
SUMMARY:The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness. About 10-20% of the patients with liver metastases have resectable disease, which may translate into long term survival. CRC patients with synchronous metastases tend to have more extensive disease with bilobar liver involvement. With the availability of more effective chemotherapy regimens and targeted systemic interventions, the median survival of CRC patients with metastatic disease has increased from 6 months in the 1990’s to 24 months. Selective Internal Radiation Therapy (SIRT) or RadioEmbolization using radioisotope Yttrium-90 (Y-90) coated resin particles, a pure beta emitter, has demonstrated significant benefit for patients with unresectable liver metastases, in previously published studies. Y-90 resin microspheres are no bigger in diameter than a human hair and are introduced into the hepatic artery by initially accessing the femoral artery. The blood supply to the liver tumors is via the hepatic artery and these tumors tend to be hypervascular. The Y-90 resin microspheres become preferentially lodged in the narrow capillaries that surround liver tumors and selectively deliver a high dose of short-range beta radiation to the liver tumors. The physical properties of Y-90 resin microspheres facilitate even distribution of radioactivity within and around the liver metastases. SIRFLOX is an International, multi-center, open-label, randomized phase III study, which evaluated the efficacy and safety of combining modified FOLFOX6 (Oxaliplatin, 5-FU and Leucovorin) chemotherapy regimen with or without AVASTIN® (Bevacizumab) with SIRT, using Y-90 resin microspheres, as first line treatment in patients with unresectable liver only or liver dominant metastatic ColoRectal Cancer (mCRC). The randomization included 530 patients of whom 263 patients received mFOLFOX6 with or without AVASTIN® (Group A) and 267 patients received mFOLFOX6 + SIRT administered once with cycle 1, with or without AVASTIN® (Group B), with the treatment given until disease progression. Patients were stratified based on the extent of liver involvement (25% or less versus more than 25%), presence of extra hepatic disease (liver only versus liver dominant disease) and treatment with AVASTIN®, which was at the discretion of the attending physician. Forty percent of the patients had extra hepatic disease. The primary endpoint was Progression Free Survival (PFS). With a median follow up of 36.1 months, the median PFS in the liver was 12.6 months versus 20.5 months in Group A versus Group B respectively (HR=0.69; P=0.002). The hepatic Response Rate was 68.8% versus 78.7% (P=0.042), with a Complete Response Rate of 1.9% versus 6.0% (P=0.02) in Groups A and B respectively. Even though hematologic and gastrointestinal adverse events were higher in the SIRT group, the toxicity levels were acceptable. The authors concluded that the addition of SIRT to chemotherapy resulted in a 7.9 month improvement in Progression Free Survival in the liver, for patients with unresectable metastatic ColoRectal cancer (mCRC), with a 31% reduction in the risk of tumor progression in the liver. With the liver being the most common site of spread in patients with metastatic CRC, this study provides Level One evidence to support the use of SIRT in combination with chemotherapy in this patient group. SIRFLOX: Randomized phase III trial comparing first-line mFOLFOX6 ± bevacizumab (bev) versus mFOLFOX6 + selective internal radiation therapy (SIRT) ± bev in patients (pts) with metastatic colorectal cancer (mCRC). Gibbs P, Heinemann V, Sharma NK, et al. J Clin Oncol 33, 2015 (suppl; abstr 3502)</s
SIRFLOX is an International, multi-center, open-label, randomized phase III study, which evaluated the efficacy and safety of combining modified FOLFOX6 (Oxaliplatin, 5-FU and Leucovorin) chemotherapy regimen with or without AVASTIN® (Bevacizumab) with SIRT, using Y-90 resin microspheres, as first line treatment in patients with unresectable liver only or liver dominant metastatic ColoRectal Cancer (mCRC). The randomization included 530 patients of whom 263 patients received mFOLFOX6 with or without AVASTIN® (Group A) and 267 patients received mFOLFOX6 + SIRT administered once with cycle 1, with or without AVASTIN® (Group B), with the treatment given until disease progression. Patients were stratified based on the extent of liver involvement (25% or less versus more than 25%), presence of extra hepatic disease (liver only versus liver dominant disease) and treatment with AVASTIN®, which was at the discretion of the attending physician. Forty percent of the patients had extra hepatic disease. The primary endpoint was Progression Free Survival (PFS). With a median follow up of 36.1 months, the median PFS in the liver was 12.6 months versus 20.5 months in Group A versus Group B respectively (HR=0.69; P=0.002). The hepatic Response Rate was 68.8% versus 78.7% (P=0.042), with a Complete Response Rate of 1.9% versus 6.0% (P=0.02) in Groups A and B respectively. Even though hematologic and gastrointestinal adverse events were higher in the SIRT group, the toxicity levels were acceptable. The authors concluded that the addition of SIRT to chemotherapy resulted in a 7.9 month improvement in Progression Free Survival in the liver, for patients with unresectable metastatic ColoRectal cancer (mCRC), with a 31% reduction in the risk of tumor progression in the liver. With the liver being the most common site of spread in patients with metastatic CRC, this study provides Level One evidence to support the use of SIRT in combination with chemotherapy in this patient group. SIRFLOX: Randomized phase III trial comparing first-line mFOLFOX6 ± bevacizumab (bev) versus mFOLFOX6 + selective internal radiation therapy (SIRT) ± bev in patients (pts) with metastatic colorectal cancer (mCRC). Gibbs P, Heinemann V, Sharma NK, et al. J Clin Oncol 33, 2015 (suppl; abstr 3502)</s
Tag: Colon Cancer
Daily Aspirin May Improve Survival after Diagnosis of Colorectal Cancer
