMMARY: The American Cancer Society estimates that in 2014, 18,860 new cases of Acute Myeloid Leukemia (AML) will be diagnosed in the United States and 10,460 patients will die of the disease. Acute Myeloid Leukemia in general is a disease of the elderly and the average age of a patient with AML is about 66 years. AML can be considered as a group of heterogeneous diseases with different clinical behavior and outcomes. Cytogenetic analysis has been part of routine evaluation when caring for patients with AML. By predicting resistance to therapy, tumor cytogenetics will stratify patients, based on risk and help manage them accordingly. Even though cytotoxic chemotherapy may lead to long term remission and cure in a minority of patients with favorable cytogenetics, patients with high risk features such as unfavorable cytogenetics, molecular abnormalities, prior myelodysplasia and advanced age, have poor outcomes with conventional chemotherapy.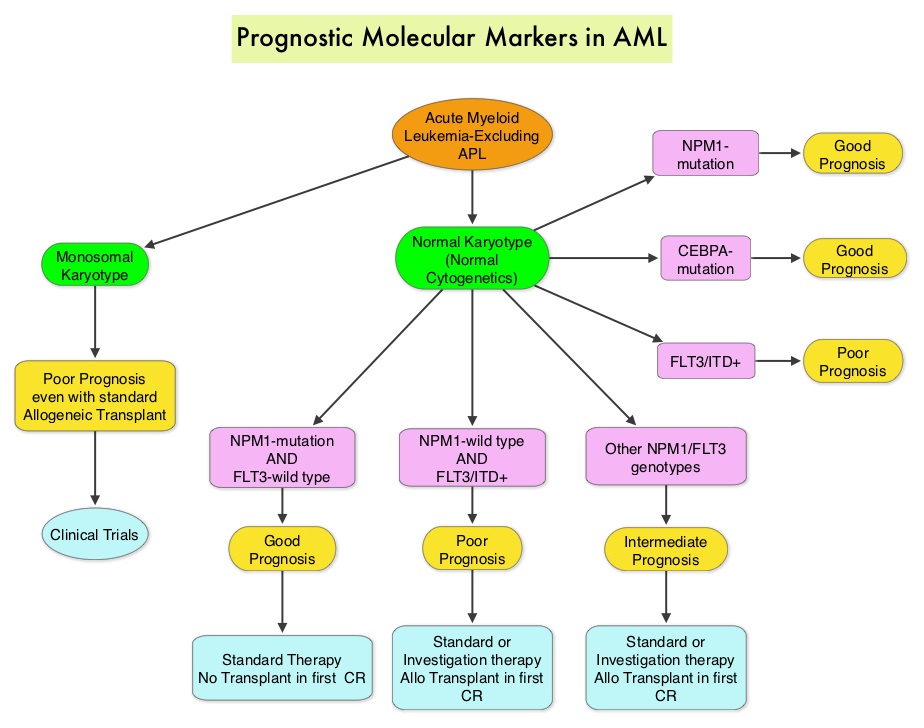 The Fms-Like Tyrosine kinase 3 (FLT3) is a receptor tyrosine kinase in the PDGF family of growth factor receptors located on the cell surface (transmembrane) and plays an important role in both normal and malignant hematopoiesis by activating key signaling pathways. Activating mutations in the FLT3 receptor is the most common genetic abnormality in AML and is detected in approximately 30% of the patients. The most common FLT3 mutation is the FLT3-ITD (Internal Tandem Duplication) mutation caused by tandem duplication within the coding region of the gene. The presence of FLT3-ITD mutations can negate the benefit of any other favorable molecular and cytogenetic features. Patients with FLT3-ITD mutations are predicted to have poor outcomes with shorter remission duration and significantly decreased leukemia free and overall survival. These mutations are detected using Polymerase Chain Reaction (PCR) based molecular diagnostic DNA testing. The authors in this meta-analysis examined the prognostic significance of three mutations frequently noted in patients with cytogenetically normal Acute Myeloid Leukemia. These mutations included FLT3-ITD, mutated NPM1 (Nucleophosmin) and mutations of the CCAAT enhancer-binding protein alpha (CEBPA) gene. This systematic review and meta-analysis included 1942 patients from multiple electronic databases from 2000 to March 2012. It was noted that FLT3-ITD was associated with the worse prognosis, with inferior Overall Survival (OS) and Relapse Free Survival (RFS), whereas mutations in NPM1 and CEBPA genes were associated with a favorable prognosis. The discovery of new molecular mutations in AML patients with normal cytogenetics may help predict outcomes and provide valuable information to facilitate risk-adapted therapy. Port M, Böttcher M, Thol F, et al. Ann Hematol. 2014;93:1279-1286
The Fms-Like Tyrosine kinase 3 (FLT3) is a receptor tyrosine kinase in the PDGF family of growth factor receptors located on the cell surface (transmembrane) and plays an important role in both normal and malignant hematopoiesis by activating key signaling pathways. Activating mutations in the FLT3 receptor is the most common genetic abnormality in AML and is detected in approximately 30% of the patients. The most common FLT3 mutation is the FLT3-ITD (Internal Tandem Duplication) mutation caused by tandem duplication within