
SUMMARY: Lynch Syndrome (Hereditary NonPolyposis Colorectal Cancer – HNPCC), is an autosomal dominant inherited disorder associated with increased risk of colorectal, endometrial, ovary, gastric, small bowel, pancreatic, brain, ureter or renal pelvis cancer. In the United States, approximately 140,000 new cases of colorectal cancer are diagnosed each year of which 3 to 5 percent are caused by Lynch Syndrome (LS). One in 35 patients with newly diagnosed colorectal cancer is related to Lynch Syndrome. Four genes, MLH1, MSH2, MSH6, and PMS2 are involved in the repair of mistakes that occur during DNA replication.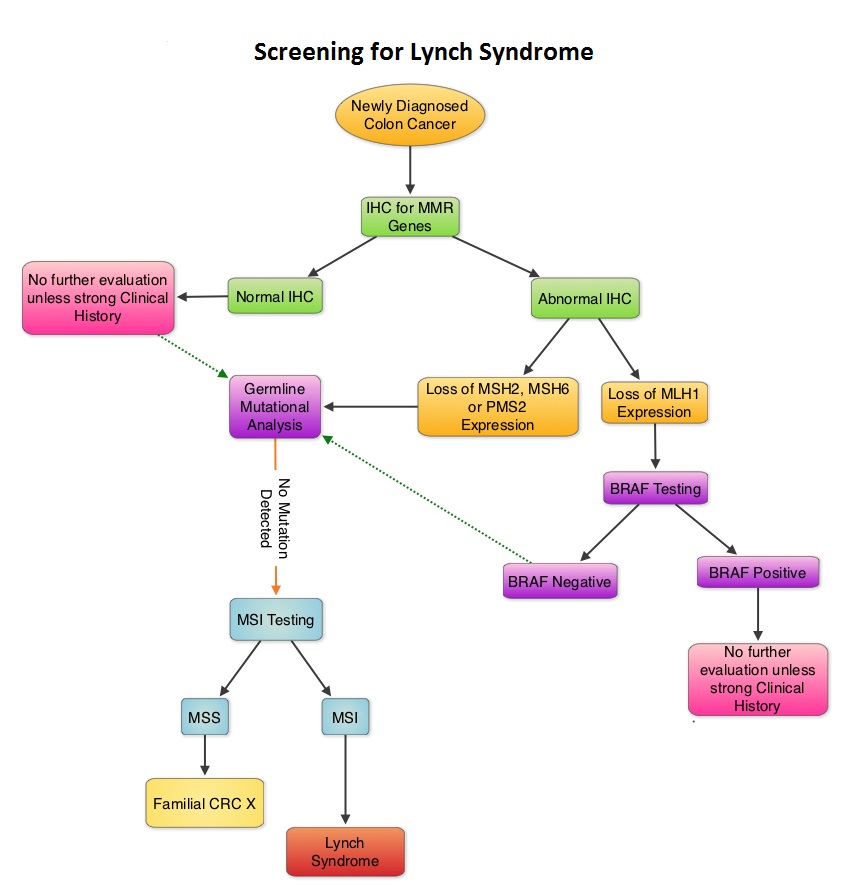 When any of these genes are mutated, repair of DNA replication mistakes is prevented resulting in continuous division of abnormal cells and possibly cancer. The EPCAM gene lies next to the MSH2 gene on chromosome 2 and mutations in the EPCAM gene can cause the MSH2 gene to be inactivated, interrupting DNA repair and leading to accumulation of DNA replication errors and possible malignancy. A Clinical Diagnosis of Lynch Syndrome can be made based on personal and family history if at least three relatives have a malignancy associated with Lynch Syndrome such as colorectal, endometrial, small bowel, ureter or renal pelvis cancer. In addition the following criteria should be met: • One relative must be a first-degree relative of the other two. • At least two successive generations must be affected. • At least one relative with a Lynch syndrome associated cancer should be diagnosed before 50 years of age. • Familial Adenomatous Polyposis should be excluded. • Tumors should be verified whenever possible. Because family history can sometimes be difficult to obtain or confirm NCCN in those circumstances has recommended screening all newly diagnosed colorectal cancer patients for Lynch syndrome. Germline defects/mutations in the mismatch repair genes MLH1, MSH2, MSH6 and PMS2 results in microsatellite instability in tumors. Tumors are described as MSI-High when they have changes in 2 or more, of the 5 microsatellite markers. So, High levels of MSI within a tumor are suggestive of defective DNA mismatch repair. ImmunoHistoChemistry (IHC) staining of tumor tissue is performed for protein expression of the four mismatch repair genes known to be mutated in Lynch Syndrome (MLH1, MSH2, MSH6 and PMS2). IHC test is described as normal when all 4 mismatch repair proteins are normally expressed suggesting that an underlying mismatch repair gene mutation is unlikely. When IHC test is abnormal, it means that that at least one of the 4 mismatch repair proteins is not expressed and an inherited mutation may be present in the gene related to that protein. This can be further confirmed by mutation analysis of the corresponding gene. Screening tests for Lynch syndrome include IHC staining of tumor tissue for protein expression of the four mismatch repair genes and tumor evaluation for MSI. In LS, more than 90% of the tumors are MSI-H (microsatellite instability-high) and/or lack expression of at least one of the mismatch repair proteins by IHC staining and there is a 96% correlation between IHC and MSI when used as a screening test for LS. Approximately 5% of tumors that display MSI may have normal protein expression for the four mismatch