SUMMARY:The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. Several epidemiological studies as well as randomized controlled trials have shown that Aspirin reduces the incidence of ColoRectal Cancer (CRC) and CRC associated mortality. Platelets have long been implicated in the mechanism of tumor metastases. More recent data suggests that platelets may play a role in tumorigenesis as well, through the release of angiogenic and growth factors due to overexpression of COX-2. Daily low dose Aspirin inhibits COX-1 and COX-2.  It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties. Even though the benefits of Aspirin in the primary prevention of CRC remains well established, the role of Aspirin in secondary prevention in patients with CRC is unclear. The authors conducted this trial to evaluate the association between Aspirin use after diagnosis of CRC with CRC-Specific Survival (CSS) and Overall Survival (OS) in the largest group of patients ever studied. The study authors in this retrospective study identified 25,644 patients in the Cancer Registry of Norway, diagnosed with ColoRectal Cancer (CRC) from 2004 through 2011. Using the Norwegian Prescription Database, the authors were then able to establish that 6,109 patients in this large cohort had documented exposure to Aspirin. Exposure to Aspirin was defined as a prescription for more than 6 months of Aspirin following a diagnosis of CRC. The median follow up was 2.2 years. The authors performed a multivariate regression analysis controlling for age, gender, tumor stage, tumor differentiation and noted that exposure to Aspirin post-diagnosis, independently improved ColoRectal Cancer (CRC) -Specific Survival (HR=0.75; P<0.001) and Overall Survival (HR=0.86; P<0.001). The authors concluded that in this large group of unselected ColoRectal Cancer (CRC) patients, exposure to Aspirin after the diagnosis of CRC is independently associated with improved Colorectal Cancer-Specific Survival and Overall Survival. They added that because of the risk of bleeding, the risk–benefit should be assessed before Aspirin is routinely recommended to this patient population. Impact of aspirin as secondary prevention in an unselected cohort of 25,644 patients with colorectal cancer: A population-based study. Bains S, Mahic M, Cvancarova M, et al. J Clin Oncol 33, 2015 (suppl; abstr 3504)
It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties. Even though the benefits of Aspirin in the primary prevention of CRC remains well established, the role of Aspirin in secondary prevention in patients with CRC is unclear. The authors conducted this trial to evaluate the association between Aspirin use after diagnosis of CRC with CRC-Specific Survival (CSS) and Overall Survival (OS) in the largest group of patients ever studied. The study authors in this retrospective study identified 25,644 patients in the Cancer Registry of Norway, diagnosed with ColoRectal Cancer (CRC) from 2004 through 2011. Using the Norwegian Prescription Database, the authors were then able to establish that 6,109 patients in this large cohort had documented exposure to Aspirin. Exposure to Aspirin was defined as a prescription for more than 6 months of Aspirin following a diagnosis of CRC. The median follow up was 2.2 years. The authors performed a multivariate regression analysis controlling for age, gender, tumor stage, tumor differentiation and noted that exposure to Aspirin post-diagnosis, independently improved ColoRectal Cancer (CRC) -Specific Survival (HR=0.75; P<0.001) and Overall Survival (HR=0.86; P<0.001). The authors concluded that in this large group of unselected ColoRectal Cancer (CRC) patients, exposure to Aspirin after the diagnosis of CRC is independently associated with improved Colorectal Cancer-Specific Survival and Overall Survival. They added that because of the risk of bleeding, the risk–benefit should be assessed before Aspirin is routinely recommended to this patient population. Impact of aspirin as secondary prevention in an unselected cohort of 25,644 patients with colorectal cancer: A population-based study. Bains S, Mahic M, Cvancarova M, et al. J Clin Oncol 33, 2015 (suppl; abstr 3504)
CYRAMZA® (Ramucirumab)
The FDA on April 24, 2015 approved CYRAMZA® for use in combination with FOLFIRI for the treatment of patients with metastatic ColoRectal Cancer (mCRC), whose disease has progressed on a first line Bevacizumab, Oxaliplatin and Fluoropyrimidine containing regimen. CYRAMZA® is a recombinant human monoclonal IgG1 antibody that binds to the human vascular endothelial growth factor- receptor 2 (VEGF-R2), preventing the interaction of VEGF-R2 to its ligands. CYRAMZA® was approved earlier in 2014 for the treatment of patients with advanced Gastric or GastroEsophageal Junction (GEJ) adenocarcinoma and in December 2014, for use in combination with TAXOTERE® (Docetaxel) for the treatment of patients with metastatic Non Small Cell Lung Cancer (NSCLC). CYRAMZA® injection for intravenous infusion, is a product of Eli Lilly and Company.
FDA Approves CYRAMZA® for Metastatic ColoRectal Cancer
SUMMARY: The FDA on April 24, 2015 approved CYRAMZA® for use in combination with FOLFIRI for the treatment of patients with metastatic ColoRectal Cancer (mCRC), whose disease has progressed on a first line AVASTIN® (Bevacizumab), ELOXATIN® (Oxaliplatin) and Fluoropyrimidine containing regimen. The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. With the availability of new active agents for the treatment of CRC, improving Overall Survival for patients with advanced disease, by prudently planning a treatment strategy and properly sequencing these agents, has become increasing relevant. 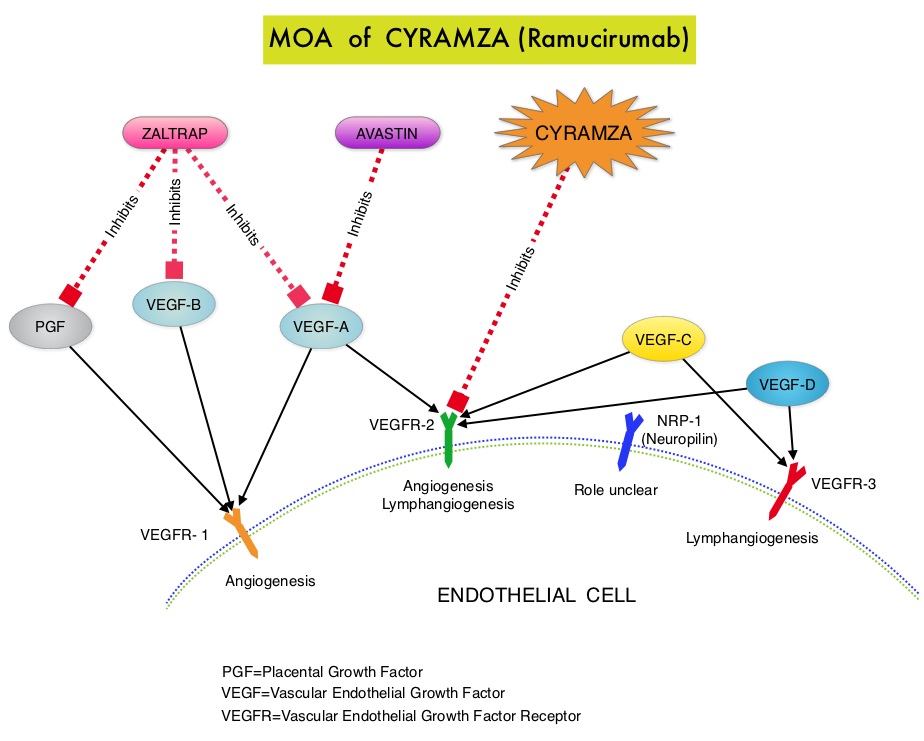 CYRAMZA® (Ramucirumab) is a recombinant human IgG1 monoclonal antibody that binds to Vascular Endothelial Growth Factor Receptor 2 (VEGFR-2) and blocks binding of the VEGFR ligands VEGF-A, VEGF-C, and VEGF-D and thus inhibits ligand-induced proliferation and migration of endothelial cells. This is unlike AVASTIN®, which inhibits VEGF-A. Several studies have demonstrated that continuing VEGF inhibition along with standard second-line chemotherapy beyond disease progression has a significant advantage, in patients with mCRC. Two observational studies (BRiTE and ARIES) as well as an open label phase III study have all shown improvement in median Overall Survival (OS) when AVASTIN® was continued beyond first progression and given along with second line chemotherapy. In the VELOUR trial, FOLFIRI in combination with ZALTRAP® (Aflibercept), a VEGF-A, VEGF-B and Placental Growth Factor inhibitor, when given as second line therapy for those patients with mCRC who had progressed on AVASTIN® plus ELOXATIN® containing regimen, resulted in a significant improvement in the median PFS and OS.