the coding region of the gene. The presence of FLT3-ITD mutations can negate the benefit of any other favorable molecular and cytogenetic features. Patients with FLT3-ITD mutations are predicted to have poor outcomes with shorter remission duration and significantly decreased leukemia free and overall survival. These mutations are detected using Polymerase Chain Reaction (PCR) based molecular diagnostic DNA testing. The authors in this meta-analysis examined the prognostic significance of three mutations frequently noted in patients with cytogenetically normal Acute Myeloid Leukemia. These mutations included FLT3-ITD, mutated NPM1 (Nucleophosmin) and mutations of the CCAAT enhancer-binding protein alpha (CEBPA) gene. This systematic review and meta-analysis included 1942 patients from multiple electronic databases from 2000 to March 2012. It was noted that FLT3-ITD was associated with the worse prognosis, with inferior Overall Survival (OS) and Relapse Free Survival (RFS), whereas mutations in NPM1 and CEBPA genes were associated with a favorable prognosis. The discovery of new molecular mutations in AML patients with normal cytogenetics may help predict outcomes and provide valuable information to facilitate risk-adapted therapy. Port M, Böttcher M, Thol F, et al. Ann Hematol. 2014;93:1279-1286
Final results of a randomized phase 2 study showing the clinical benefit of quizartinib (AC220) in patients with FLT3-ITD positive relapsed or refractory acute myeloid leukemia
SUMMARY: Acute Myeloid Leukemia (AML) is generally a disease of the elderly and the average age of a patient at the time of diagnosis is about 66 years. According to the American Cancer Society, approximately 18,860 new cases of AML will be diagnosed in 2014 and 10,460 patients will die of the disease. AML can be considered as a group of heterogeneous diseases with different clinical behavior and outcomes. Even though cytotoxic chemotherapy may lead to long term remission and cure in a minority of patients with favorable cytogenetics, patients with high risk features such as unfavorable cytogenetics, molecular abnormalities, prior myelodysplasia and advanced age, have poor outcomes with conventional chemotherapy. 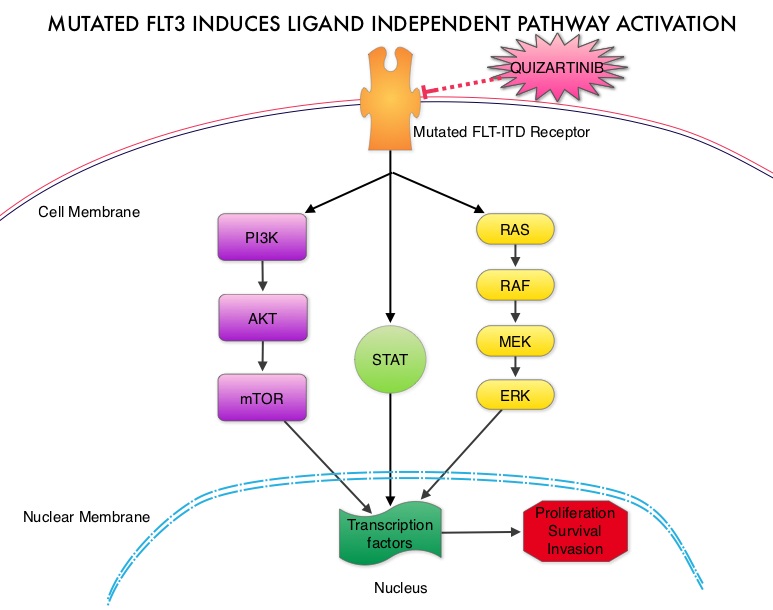 The fms-like tyrosine kinase 3 (FLT3) is a receptor tyrosine kinase in the PDGF family of growth factor receptors located on the cell surface (transmembrane) and plays an important role in both normal and malignant hematopoiesis by activating key signaling pathways. Activating mutations in the FLT3 receptor is the most common genetic abnormality in AML and is detected in approximately 30% of the patients. The most common FLT3 mutation is the FLT3-ITD (Internal Tandem Duplication) mutation caused by a tandem duplication within the coding region of the gene. The presence of FLT3-ITD mutations can negate the benefit of any other favorable molecular and cytogenetic features. Patients with FLT3-ITD mutations have poor outcomes with shorter remission duration and significantly decreased leukemia free and overall survival. These mutations are detected using Polymerase Chain Reaction (PCR) based molecular diagnostic DNA testing. Several therapeutic agents are being developed to target FLT3 mutations. Quizartinib (AC220) is an oral tyrosine kinase inhibitor, which has demonstrated activity in patients