repair genes. It should be noted that an abnormal MSI and/or IHC test in colon cancer patients is not diagnostic of Lynch syndrome but can be a useful screening test. This is because even though MSI in the tumor tissue is pathognomonic of Lynch syndrome, approximately 15% of patients with sporadic colorectal cancers exhibit tumors with high MSI as a result of somatic MLH1 promoter hypermethylation. Further, the majority of colon cancer tumors that lack protein expression on IHC staining of MLH1 (often coexisting with loss of PMS2) are often due to an acquired genetic defect. If the IHC indicates absence of MLH1 protein expression, tumor should be tested for BRAF mutation V600E which can be seen in sporadic colorectal cancers but rarely found in patients who have Lynch Syndrome. Once a diagnosis of Lynch Syndrome is made, at risk family members should undergo colonoscopic evaluation at 20-25 years of age or 2-5 years prior to the earliest colon cancer, if it is diagnosed before age 25 and is repeated every 1-2 years. Prophylactic hysterectomy and bilateral salpingo-oophorectomy (BSO) should be considered by women who have completed childbearing. NCCN Guidelines Version 1.2014 Lynch Syndrome
When any of these genes are mutated, repair of DNA replication mistakes is prevented resulting in continuous division of abnormal cells and possibly cancer. The EPCAM gene lies next to the MSH2 gene on chromosome 2 and mutations in the EPCAM gene can cause the MSH2 gene to be inactivated, interrupting DNA repair and leading to accumulation of DNA replication errors and possible malignancy. A Clinical Diagnosis of Lynch Syndrome can be made based on personal and family history if at least three relatives have a malignancy associated with Lynch Syndrome such as colorectal, endometrial, small bowel, ureter or renal pelvis cancer. In addition the following criteria should be met: • One relative must be a first-degree relative of the other two. • At least two successive generations must be affected. • At least one relative with a Lynch syndrome associated cancer should be diagnosed before 50 years of age. • Familial Adenomatous Polyposis should be excluded. • Tumors should be verified whenever possible. Because family history can sometimes be difficult to obtain or confirm NCCN in those circumstances has recommended screening all newly diagnosed colorectal cancer patients for Lynch syndrome. Germline defects/mutations in the mismatch repair genes MLH1, MSH2, MSH6 and PMS2 results in microsatellite instability in tumors. Tumors are described as MSI-High when they have changes in 2 or more, of the 5 microsatellite markers. So, High levels of MSI within a tumor are suggestive of defective DNA mismatch repair. ImmunoHistoChemistry (IHC) staining of tumor tissue is performed for protein expression of the four mismatch repair genes known to be mutated in Lynch Syndrome (MLH1, MSH2, MSH6 and PMS2). IHC test is described as normal when all 4 mismatch repair proteins are normally expressed suggesting that an underlying mismatch repair gene mutation is unlikely. When IHC test is abnormal, it means that that at least one of the 4 mismatch repair proteins is not expressed and an inherited mutation may be present in the gene related to that protein. This can be further confirmed by mutation analysis