CYRAMZA® (Ramucirumab) is a recombinant human IgG1 monoclonal antibody that binds to Vascular Endothelial Growth Factor Receptor 2 (VEGFR-2) and blocks binding of the VEGFR ligands VEGF-A, VEGF-C, and VEGF-D and thus inhibits ligand-induced proliferation and migration of endothelial cells. This is unlike AVASTIN®, which inhibits VEGF-A. Several studies have demonstrated that continuing VEGF inhibition along with standard second-line chemotherapy beyond disease progression has a significant advantage, in patients with mCRC. Two observational studies (BRiTE and ARIES) as well as an open label phase III study have all shown improvement in median Overall Survival (OS) when AVASTIN® was continued beyond first progression and given along with second line chemotherapy. In the VELOUR trial, FOLFIRI in combination with ZALTRAP® (Aflibercept), a VEGF-A, VEGF-B and Placental Growth Factor inhibitor, when given as second line therapy for those patients with mCRC who had progressed on AVASTIN® plus ELOXATIN® containing regimen, resulted in a significant improvement in the median PFS and OS.
The RAISE trial is a double-blind, phase III study in which 1072 patients with mCRC who progressed on or after first-line treatment with AVASTIN®, ELOXATIN® and a Fluoropyrimidine were randomized to receive FOLFIRI given along with antiangiogenic agent CYRAMZA® (N = 536) or placebo (N = 536), every 2 weeks. The FOLFIRI regimen consisted of CAMPTOSAR® (Irinotecan) 180 mg/m2 IV, Folinic Acid 400 mg/m2 IV and 5-FU 400 mg/m2 IV bolus followed by 5-FU 2400 mg/m2 continuous IV infusion over 46 to 48 hours. CYRAMZA® was administered at a dose of 8 mg/kg IV every 2 weeks. The median age of patients was 62 years, about 50% harbored KRAS mutations and 99% of the patients had an ECOG performance status of 0 or 1. Treatment was continued until disease progression or unacceptable toxicity. The primary endpoint of the study was Overall Survival (OS) and secondary endpoints included Progression Free Survival (PFS), Objective Response Rate (ORR) and toxicity. There was a statistically significant Overall Survival improvement in patients receiving FOLFIRI plus CYRAMZA® compared to those receiving FOLFIRI plus placebo with a median OS of 13.3 and 11.7 months for patients on the FOLFIRI plus CYRAMZA® and FOLFIRI plus placebo arms, respectively (HR=0.85; P=0.023). The median PFS with FOLFIRI and CYRAMZA® was 5.7 months versus 4.5 months with FOLFIRI and placebo (HR= 0.79; P=0.001). There was no statistically significant difference in Objective Response Rate noted in the two treatment groups. Compared to the placebo group, more patients receiving CYRAMZA®, experienced grade 3 or more adverse events such as neutropenia (38.4% vs 23.3%) and hypertension (10.8% vs 2.8%). Other adverse events associated with CYRAMZA® included hemorrhage (43.9% vs 22.7% with placebo) and proteinuria (17% vs 4.5% with placebo). The authors concluded that CYRAMZA® is a new treatment option for second line treatment of patients with metastatic ColoRectal Cancer, including those with KRAS mutations. Tabernero J, Cohn AL, Obermannova R, et al. RAISE: A randomized, double-blind, multicenter phase III study of irinotecan, folinic acid, and 5-fluorouracil (FOLFIRI) plus ramucirumab (RAM) or placebo (PBO) in patients (pts) with metastatic colorectal carcinoma (CRC) progressive during or following first-line combination therapy with bevacizumab (bev), oxaliplatin (ox), and a fluoropyrimidine (fp). 2015 Gastrointestinal Cancers Symposium; January 15-17, 2015; San Francisco, CA. Abstract 512.
Higher Serum Vitamin D Levels May Improve Survival in Patients with Advanced Colon Cancer
SUMMARY: The American Cancer Society estimates that approximately 133,000 new cases of colorectal cancer will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. There is a growing body of evidence suggesting that Vitamin D has colon cancer preventing properties and may induce antitumor immunity. A recent study by Song and colleagues (Gut. 2015;64:260-271) showed that high plasma level 25-Hydroxy Vitamin D [25(OH)D] was associated with lower risk of colorectal cancer with intense immune reaction, supporting that vitamin D through tumor-host interaction may play a role in cancer immunoprevention.  There appears to be a strong association between plasma 25(OH)D level and colorectal cancer (CRC) specific mortality, with better outcomes in patients with Stage I-III CRC, who had higher plasma levels of 25(OH)D (Zgaga L, et al. J Clin Oncol 2014;32:2430-2439). The researchers in this present study conducted a prospective analysis of data from CALGB 80405 trial and evaluated the relationship between plasma 25(OH)D level and patient outcomes, which included Overall Survival and Progression Free Survival (PFS). CALGB 80405 is a phase III trial in which patients with newly diagnosed, advanced colorectal cancer were initially randomized to three groups- 1) Chemotherapy (FOLFIRI or mFOLFOX6) with ERBITUX® (Cetuximab) 2) Chemotherapy with AVASTIN® (Bevacizumab) 3) Chemotherapy with ERBITUX® and AVASTIN®. The protocol was later amended to only include patients with KRAS Wild Type tumors and the chemotherapy with ERBITUX® and AVASTIN® group was deleted. This trial was not designed to compare chemotherapy regimens. The Overall Survival (OS) in both the treatment groups were similar at 29+ months.
There appears to be a strong association between plasma 25(OH)D level and colorectal cancer (CRC) specific mortality, with better outcomes in patients with Stage I-III CRC, who had higher plasma levels of 25(OH)D (Zgaga L, et al. J Clin Oncol 2014;32:2430-2439). The researchers in this present study conducted a prospective analysis of data from CALGB 80405 trial and evaluated the relationship between plasma 25(OH)D level and patient outcomes, which included Overall Survival and Progression Free Survival (PFS). CALGB 80405 is a phase III trial in which patients with newly diagnosed, advanced colorectal cancer were initially randomized to three groups- 1) Chemotherapy (FOLFIRI or mFOLFOX6) with ERBITUX® (Cetuximab) 2) Chemotherapy with AVASTIN® (Bevacizumab) 3) Chemotherapy with ERBITUX® and AVASTIN®. The protocol was later amended to only include patients with KRAS Wild Type tumors and the chemotherapy with ERBITUX® and AVASTIN® group was deleted. This trial was not designed to compare chemotherapy regimens. The Overall Survival (OS) in both the treatment groups were similar at 29+ months.