with both wild type FLT3 as well as those with FLT3-ITD mutations. In this randomized, open label phase II study, the authors evaluated the efficacy and safety of two different, lower dosages of Quizartinib, in patients 18 years of age or older, with FLT3-ITD positive, relapsed or refractory AML. Seventy six patients (N=76) were randomized to receive either Quizartinib 30 mg/day (Group A) or Quizartinib 60 mg/day (Group B), given orally and continuously, during a 28 day treatment cycle. Treatment was continued until relapse, intolerance or Hematopoietic Stem Cell Transplantation (HSCT). Both groups were well balanced except for age over 60 years (42% Group A, 26% Group B) and the percentage with secondary AML (8% Group A, 18% Group B). The composite Complete Remission (CRc) rate included Complete Remission (CR), Complete Remission with incomplete platelet recovery (CRp), and Complete Remission with incomplete hematologic recovery (CRi). The CRc rate in both groups A and B was 47% and the Overall Response Rate (CRc + Partial Response (PR)) was 61% in Group A and 71% in Group B. Further, 32% of patiens in Group A and 42% in Group B were able to undergo HSCT, after achieving CRc or PR. The most common treatment related adverse events were diarrhea (18%), febrile neutropenia (16%), and QT prolongation (15%). The QT prolongation rate was significantly less with lower doses of Quizartinib, as was used in this study, compared to what was noted with higher doses of Quizartinib utilized in other trials. The authors concluded that Quizartinib is highly effective in relapsed and refractory AML patients with FLT3-ITD mutations, with an acceptable safety profile. Schiller GJ, Tallman MS, Goldberg SL, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7100)
The fms-like tyrosine kinase 3 (FLT3) is a receptor tyrosine kinase in the PDGF family of growth factor receptors located on the cell surface (transmembrane) and plays an important role in both normal and malignant hematopoiesis by activating key signaling pathways. Activating mutations in the FLT3 receptor is the most common genetic abnormality in AML and is detected in approximately 30% of the patients. The most common FLT3 mutation is the FLT3-ITD (Internal Tandem Duplication) mutation caused by a tandem duplication within the coding region of the gene. The presence of FLT3-ITD mutations can negate the benefit of any other favorable molecular and cytogenetic features. Patients with FLT3-ITD mutations have poor outcomes with shorter remission duration and significantly decreased leukemia free and overall survival. These mutations are detected using Polymerase Chain Reaction (PCR) based molecular diagnostic DNA testing. Several therapeutic agents are being developed to target FLT3 mutations. Quizartinib (AC220) is an oral tyrosine kinase inhibitor, which has demonstrated activity in patients with both wild type FLT3 as well as those with FLT3-ITD mutations. In this randomized, open label phase II study, the authors evaluated the efficacy and safety of two different, lower dosages of Quizartinib, in patients 18 years of age or older, with FLT3-ITD positive, relapsed or refractory AML. Seventy six patients (N=76) were randomized to receive either Quizartinib 30 mg/day (Group A) or Quizartinib 60 mg/day (Group B), given orally and continuously, during a 28 day treatment