of the corresponding gene. Screening tests for Lynch syndrome include IHC staining of tumor tissue for protein expression of the four mismatch repair genes and tumor evaluation for MSI. In LS, more than 90% of the tumors are MSI-H (microsatellite instability-high) and/or lack expression of at least one of the mismatch repair proteins by IHC staining and there is a 96% correlation between IHC and MSI when used as a screening test for LS. Approximately 5% of tumors that display MSI may have normal protein expression for the four mismatch repair genes. It should be noted that an abnormal MSI and/or IHC test in colon cancer patients is not diagnostic of Lynch syndrome but can be a useful screening test. This is because even though MSI in the tumor tissue is pathognomonic of Lynch syndrome, approximately 15% of patients with sporadic colorectal cancers exhibit tumors with high MSI as a result of somatic MLH1 promoter hypermethylation. Further, the majority of colon cancer tumors that lack protein expression on IHC staining of MLH1 (often coexisting with loss of PMS2) are often due to an acquired genetic defect. If the IHC indicates absence of MLH1 protein expression, tumor should be tested for BRAF mutation V600E which can be seen in sporadic colorectal cancers but rarely found in patients who have Lynch Syndrome. Once a diagnosis of Lynch Syndrome is made, at risk family members should undergo colonoscopic evaluation at 20-25 years of age or 2-5 years prior to the earliest colon cancer, if it is diagnosed before age 25 and is repeated every 1-2 years. Prophylactic hysterectomy and bilateral salpingo-oophorectomy (BSO) should be considered by women who have completed childbearing. NCCN Guidelines Version 1.2014 Lynch Syndrome
Tag: Colon Cancer
Maintenance treatment with capecitabine and bevacizumab versus observation after induction treatment with chemotherapy and bevacizumab in metastatic colorectal cancer (mCRC) The phase III CAIRO3 study of the Dutch Colorectal Cancer Group (DCCG)
SUMMARY: Treatment of metastatic colorectal cancer with a combination of chemotherapy given along with AVASTIN® is well established. However the duration of therapy remains unclear and it is common to give drug holidays to patients. The outcome in patients who are given these drug holidays remains unclear. The CAIRO3 study is a phase III trial in which patients with previously untreated, unresectable metastatic colorectal cancer received induction treatment with six cycles of Capecitabine (XELODA®)/Oxaliplatin (ELOXATIN®) plus Bevacizumab (AVASTIN®) – CAPOX-B. Patients who had not progressed during induction and had reponses or had stable disease (N=558) were then randomized to receive either XELODA® at 625 mg/m2 twice daily along with AVASTIN® at 7.5 mg/kg every 3 weeks or be observed. Upon first progression, patients in both treatment groups were treated with CAPOX-B until second progression and this was considered the primary endpoint for this study. Secondary endpoints included Overall Survival (OS). Median follow up was 40 months. The median time to second progression from randomization was 19.8 months in the maintenance group and 15 months in the observation group (HR=0.63; P<0.001) The time to first progression in the maintenance treatment group was 8.5 months versus 4.1 months