In the present study, plasma 25(OH)D level were measured at baseline in 1,043 patients at the time of their enrollment in CALGB 80405, and dietary and lifestyle behaviors were collected from self-administered questionnaires. The median plasma 25(OH)D level was 17.2 ng/mL, with the range varying from 2.2 to 72.7 ng/mL (recommended range is 20-30 ng/mL). Factors associated with lower 25(OH)D level included older age, black race, lower dietary and supplemental vitamin D intake, higher Body Mass Index (BMI), ECOG performance status of 1 versus 0 and lower physical activity. Additionally, patients whose blood specimens were drawn in the winter and spring months had significantly lower 25(OH)D level, as did patients who were from the Northern and Northeastern parts of the United States. Vitamin D supplement use was uncommon in this patient population. After adjusting for pathologic and clinical prognostic factors, patients in the group with the highest level of 25(OH)D had significantly improved median OS compared to those in the group with the lowest level (32.6 vs 24.5 months; HR=0.67, P trend 0.002). Higher level of 25(OH)D was also associated with improved PFS (median 12.2 vs 10.1 months; HR 0.80, P trend = 0.02). These results were consistent across all subgroups of patients. The authors concluded that higher plasma level of 25(OH)D was associated with significantly improved survival in metastatic CRC patients treated with a combination of chemotherapy and biologic agents. With 30-35% of the malignancies attributed to dietary habits, the onus is therefore on the treating physicians to provide nutrition counseling during and after cancer treatment. Recommending vitamin D supplements for those patients with colon cancer with low vitamin D levels, may therefore not be unreasonable. Vitamin D status and survival of metastatic colorectal cancer patients: Results from CALGB/SWOG 80405 (Alliance). Ng K, Venook AP, Sato K, et al. J Clin Oncol 33, 2015 (suppl 3; abstr 507)
Pre- and Post-diagnosis Physical Activity, Television Viewing, and Mortality Among Patients With Colorectal Cancer in the National Institutes of Health–AARP Diet and Health Study
SUMMARY:The American Cancer Society estimates that approximately 137,000 new cases of colorectal cancer were diagnosed in the United States in 2014 and over 50,000 died of the disease. Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable. Standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival and Overall Survival. Reducing risk of death and improving survival even further with leisure time physical activity is the topic of this discussion. The most prevalent sedentary behavior, watching TV, has been associated with poorer survival in the general population. Several studies have suggested protective effects of physical activity on cancer recurrence although this has not been conclusive. Pooled data from other studies have shown that lack of physical activity among survivors of ColoRectal Cancer (CRC) has been associated with higher mortality risk. However, the independent effects of physical activity before and after colorectal cancer diagnosis, has remained unclear and the association between watching TV and mortality in survivors of CRC has not been defined. There are several biologic mechanisms that explain the association between sedentary life style, physical activity, and mortality. The adipose tissue in the body in addition to serving as the storage site for energy also releases adipokines, which have pro-inflammatory and anti-inflammatory properties. Physical activity decreases inflammatory adipocytokines and increases anti-inflammatory cytokines and thereby could affect cancer incidence and mortality. Also, physical activity has been shown to increase insulin sensitivity. Several studies have shown increased risk of CRC, increased angiogenesis, tumor growth, and anti-apoptotic activity with higher circulating insulin and insulin-like growth factor-1 and lower insulin-binding protein levels. Physical activity also improves cardiovascular health by lowering blood pressure. The authors in this study explored the impact of lifestyle such as moderate to vigorous intensity physical activity level and TV viewing time (sedentary life style) on ColoRectal Cancer mortality among CRC survivors, with particular attention to pre and post cancer diagnosis contributing factors. Data was collected from a large cohort of patients enrolled in the National Institutes of Health Diet and Health Study and the associations were analyzed between pre CRC diagnosis (N=3797) and post CRC diagnosis (N= 1759) life styles (physical activity and TV watching) and overall and disease-specific mortality. It was noted that patients who had 7 or more hours of weekly leisure physical activity before their diagnosis of CRC had a 20% lower risk of all-cause mortality compared to those who had a sedentary life style and were not engaged in any leisure time activity (HR=0.80; P=0.02). Patients who were engaged in 7 or more hours of weekly leisure physical activity post CRC diagnosis had a 31% lower risk of all-cause mortality compared to those who reported no activity (HR=0.69; P=0.006). This benefit was noted independent of pre-diagnosis activity. Amongst those who reported sedentary lifestyle, patients who spent 5 or more TV hours per day before CRC diagnosis had a 22% increased risk in all-cause mortality compared to those who watched no more than 2 hours of TV per day (HR=1.22; P=0.002). A similar trend of increased risk of all-cause mortality was seen in those who spent more TV hours, post diagnosis although this was not statistically significant. The authors concluded that in patients with CRC, leisure time physical activity was inversely associated with all-cause mortality, whereas more TV hours was associated with increased mortality risk. Health Care providers should therefore proactively promote increasing physical activity and minimizing TV hours, among survivors of ColoRectal Cancer. Arem H, Pfeiffer RM, Engels EA, et al. J Clin Oncol 2015; 33:180-188