cycle. Treatment was continued until relapse, intolerance or Hematopoietic Stem Cell Transplantation (HSCT). Both groups were well balanced except for age over 60 years (42% Group A, 26% Group B) and the percentage with secondary AML (8% Group A, 18% Group B). The composite Complete Remission (CRc) rate included Complete Remission (CR), Complete Remission with incomplete platelet recovery (CRp), and Complete Remission with incomplete hematologic recovery (CRi). The CRc rate in both groups A and B was 47% and the Overall Response Rate (CRc + Partial Response (PR)) was 61% in Group A and 71% in Group B. Further, 32% of patiens in Group A and 42% in Group B were able to undergo HSCT, after achieving CRc or PR. The most common treatment related adverse events were diarrhea (18%), febrile neutropenia (16%), and QT prolongation (15%). The QT prolongation rate was significantly less with lower doses of Quizartinib, as was used in this study, compared to what was noted with higher doses of Quizartinib utilized in other trials. The authors concluded that Quizartinib is highly effective in relapsed and refractory AML patients with FLT3-ITD mutations, with an acceptable safety profile. Schiller GJ, Tallman MS, Goldberg SL, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7100)
Effect of NPM1 and FLT3 Mutations on the Outcomes of Elderly Patients With Acute Myeloid Leukemia Receiving Standard Chemotherapy
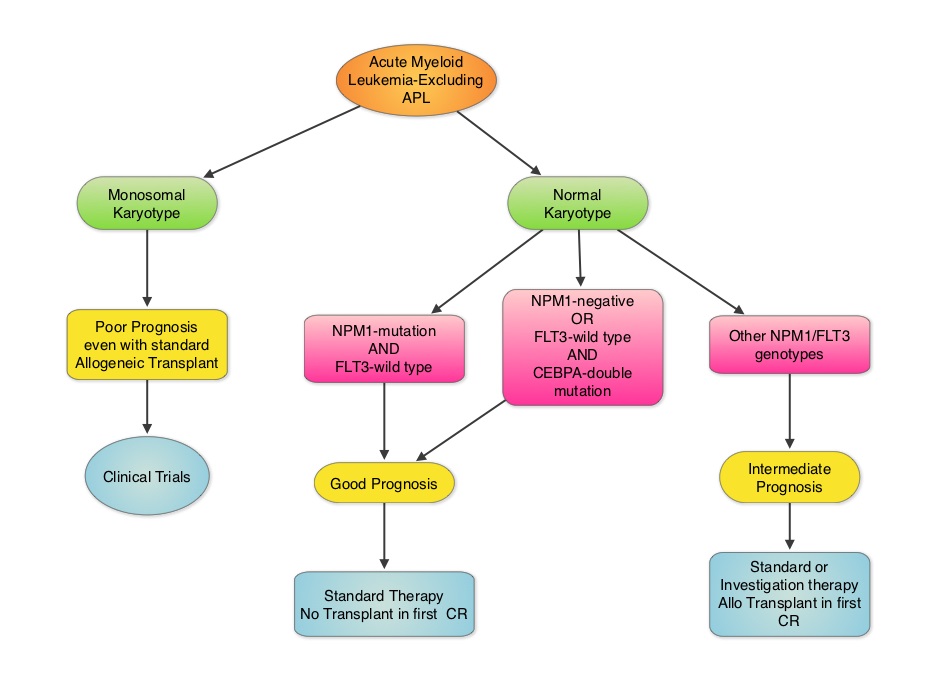
SUMMARY: Cytogenetic analysis has been part of routine evaluation when caring for patients with AML. By predicting resistance to therapy, cytogenetics stratify patients based on risk and helps manage them accordingly. Even though normal karyotype is the most common cytogenetic finding, approximately 10%-15% of AML patients have a monosomal karyotype (presence of at least 2 autosomal monosomies or a single autosomal monosomy in combination with at least one structural abnormality). These patients have a poor prognosis and alterations in the TP53 gene has been implicated in majority of these patients. AML patients with a normal karyotype should be tested for NPM1 (Nucleophosmin), FLT3 (Fms-related tyrosine kinase 3) and CEBPA (CCAAT/Enhancer Binding Protein Alpha) mutations, in addition to cytogenetics, as this may have therapeutic implications. CEBPA is a transcription factor and plays an important role in myeloid differentiation. Mutations in the CEBPA gene have been described in approximately 10% of patients with AML. Patients can have one or two mutations in this gene. It appears that favorable outcomes may be limited to those patients who have double CEBPA mutations rather than those with single CEBPA mutations. AML patients without FLT3 mutations or NPM1 mutation with CEBPA-double mutations have a favorable outcome. In this retrospective review, the authors analyzed the clinical impact of NPM1 and FLT3 mutations in AML patients, 65 years of age or older, treated with cytotoxic chemotherapy. A total of 557 patients were retrospectively reviewed. They noted that the outcomes were significantly better amongst patients with NPM1-mut/FLT3-wild type genotype compared to any other NPM1/FLT3 genotypes. The median survival was 21.5 months vs. 9.0 months and estimated 2-year survival rates were 51% vs. 38%, respectively (P = .003). The authors concluded that elderly AML patients with NPM1-mut/FLT3-wild type genotype have significantly improved outcomes when treated with cytotoxic chemotherapy. This subset of patients have a good prognosis with outcomes similar to those with favorable cytogenetics such as Inversion 16 and t(8:21). The discovery of molecular mutations is providing valuable information to facilitate risk-adapted therapy. Daver N, Liu Dumlao T, Ravandi F, et al. Clinical Lymphoma Myeloma and Leukemia 2013;13:435-440