in the observation group (HR 0.41; P<0.001). The time to second progression following treatment with CAPOX-B was 11.8 months in the maintenance group versus 10.5 months for the observation group (HR 0.77; P=0.007), representing a 23% reduction in the risk of progression. The adjusted median OS was 21.7 months with maintenance treatment and 18.2 months in the observation group (HR=0.80; P=0.035). Treatment was well tolerated with slight increase in hand-foot syndrome and neurotoxicity in the maintenance group. Based on this data, the authors recommended maintenance treatment with XELODA® and AVASTIN® until progression or unacceptable toxicity, following 6 cycles of efficacious treatment with CAPOX-B. It is important to note that in the SAKK 41/06 trial conducted by the Swiss Group, observation alone was non-inferior to single agent maintenance AVASTIN® following initial chemotherapy, suggesting that the addition of fluoropyrimidine (XELODA®) chemotherapy to AVASTIN® as maintenance treatment, improves time to progression and median OS in patients with metastatic colorectal cancer. Koopman M, Simkens LH, Ten Tije, AJ et al. J Clin Oncol 31, 2013 (suppl; abstr 3502)
Validation of the 12-Gene Colon Cancer Recurrence Score in NSABP C-07 As a Predictor of Recurrence in Patients With Stage II and III Colon Cancer Treated With Fluorouracil and Leucovorin (FU/LV) and FU/LV Plus Oxaliplatin
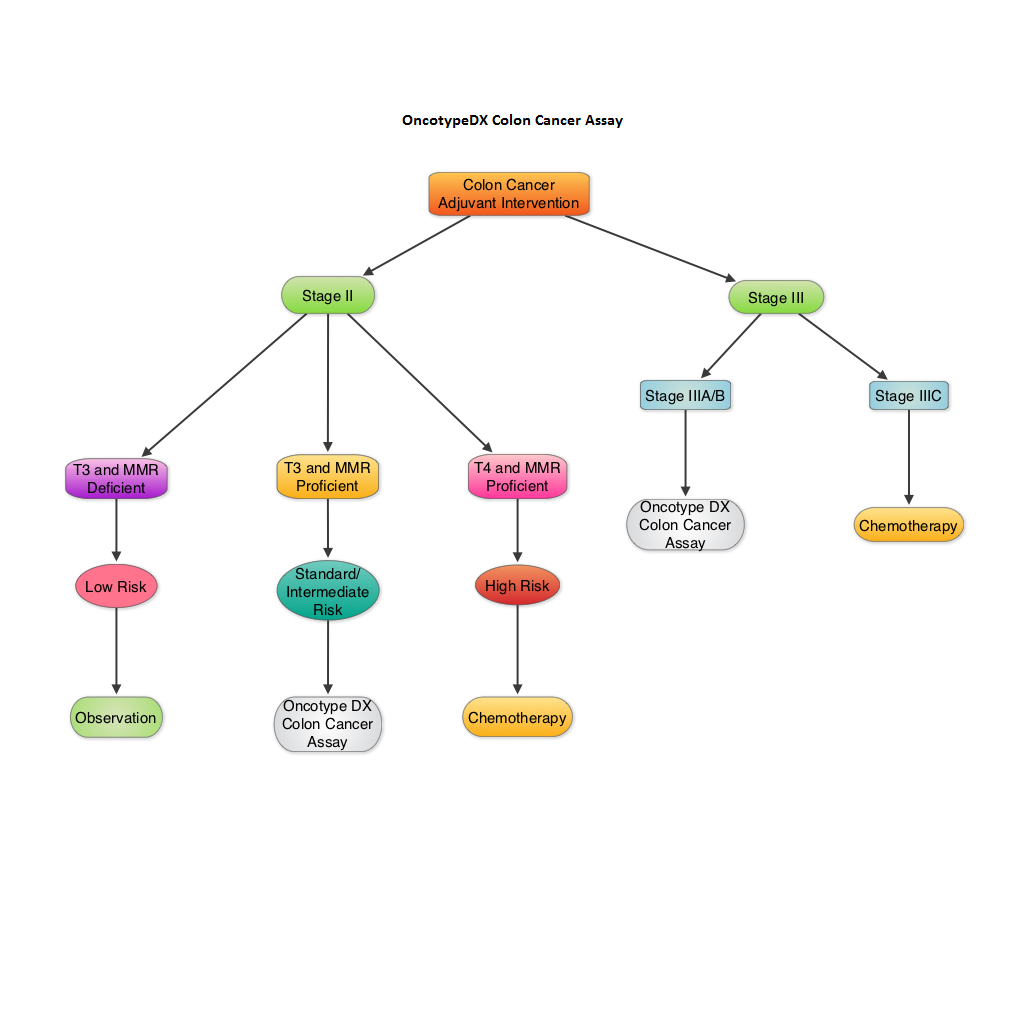
SUMMARY: The beneficial role of adjuvant chemotherapy is established in Stage III colon Cancer. This however is less convincing in patients with stage II colon cancer. The conventional clinical and pathological features such as Tumor stage, Grade, Lymphovascular invasion and number of lymph nodes evaluated, may be of some prognostic significance in Stage II colon cancer, but have not been validated. Nonetheless, a majority of these patients receive ELOXATIN® (Oxaliplatin) based adjuvant chemotherapy, with very little benefit and significant toxicity. The 12-gene Colon Cancer Recurrence Score assay was developed after it was validated in multiple studies in over 3000 patients. This assay is not recommended for Stage II MMR (MisMatchRepair) Deficient patients, as these patients have a better survival and their tumors are resistant to 5-Fluorouracil and may actually do worse with adjuvant chemotherapy following surgery. The recurrent score corresponds to the likelihood of colon cancer recurrence 3 years after surgery, with a higher score suggesting a higher risk of recurrence. The authors in this analysis conducted a prospectively designed, clinical validation study of Recurrence Score, in 892 fixed Paraffin embedded tumor specimens from patients with stage II and III colon cancer, randomly assigned to Fluorouracil (FU) or FU plus ELOXATIN® in the National Surgical Adjuvant Breast and Bowel Project C-07. The primary objective of this study was to retrospectively determine the relationship between the recurrent score and the recurrent risk in stage II/III patients treated with 5-FU or 5-FU/ELOXATIN®. Secondary objectives were to determine if recurrence score provided significant information beyond T stage, tumor grade, MMR status and number of lymph nodes examined. From this analysis, the authors reported that recurrent score performs similarly in both