There are several biologic mechanisms that explain the association between sedentary life style, physical activity, and mortality. The adipose tissue in the body in addition to serving as the storage site for energy also releases adipokines, which have pro-inflammatory and anti-inflammatory properties. Physical activity decreases inflammatory adipocytokines and increases anti-inflammatory cytokines and thereby could affect cancer incidence and mortality. Also, physical activity has been shown to increase insulin sensitivity. Several studies have shown increased risk of CRC, increased angiogenesis, tumor growth, and anti-apoptotic activity with higher circulating insulin and insulin-like growth factor-1 and lower insulin-binding protein levels. Physical activity also improves cardiovascular health by lowering blood pressure. The authors in this study explored the impact of lifestyle such as moderate to vigorous intensity physical activity level and TV viewing time (sedentary life style) on ColoRectal Cancer mortality among CRC survivors, with particular attention to pre and post cancer diagnosis contributing factors. Data was collected from a large cohort of patients enrolled in the National Institutes of Health Diet and Health Study and the associations were analyzed between pre CRC diagnosis (N=3797) and post CRC diagnosis (N= 1759) life styles (physical activity and TV watching) and overall and disease-specific mortality. It was noted that patients who had 7 or more hours of weekly leisure physical activity before their diagnosis of CRC had a 20% lower risk of all-cause mortality compared to those who had a sedentary life style and were not engaged in any leisure time activity (HR=0.80; P=0.02). Patients who were engaged in 7 or more hours of weekly leisure physical activity post CRC diagnosis had a 31% lower risk of all-cause mortality compared to those who reported no activity (HR=0.69; P=0.006). This benefit was noted independent of pre-diagnosis activity. Amongst those who reported sedentary lifestyle, patients who spent 5 or more TV hours per day before CRC diagnosis had a 22% increased risk in all-cause mortality compared to those who watched no more than 2 hours of TV per day (HR=1.22; P=0.002). A similar trend of increased risk of all-cause mortality was seen in those who spent more TV hours, post diagnosis although this was not statistically significant. The authors concluded that in patients with CRC, leisure time physical activity was inversely associated with all-cause mortality, whereas more TV hours was associated with increased mortality risk. Health Care providers should therefore proactively promote increasing physical activity and minimizing TV hours, among survivors of ColoRectal Cancer. Arem H, Pfeiffer RM, Engels EA, et al. J Clin Oncol 2015; 33:180-188
Statin Use After Colorectal Cancer Diagnosis and Survival A Population-Based Cohort Study
SUMMARY: Approximately 32 million Americans take a statin in the United States. Statins (3-Hydroxy-3-MethylGlutaryl coenzyme A reductase inhibitors) are usually prescribed to lower LDL cholesterol. Cholesterol is a structural component of cell membranes and a reduction in the availability of cholesterol can result in decreased proliferation and migration of cancer cells. The six statin drugs available in the United States include LIPITOR® (Atorvastatin), ZOCOR® (Simvastatin), CRESTOR® (Rosuvastatin), MEVACOR® (Lovastatin), PRAVACHOL® (Pravastatin) and LESCOL® (Fluvastatin). 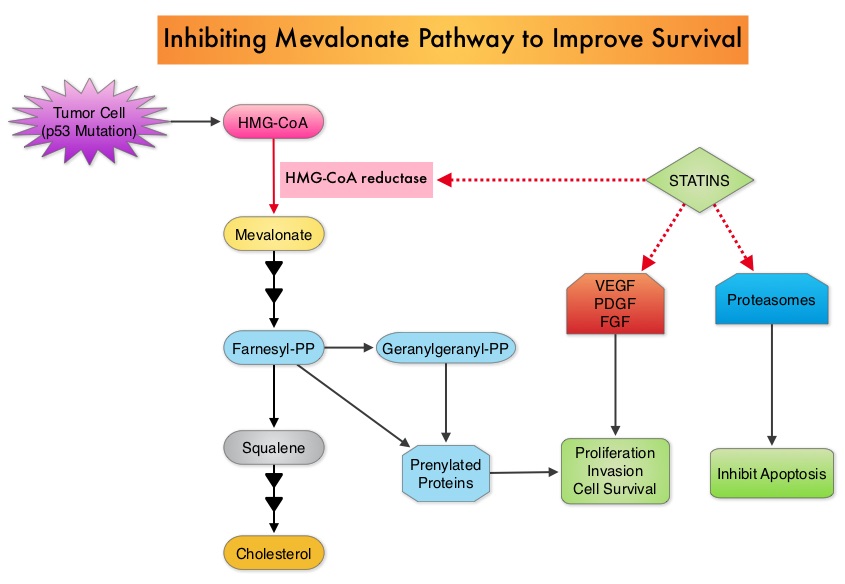 Statin use in cancer patients has been associated with a reduction in cancer related mortality in several clinical studies. This benefit has been attributed to the inhibition of HMG-CoA reductase, which is a rate limiting enzyme in the mevalonate and cholesterol synthesis pathway. The mevalonate pathway is upregulated by mutated p53 (tumor suppressor gene) which is often expressed in cancer cells. By inhibiting the mevalonate pathway, statins can reduce isoprenoid levels such as farnesylpyrophosphate (F-PP) and geranylgeranylpyrophosphate (GG-PP). These isoprenoids are essential for the posttranslational modification of several proteins involved in important intracellular signaling pathways and therefore play a crucial role in cell growth, proliferation, survival and migration. Statins also inhibit angiogenic pathways and proteasomes, thereby negatively impacting cell proliferation and survival. Survival benefit with statin use after colorectal cancer diagnosis has been unclear. To answer this question, the authors identified a cohort of patients (N=7657) diagnosed with stage I to III colorectal cancer from 1998 to 2009, in the National Cancer Data Repository (English Cancer Registry). Information on statin use was obtained from medical records of patients and in this cohort of patients 35% were identified to have used statin drugs following diagnosis of colorectal cancer. Twenty percent of these patients had stage I disease, 43% had stage II disease and 37% had stage III disease. Patients were followed up for 14 years following their diagnosis of colorectal cancer. Statin use after a diagnosis of colorectal cancer was associated with a 29% reduction in colorectal cancer-specific mortality (HR= 0.71). There was a dose-response association with a 36% reduction in colorectal cancer-specific mortality with statin use for more than 1 year (HR=0.64). Statin users after colorectal cancer diagnosis also had a 25% reduction in all-cause mortality (HR=0.75). The authors concluded that based on this large population based colorectal cancer cohort, statin use following diagnosis of colorectal cancer was associated with longer rates of survival. Cardwell CR, Hicks BM, Hughes C, et al. J Clin Oncol 2014;32:3177-3183
Statin use in cancer patients has been associated with a reduction in cancer related mortality in several clinical studies. This benefit has been attributed to the inhibition of HMG-CoA reductase, which is a rate limiting enzyme in the mevalonate and cholesterol synthesis pathway. The mevalonate pathway is upregulated by mutated p53 (tumor suppressor gene) which is often expressed in cancer cells. By inhibiting the mevalonate pathway, statins can reduce isoprenoid levels such as farnesylpyrophosphate (F-PP) and geranylgeranylpyrophosphate (GG-PP). These isoprenoids are essential for the posttranslational modification of several proteins involved in important intracellular signaling pathways and therefore play a crucial role in cell growth, proliferation, survival and migration. Statins also inhibit angiogenic pathways and proteasomes, thereby negatively impacting cell proliferation and survival. Survival benefit with statin use after colorectal cancer diagnosis has been unclear. To answer this question, the authors identified a cohort of patients (N=7657) diagnosed with stage I to III colorectal cancer from 1998 to 2009, in the National Cancer Data Repository (English Cancer