Final Results of a Phase 2 Open-Label, Monotherapy Efficacy and Safety Study of Quizartinib (AC220) in Patients with FLT3-ITD Positive or Negative Relapsed/Refractory Acute Myeloid Leukemia After Second-Line Chemotherapy or Hematopoietic Stem Cell Transplantation
SUMMARY: FLT3-ITD (FMS-like tyrosine kinase 3 – Internal Tandem Duplications) mutations are seen in approximately a third of the patients with AML and are associated with early relapse and poor survival. Quizartinib is an oral tyrosine kinase inhibitor, which has demonstrated activity in patients with both wild type FLT3 as well as those with FLT3 mutations. In this phase II trial, 333 patients were enrolled and divided into 2 cohorts – patients older than 60 years and those between 18 and 60 years of age. The data presented here relates to cohort 2 (younger cohort) which included 137 patients with AML, who either relapsed or were refractory to second line chemotherapy or relapsed after hematopoietic stem cell transplantation (HSCT). Of these patients, 99 were FLT3 -ITD mutation positive and 38 were FLT3 wild type. The dose of Quizartinib was 90 mg/day for women and 135 mg/day for men and was given continuously in 28-day cycles. This dosing schedule was chosen because of the risk for QT interval prolongation, based on gender. The primary end point was a composite complete remission rate (CRc), which included complete remission, complete remission with incomplete platelet recovery (CRp) and complete remission with incomplete hematologic recovery (CRi). Patients with FLT3 mutations had a CRc of 44% with 4% CR and 40% CRi. The median duration of response was 11.3 weeks and the median overall survival was 23.1 weeks. This compared to a CRc of 34% for those with wild type FLT3. Thirty four percent (34%) of the patients were able to undergo HSCT following response to Quizartinib. The most common side effects included nausea, vomiting, QT prolongation, cytopenia, diarrhea and fatigue. The authors concluded that Quizartinib has significant activity in patients with resistant and refractory AML and can facilitate HCST in about a third of the treated patients. Levis MJ, Perl AE, Dombret H, et al. 54th ASH Annual Meeting and Exposition 2012, Abstract 673
Oncoprescribe Blog Prognosis in AML based on gene signature
Outcomes in Acute Myeloid Leukemia (AML) is dependent on age, FLT3 mutations and cytogenetics, that is, until now. A study published in the JAMA this month concluded that high expression of Leukemic Stem Cell (LSC) gene expression signature was independently associated with lower remission rates following induction chemotherapy, as well as inferior relapse free, event free and overall survival in patients with normal as well as abnormal karyotypic findings and was also independent of age and FLT3 mutations.
The LSC score will soon become a very important component for risk stratification in patients with AML