Stage II and Stage III colon cancer patients and predicts recurrence risk beyond T and N stage, Grade, MMR status, number of lymph nodes examined and treatment. Amongst Stage II patients, T4 tumors that are MMR proficient fall in the high risk category and chemotherapy should be considered regardless of the recurrent score whereas T3 tumors that are MMR proficient fall in the standard/intermediate risk category and recurrent score assay may assist in the decision making process. In this group, a recurrence score of 41 or more puts these patients at a recurrence risk that is similar to those who have T4 tumors that is MMR proficient and will therefore benefit from adjuvant chemotherapy. In certain stage IIIA/B patients, a low recurrence score of less than 30 is associated with low absolute benefit with ELOXATIN® and therefore is not recommended. The authors concluded that the 12- Gene Colon Cancer Recurrent Score results can help guide adjuvant therapy decisions for patients with Stage II colon cancer and certain patients with Stage III colon cancer. Yothers G, O’Connell MJ, Lee M, et al. J Clin Oncol 2013;31:4512-4519.
Bevacizumab plus capecitabine versus capecitabine alone in elderly patients with previously untreated metastatic colorectal cancer (AVEX) an open-label, randomised phase 3 trial
SUMMARY: The authors in this randomized phase III trial specifically enrolled chemo naïve patients, 70 years of age or older, with metastatic ColoRectal Cancer (CRC) because, this sub group of patients are often excluded or under- represented in clinical trials. Two hundred and eighty (N=280) chemo naïve patients with metastatic CRC, deemed not to be candidates for more aggressive regimens such as ELOXATIN® (Oxaliplatin) or CAMPTOSAR® (Irinotecan) based chemotherapy regimens, were randomly assigned in a 1:1 ratio to receive either AVASTIN® (Bevacizumab) plus XELODA® (Capecitabine) (n=140) or XELODA® alone (n=140). Treatment consisted of XELODA® 1000 mg/m2 orally twice a day on days 1—14 alone or with AVASTIN® 7•5 mg/kg, given intravenously on day 1. Treatment was given every 3 weeks until disease progression or until unacceptable toxicities were noted. The median age was 76 years and patients were stratified by performance status. The median number of cycles for AVASTIN® plus XELODA® was 9 and for XELODA® alone was 6 cycles. The primary endpoint was Progression Free Survival (PFS). The PFS was significantly longer with the combination of AVASTIN® and XELODA® versus XELODA® alone (9•1 months vs 5•1 months; Hazard Ratio= 0•53; P<0•0001). The combination treatment in general was well tolerated but with a slightly higher incidence of hand-foot syndrome and hemorrhage compared to single agent XELODA®. Overall Survival (OS) was not significantly different between the treatment groups as this study was not powered to detect OS differences. The authors concluded that, in this study, which only enrolled elderly patients with metastatic CRC, unsuitable for aggressive therapy, a combination of AVASTIN® and XELODA® is a reasonable option with proven benefit. Cunningham D, Lang I, Marcuello E, et al. Lancet Oncol 2013;14:1077-1085
Use of Molecular Biomarkers to Inform Adjuvant Therapy for Colon Cancer