Registry). Information on statin use was obtained from medical records of patients and in this cohort of patients 35% were identified to have used statin drugs following diagnosis of colorectal cancer. Twenty percent of these patients had stage I disease, 43% had stage II disease and 37% had stage III disease. Patients were followed up for 14 years following their diagnosis of colorectal cancer. Statin use after a diagnosis of colorectal cancer was associated with a 29% reduction in colorectal cancer-specific mortality (HR= 0.71). There was a dose-response association with a 36% reduction in colorectal cancer-specific mortality with statin use for more than 1 year (HR=0.64). Statin users after colorectal cancer diagnosis also had a 25% reduction in all-cause mortality (HR=0.75). The authors concluded that based on this large population based colorectal cancer cohort, statin use following diagnosis of colorectal cancer was associated with longer rates of survival. Cardwell CR, Hicks BM, Hughes C, et al. J Clin Oncol 2014;32:3177-3183
CALGB/SWOG 80405 Phase III trial of irinotecan/5-FU/leucovorin (FOLFIRI) or oxaliplatin/5-FU/leucovorin (mFOLFOX6) with bevacizumab (BV) or cetuximab (CET) for patients (pts) with KRAS wild-type (wt) untreated metastatic adenocarcinoma of the colon or rectum (MCRC)
SUMMARY: The American Cancer Society estimates that approximately 137,000 new cases of colorectal cancer will be diagnosed in the United States in 2014 and over 50,000 are expected to die of the disease. Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable. Standard chemotherapy when combined with anti EGFR (Epidermal Growth Factor Receptor) targeted monoclonal antibodies such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab) as well as anti VEGF agent AVASTIN® (Bevacizumab), have demonstrated improvement in Progression Free Survival and Overall Survival.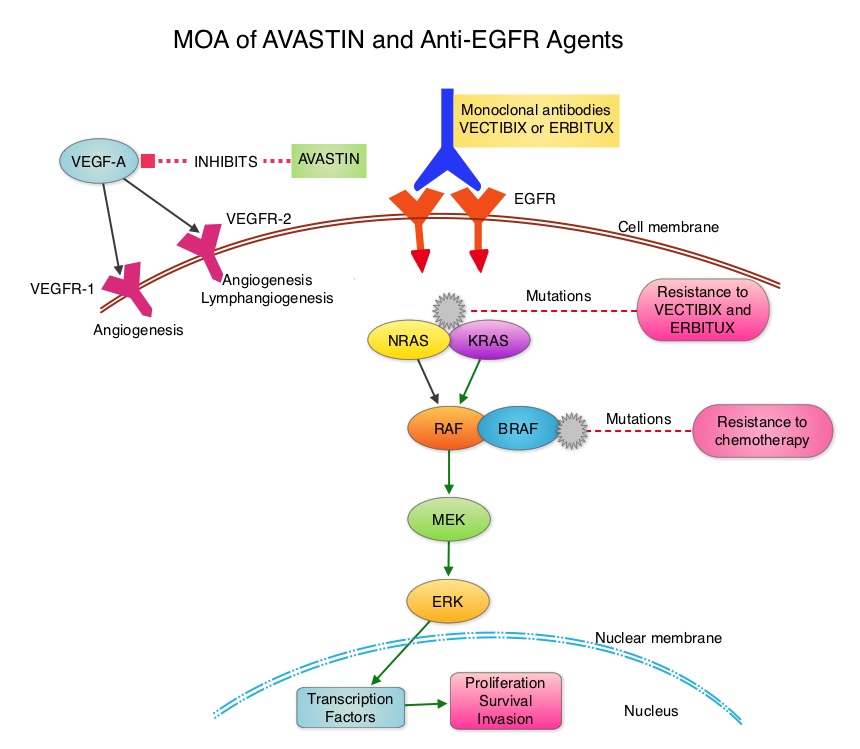 The benefit with anti EGFR agents however is only demonstrable in patients with metastatic colon cancer, whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now becoming clear that even amongst the KRAS Wild Type patient groups, about 15% to 20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Therefore, pan RAS (expanded RAS) testing may become relevant. To determine the optimal combination treatment regimen, this phase III intergroup trial evaluated the addition of ERBITUX® or AVASTIN® to physician’s choice of standard first line chemotherapy such as FOLFIRI or mFOLFOX6. Even though the original study included unselected metastatic colorectal cancer patients and randomization to a third arm (combination of ERBITUX® and AVASTIN®), this study was amended to include only pts with KRAS Wild Type tumors and the combination ERBITUX® and AVASTIN® arm was deleted. Patients were randomized to either ERBITUX® 400 mg/m2 week one and then 250 mg/m2, weekly or AVASTIN® 5 mg/kg every 2 weeks given along with FOLFIRI or mFOLFOX6 chemotherapy (physicians choice at the time of enrollment). The median age was 59 years and treatment groups were Chemo plus AVASTIN® (N=559) and Chemo plus ERBITUX® (N=578). Approximately 27% of the patients received FOLFIRI chemotherapy regimen and 76% received mFOLFOX6 chemotherapy regimen. Treatment was given until disease progression and median follow up was 24 months. The primary endpoint was Overall Survival. The median Overall Survival was similar in the ERBITUX® combination and the AVASTIN® combination groups (about 29 months) and so was the Progression Free Survival in both groups (about 10.5 months). The chemotherapy used with either of the antibodies had no influence on the outcomes. The toxicity profiles were different as expected, with increased incidence of Grade 3-4 rash (7% versus 0%) and diarrhea (11% versus 8%), in the ERBITUX® group and increased incidence of Grade 3-4 hypertension (7% versus 1%) and gastrointestinal events (2% versus 0.5%), in the AVASTIN® group. The authors concluded that either ERBITUX® or AVASTIN® in combination with chemotherapy have equivalent overall survival benefit, when given as first line therapy, for patients with metastatic colorectal cancer, whose tumors are KRAS Wild Type. It remains to be seen however, if pan RAS (expanded RAS) testing and other molecular studies will identify subsets of patients who will benefit from specific antibody chemotherapy combination regimens. Venook AP, Niedzwiecki D, Lenz H, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA3)
The benefit with anti EGFR agents however is only demonstrable in patients with metastatic colon cancer, whose tumors do not harbor KRAS mutations in codons 12 and 13 of exon 2 (KRAS Wild Type). It is now becoming clear that even amongst the KRAS Wild Type patient groups, about 15% to 20% have other rare mutations such as NRAS and BRAF mutations, which confer resistance to anti EGFR agents. Therefore, pan RAS (expanded RAS) testing may become relevant. To determine the optimal combination treatment regimen, this phase III intergroup trial evaluated the addition of ERBITUX® or AVASTIN® to physician’s choice of standard first line chemotherapy such as FOLFIRI or mFOLFOX6. Even though the original study included unselected metastatic colorectal cancer patients and randomization to a third arm (combination of ERBITUX® and AVASTIN®), this study was amended to include only pts with KRAS Wild Type tumors and the combination ERBITUX® and AVASTIN® arm was deleted. Patients were randomized to either ERBITUX® 400 mg/m2 week one and then 250 mg/m2, weekly or AVASTIN® 5 mg/kg every 2 weeks given along with FOLFIRI or mFOLFOX6 chemotherapy (physicians choice at the time of enrollment). The median age was 59 years and treatment groups were Chemo plus AVASTIN® (N=559) and Chemo plus ERBITUX® (N=578). Approximately 27% of the patients received FOLFIRI chemotherapy regimen and 76% received mFOLFOX6 chemotherapy regimen. Treatment was given until disease progression and median follow up was 24 months. The primary endpoint was Overall Survival. The median Overall Survival was similar in the ERBITUX® combination and the AVASTIN® combination groups (about 29 months) and so was the Progression Free Survival in both groups (about 10.5 months). The chemotherapy used with either of the antibodies had no influence on the outcomes. The toxicity profiles were different as expected, with increased incidence of Grade 3-4 rash (7% versus 0%) and diarrhea (11% versus 8%), in the ERBITUX® group and increased incidence of Grade 3-4 hypertension (7% versus 1%) and gastrointestinal events (2% versus 0.5%), in the AVASTIN® group. The authors concluded that either ERBITUX® or AVASTIN® in combination with chemotherapy have equivalent overall survival benefit, when given as first line therapy, for patients with metastatic colorectal cancer, whose tumors are KRAS Wild Type. It remains to be seen however, if pan RAS (expanded RAS) testing and other molecular studies will identify subsets of patients who will benefit from specific antibody chemotherapy combination regimens. Venook AP, Niedzwiecki D, Lenz H, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA3)
Multitarget Stool DNA Testing for Colorectal-Cancer Screening
SUMMARY: The American Cancer Society estimates that approximately 137,000 new cases of colorectal cancer will be diagnosed in the United States in 2014 and over 50,000 are expected to die of the disease. It is the third leading cause of cancer death in the U.S. and the lifetime risk of developing colorectal cancer is 1 in 20. Implementation of screening programs in the U.S. has resulted in a 46% decrease in the rate of death from colorectal cancer, from its peak. The U.S. Preventive Services Task Force recommends annual screening with high sensitivity Fecal Occult Blood Testing (FOBT), sigmoidoscopy every 5 years with high-sensitivity FOBT every 3 years and screening colonoscopy every 10 years. Fecal Immunochemical testing (FIT) measures intact human globin protein as opposed to heme. Animal heme from meat will not trigger a false positive test with FIT and as such dietary restrictions are not necessary. Further, FIT is superior to FOBT in detecting advanced adenomas and only requires one stool specimen, as opposed to three specimens for FOBT.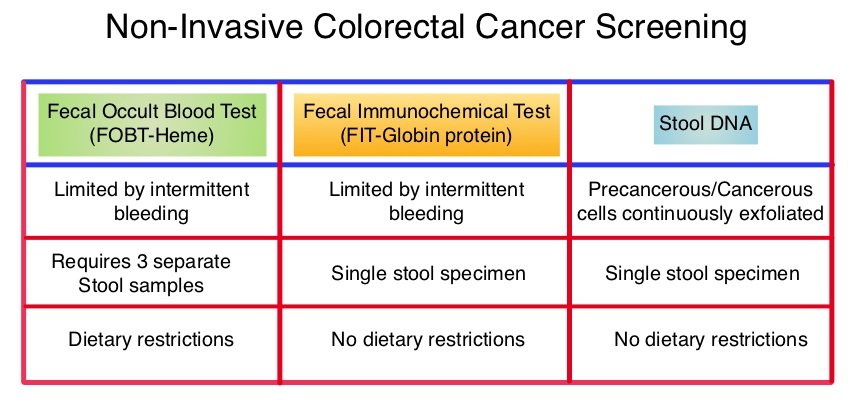 COLOGUARD® is highly sensitive, noninvasive, multitarget, stool based DNA test, for colorectal cancer screening ie.early detection of colorectal cancer and precancerous lesions. This test takes advantage of the genetic and epigenetic alterations that leads to the development of colorectal cancer and analyzes the altered DNA signatures of cancerous and precancerous cells that exfoliate into the colon. In addition, this test includes an immunochemical assay for human hemoglobin. The stool samples can be easily collected, mailed from home, and requires no bowel preparation, medication restrictions or dietary change. The purpose of this study was to determine the sensitivity of COLOGUARD® as compared with FIT, for the detection of screening-relevant colorectal cancer. The study was conducted at 90 medical centers throughout the United States and Canada and evaluable patients (N=9989) were asymptomatic individuals between ages 50 and 84 years who were required to provide a stool sample and undergo screening colonoscopy within 90 days. Enrollment was weighted toward those aged 65 years or older. The primary outcome was the ability of COLOGUARD® to detect colorectal cancer and secondary outcomes were the ability of COLOGUARD® to detect advanced precancerous lesions, polyps with high grade dysplasia and serrated sessile polyps measuring 1 cm or more, when compared to FIT. (Sensitivity is defined as the proportion of persons with disease who have a positive test and Specificity is defined as proportion of persons without disease who have a negative test.) The sensitivity for detecting colorectal cancer was 92% with COLOGUARD® and 74% with FIT (P=0.002). The sensitivity for detecting advanced precancerous lesions was 42.4% vs 23.8% (P<0.001), polyps with high-grade dysplasia was 69.2% vs 46.2% (P=0.004) and serrated sessile polyps measuring 1 cm or more were 42.4% vs 5.1%, (P<0.001) with COLOGUARD® and FIT respectively. Specificities with COLOGUARD® were lower compared to FIT (P<0.001). The authors concluded that COLOGUARD® can detect significantly more colorectal cancers and precancerous lesions than FIT. The high sensitivity of this non-invasive, stool DNA test, to detect curable stage of colorectal cancer, may increase the number of people, who will choose to be screened for colorectal cancer. Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. N Engl J Med 2014; 370:1287-1297
COLOGUARD® is highly sensitive, noninvasive, multitarget, stool based DNA test, for colorectal cancer screening ie.early detection of colorectal cancer and precancerous lesions. This test takes advantage of the genetic and epigenetic alterations that leads to the development of colorectal cancer and analyzes the altered DNA signatures of cancerous and precancerous cells that exfoliate into the colon. In addition, this test includes an immunochemical assay for human hemoglobin. The stool samples can be easily collected, mailed from home, and requires no bowel preparation, medication restrictions or dietary change. The purpose of this study was to determine the sensitivity of COLOGUARD® as compared with FIT, for the detection of screening-relevant colorectal cancer. The study was conducted at 90 medical centers throughout the United States and Canada and evaluable patients (N=9989) were asymptomatic individuals between ages 50 and 84 years who were required to provide a stool sample and undergo screening colonoscopy within 90 days. Enrollment was weighted toward those aged 65 years or older. The primary outcome was the ability of COLOGUARD® to detect colorectal cancer and secondary outcomes were the ability of COLOGUARD® to detect advanced precancerous lesions, polyps with high grade dysplasia and serrated sessile polyps measuring 1 cm or more, when compared to FIT. (Sensitivity is defined as the proportion of persons with disease who have a positive test and Specificity is defined as proportion of persons without disease who have a negative test.) The sensitivity for detecting colorectal cancer was 92% with COLOGUARD® and 74% with FIT (P=0.002). The sensitivity for detecting advanced precancerous lesions was 42.4% vs 23.8% (P<0.001), polyps with high-grade dysplasia was 69.2% vs 46.2% (P=0.004) and serrated sessile polyps measuring 1 cm or more were 42.4% vs 5.1%, (P<0.001) with COLOGUARD® and FIT respectively. Specificities with COLOGUARD® were lower compared to FIT (P<0.001). The authors concluded that COLOGUARD® can detect significantly more colorectal cancers and precancerous lesions than FIT. The high sensitivity of this non-invasive, stool DNA test, to detect curable stage of colorectal cancer, may increase the number of people, who will choose to be screened for colorectal cancer. Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. N Engl J Med 2014; 370:1287-1297