SUMMARY: The role of adjuvant chemotherapy in patients with stage III ColoRectalCancer (CRC) has been well established, with improvement in Disease Free Survival (DFS) and Overall Survival (OS). The same however, cannot be stated for patients with Stage II CRC. Several Prognostic (outcome regardless of specific treatment) and Predictive (benefit from a specific therapy) molecular biomarkers have been developed to help make treatment decisions which include MSI (MicroSatellite Instability), LOH 18q (Loss of heterozygosity on the long arm of chromosome 18), P53, TS (Thymidylate Synthase), KRAS, BRAF, ERCC1 (Excision Repair Cross-Complementation group 1), Oncotype DX and Coloprint. Even though LOH 18q, P53, TS, KRAS, BRAF and ERCC1 are of prognostic value, they presently do not provide clinical utility in the management of early stage CRC. The biomarkers of interest are MSI, Oncotype DX Colon Cancer Assay and ColoPrint. MMR and MSI: MSI is the hallmark of defective/deficient DNA MisMatchRepair (MMR) system and develops following a germline mutation in one of the MMR genes. The MMR gene system consists of several proteins which are responsible for surveillance and correction of DNA errors. These genes include MLH1, MSH2, MSH6, PMS2 and EPCAM. MSI-high (MSI-H, MMR deficient) is actually a good prognostic marker in early stage CRC, with less likelihood of lymph node involvement, systemic metastases and with improved survival. These patients do not benefit from DNA inhibiting anti-metabolites such as 5-FluoroUracil (5-FU). In fact, treatment with 5-FU could be detrimental, whereas they may be more responsive to Irinotecan. This is in contrast to early stage CRC patients with tumors that are MicroSatelliteStable (MSS) or MSI-low (MSI-L) and MMR proficient, who benefit from 5-FU based adjuvant chemotherapy with significantly improved DFS. It should be noted that the prognosis for patients with early stage CRC, whose tumors harbor V600E BRAF mutation and are MSI-H, is similar to CRC patients with MSS tumors. MSI is a genetic marker of Lynch Syndrome (Hereditary Nonpolyposis Colorectal Carcinoma – HNPCC) and approximately 15% of sporadic CRC share the genetics of Lynch Syndrome and are MSI-H and MMR-deficient. By evaluating the MMR/MSI status of a CRC patient, a clinician may be able to assess a patient’s prognosis, predict response to therapy and detect Lynch’s Syndrome, which constitutes about 3-5% of CRC cases. MSI is a functional assay and can be detected by PCR whereas ImmunoHistoChemistry (IHC) can confirm the presence or absence of MMR proteins.
ONCOTYPE DX COLON CANCER ASSAY: Oncotype DX Colon Cancer assay is a multigene expression assay and evaluates genes in the patient’s tumor, using paraffin slides. It consists of 7 potential recurrence genes and 5 internal reference genes and has been clinically validated from three prospective trials, to assess risk of recurrence, in patients with Stage II and III CRC. The Oncotype DX colon cancer assay is able to prognosticate the risk of recurrence of a particular CRC tumor but unlike the Oncotype DX assay for Breast Cancer, is unable to predict clinical benefit from adjuvant chemotherapy.
COLOPRINT: This assay uses an18 gene expression profile and requires fresh tissue. This assay is also able to assess the risk of recurrence in Stage II CRC but is unable to predict the benefit from adjuvant chemotherapy.