Analysis of KRAS/NRAS mutations in phase 3 study 20050181 of panitumumab (pmab) plus FOLFIRI versus FOLFIRI for second-line treatment (tx) of metastatic colorectal cancer (mCRC)
SUMMARY: It is estimated that approximately 97,000 new cases of colon cancer will be diagnosed in 2014 and over 50,000 will die of the disease. The lifetime risk of developing colorectal cancer is about 1 in 20. Even though colon cancer localized to the bowel is potentially curable with surgery and adjuvant chemotherapy, advanced colon cancer is often incurable. Multi agent chemotherapy in combination with monoclonal antibodies, targeted against Epidermal Growth Factor Receptor (EGFR) such as VECTIBIX® (Panitumumab) and ERBITUX® (Cetuximab), have demonstrated survival benefit, for patients with metastatic colon cancer, whose tumors do not harbor KRAS mutations in exon 2. The authors in this study evaluated the benefit of testing metastatic colorectal cancer tumors for RAS mutations beyond the mutations in the KRAS gene at exon 2.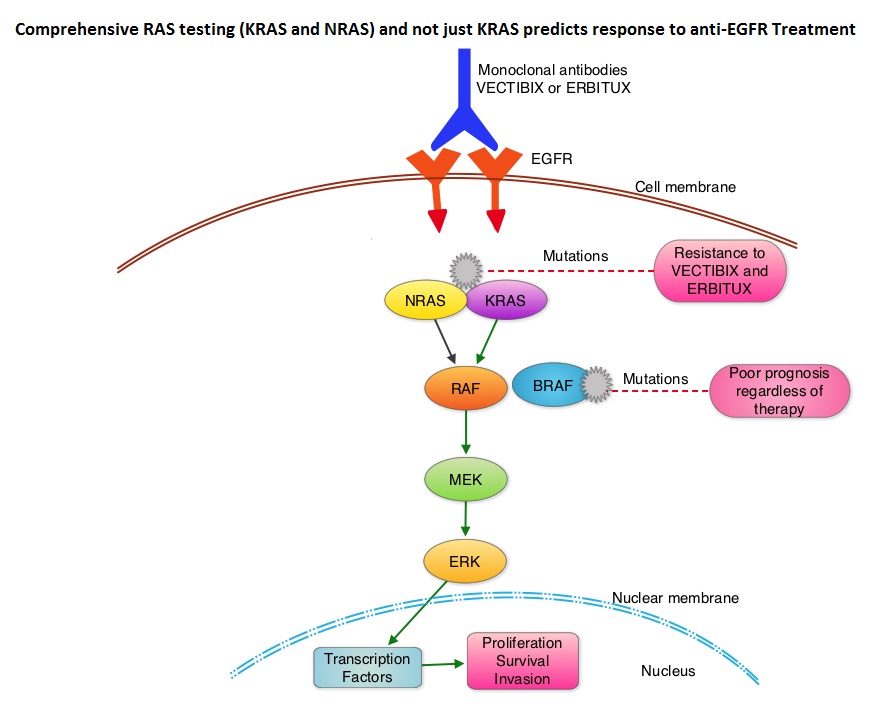 The most common RAS oncogenes in human cancer are HRAS, KRAS, and NRAS. Mutations in HRAS are not common in colon cancer whereas KRAS and NRAS mutations are seen in colon cancer and tend to be mutually exclusive. Activating mutations in exon 2 of the KRAS gene is seen in about 40% of colon cancer patients and predicts resistance to EGFR therapy. Mutational analysis is therefore usually performed to look for mutations in exon 2 of the KRAS gene. It appears however that a broader assessment of the RAS genes may more accurately predict resistance to EGFR therapy. It is also known that mutations in BRAF gene, which is downstream from RAS, may confer poor prognosis in colon cancer, regardless of therapy. The authors in a previous publication showed that in a phase III study involving 1,186 patients, the addition of VECTIBIX®, a fully human, EGFR targeted, monoclonal antibody, when combined with FOLFIRI (Folinic acid, Fluorouracil and Irinotecan), significantly improved Progression Free Survival, when compared to FOLFIRI alone (HR=0.73; P=0.004), with a trend towards improved Overall Survival (HR=0.85; P=0.12). Evolving data has suggested that testing for additional mutations in the RAS genes may help better understand the efficacy of/resistance to VECTIBIX®. In this present analysis, tumor samples of patients from the authors previous study, that were already known to be Wild Type KRAS – unmutated at KRAS exon 2 (N=597), were assessed for additional RAS mutations, specifically in KRAS exons 3 and 4 and NRAS exons 2, 3 and 4. Eighteen percent (18%) of the Wild Type KRAS exon 2 patients harbored additional RAS mutations. It was noted that patients receiving VECTIBIX® along with FOLFIRI had an improvement in both the median OS and PFS when they had wild-type (unmutated) RAS tumors compared to those, whose tumors harbored RAS mutations (median OS: 16.2 vs 11.8 months; median PFS: 6.4 vs 4.8 months). More importantly, amongst patients with mutated RAS tumors, the addition of VECTIBIX® to FOLFIRI resulted in no significant survival benefit compared to FOLFIRI alone (median OS: 11.8 vs 11.1 months; median PFS: 4.8 vs 4.0 months). The authors concluded that comprehensive RAS mutational analysis rather than KRAS testing alone, gives more relevant information for proper selection of patients with metastatic colorectal cancer, who would benefit from EGFR targeted monoclonal antibodies such as VECTIBIX®. In addition patients with RAS mutations could be spared from the associated cost and toxicites of EGFR targeted monoclonal antibodies that will not improve their outcomes. Peeters M, Oliner KS, Price TJ, et al. J Clin Oncol 32, 2014 (suppl 3; abstr LBA387)
The most common RAS oncogenes in human cancer are HRAS, KRAS, and NRAS. Mutations in HRAS are not common in colon cancer whereas KRAS and NRAS mutations are seen in colon cancer and tend to be mutually exclusive. Activating mutations in exon 2 of the KRAS gene is seen in about 40% of colon cancer patients and predicts resistance to EGFR therapy. Mutational analysis is therefore usually performed to look for mutations in exon 2 of the KRAS gene. It appears however that a broader assessment of the RAS genes may more accurately predict resistance to EGFR therapy. It is also known that mutations in BRAF gene, which is downstream from RAS, may confer poor prognosis in colon cancer, regardless of therapy. The authors in a previous publication showed that in a phase III study involving 1,186 patients, the addition of VECTIBIX®, a fully human, EGFR targeted, monoclonal antibody, when combined with FOLFIRI (Folinic acid, Fluorouracil and Irinotecan), significantly improved Progression Free Survival, when compared to FOLFIRI alone (HR=0.73; P=0.004), with a trend towards improved Overall Survival (HR=0.85; P=0.12). Evolving data has suggested that testing for additional mutations in the RAS genes may help better understand the efficacy of/resistance to VECTIBIX®. In this present analysis, tumor samples of patients from the authors previous study, that were already known to be Wild Type KRAS – unmutated at KRAS exon 2 (N=597), were assessed for additional RAS mutations, specifically in KRAS exons 3 and 4 and NRAS exons 2, 3 and 4. Eighteen percent (18%) of the Wild Type KRAS exon 2 patients harbored additional RAS mutations. It was noted that patients receiving VECTIBIX® along with FOLFIRI had an improvement in both the median OS and PFS when they had wild-type (unmutated) RAS tumors compared to those, whose tumors harbored RAS mutations (median OS: 16.2 vs 11.8 months; median PFS: 6.4 vs 4.8 months). More importantly, amongst patients with mutated RAS tumors, the addition of VECTIBIX® to FOLFIRI resulted in no significant survival benefit compared to FOLFIRI alone (median OS: 11.8 vs 11.1 months; median PFS: 4.8 vs 4.0 months). The authors concluded that comprehensive RAS mutational analysis rather than KRAS testing alone, gives more relevant information for proper selection of patients with metastatic colorectal cancer, who would benefit from EGFR targeted monoclonal antibodies such as VECTIBIX®. In addition patients with RAS mutations could be spared from the associated cost and toxicites of EGFR targeted monoclonal antibodies that will not improve their outcomes. Peeters M, Oliner KS, Price TJ, et al. J Clin Oncol 32, 2014 (suppl 3; abstr LBA387)