In summary, testing for MSI should be performed in all patients with Stage II CRC. Genetic signatures derived from Oncotype Dx Colon Cancer assay and ColoPrint may have limited clinical value for patients with early stage CRC. NCCN guidelines recommend adjuvant chemotherapy for high risk Stage II CRC. High risk for recurrence is defined as tumors that are poorly differentiated (except those tumors that are MSI-H), lymphovascular invasion, perineural invasion, bowel obstruction, localized perforation, close, indeterminate or positive margins and examination of less than 12 lymph nodes. Mettu NB, Hurwitz H and Hsu DS. Oncology 2013;27:746-754
Randomized comparison of FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment of KRAS wild-type metastatic colorectal cancer German AIO study KRK-0306 (FIRE-3)
SUMMARY: It is common practice to combine anti-EGFR agent ERBITUX® (Cetuximab) or anti-VEGF agent AVASTIN® (Bevacizumab) with chemotherapy, in the initial management of patients with metastatic colorectal cancer. There is however a higher likelihood for patients with tumors expressing wild type KRAS (non-mutated KRAS), to respond to ERBITUX®. In this randomized multicenter study, a CAMPTOSAR® (Irinotecan) based backbone, FOLFIRI (folinic acid, fluorouracil and Irinotecan) given along with ERBITUX® (Group A) was compared with FOLFIRI plus AVASTIN® (Group B), in treatment naïve patients with metastatic ColoRectal Cancer (mCRC). Of the 592 patients with wild type KRAS mCRC, 297 patients were randomized to Group A and 295 patients to Group B. The median age was 64 years. The median duration of treatment was 4.7 months and 5.3 months in Group A and Group B respectively. The primary endpoint was Objective Response Rate (ORR). Even though the ORR was comparable in Groups A and B (62% vs 57%), there was a significant improvement in the overall survival (OS) favoring Group A (28.8 vs 25.0 months, HR= 0.77, P=0.0164). The comparable response rates and surprising improvement in OS in the ERBITUX® group suggests that either ERBITUX® or AVASTIN® can be added to FOLFIRI, in the first-line treatment of wild type KRAS mCRC patients. It is however clear that in wild type KRAS mCRC patients, it may be harmful to combine ERBITUX® with FOLFOX chemotherapy regimen, as was seen in the EPOCH trial and based on MRC COIN trial, NORDIC-VII trial and N0147 trial, ERBITUX® should not be combined with FOLFOX chemotherapy regimen as there is no added benefit. It is now well established that mCRC that harbors KRAS mutations in exon 2 (about 40% of the patients) do not benefit from anti-EGFR therapies. The PRIME study has given us aditional insight and it appears that other activating RAS mutations may also predict lack of response to anti-EGFR therapies. With regards to BRAF mutations, they portend a poor prognosis, regardless of treatment. Heinemann V, Weikersthal LF, Decker T, et al. J Clin Oncol 31, 2013 (suppl; abstr LBA3506)
AVASTIN® (Bevacizumab)
The FDA on January 23, 2013 approved AVASTIN® for use in combination with fluoropyrimidine-irinotecan or fluoropyrimidine-oxaliplatin based chemotherapy, for the treatment of patients with metastatic colorectal cancer (mCRC) whose disease has progressed on a first-line AVASTIN® – containing regimen. The FDA initially approved AVASTIN® in 2004 for the first-line treatment of patients with metastatic carcinoma of the colon and rectum (in combination with intravenous 5-fluorouracil-based chemotherapy). AVASTIN® is a product of Genentech U.S., Inc.
ERBITUX® (Cetuximab)
The FDA on July 9, 2012 granted approval to ERBITUX® for use in combination with FOLFIRI (CAMPTOSAR® [Irinotecan], 5-fluorouracil, leucovorin) for first-line treatment of patients with K-ras mutation-negative (wild-type), EGFR-expressing metastatic colorectal cancer (mCRC) as determined by FDA-approved tests for this use. ERBITUX® is a product of Eli Lilly and Co.
STIVARGA® (Regorafenib)
The FDA on September 27, 2012 approved STIVARGA® (Regorafenib) for the treatment of patients with metastatic colorectal cancer (mCRC) who have been previously treated with fluoropyrimidine-, ELOXATIN® (Oxaliplatin)-, and CAMPTOSAR® (Irinotecan)-based chemotherapy, an anti-VEGF therapy, and, if KRAS wild type, an anti-EGFR therapy. STIVARGA® tablets are a product of Bayer HealthCare Pharmaceuticals, Inc.
ZALTRAP® (Ziv-aflibercept injection)
The FDA on August 3, 2012 approved ZALTRAP® (Ziv-aflibercept injection), for use in combination with 5-fluorouracil, leucovorin, CAMPTOSAR® (Irinotecan) (FOLFIRI) for the treatment of patients with metastatic colorectal cancer (mCRC) that is resistant to or has progressed following an oxaliplatin containing regimen. ZALTRAP® is a product of Sanofi U.S., Inc.