
The FDA on May 24, 2019 approved JAKAFI® for steroid-refractory acute Graft-Versus-Host Disease (GVHD) in adult and pediatric patients 12 years and older. JAKAFI® is a product of Incyte Corporation.
Tag: General Medical Oncology & Hematology
AACR Late-Breaking Research Predicting Response to Anti-PD1/PDL1 Therapy beyond Tumor Mutational Burden
SUMMARY: Immunotherapy with checkpoint inhibitors such as anti-PD1/PDL1 antibodies, is rapidly moving to the forefront of cancer treatment. These agents include PD1 targeted therapies such as KEYTRUDA® (Pembrolizumab), OPDIVO® (Nivolumab) and LIBTAYO® (Cemiplimab-rwlc) and PDL1 targeted therapies such as TECENTRIQ® (Atezolizumab), IMFINZI® (Durvalumab) and BAVENCIO® (Avelumab). Treatment with checkpoint inhibitors given as a single agent or in combination with chemotherapy has resulted in significant survival benefit in a variety of solid tumors, as well as hematologic malignancies. The efficacy of checkpoint inhibitors however varies considerably across different cancer types. Understanding tumors and their microenvironment and identifying the underlying variables that predict response to anti-PD1/PDL1 antibodies, has been challenging.
Tumor Mutational Burden (TMB) has recently emerged as a potential biomarker for immunotherapy with anti PD-1/PDL1 antibodies. TMB can be measured using Next-Generation Sequencing (NGS) and is defined as the number of somatic coding base substitutions and short insertions and deletions (indels), per megabase of genome examined. Several studies have incorporated Tumor Mutational Burden (TMB) as a biomarker, using the validated cutoff of TMB of 10 or more mutations/megabase as High, and less than 10 mutations/megabase, as Low. Drawbacks with TMB include sample consumption, higher attrition rate due to sample quality and quantity, and lack of standardization for the different TMB testing assays, with the definition of High TMB varying across studies from 7.4 or more to 20 mutations/megabase.
The Cancer Genome Atlas (TCGA), a landmark cancer genomics program, is a joint effort between the National Cancer Institute and the National Human Genome Research Institute. This program began in 2006 and has molecularly characterized over 20,000 primary cancers and matched normal samples, across 33 different cancer types. After 12 years and contributions from over 11,000 patients, TCGA has deepened our understanding of the molecular basis of cancer, changed the way cancer patients are managed in the clinic, established a rich genomics data resource for the research community and helped advance health and science technologies.
The authors in this study systematically analyzed Whole Exome Sequencing (WES) and RNA sequencing (RNAseq) data of 10,000 patients from the Cancer Genome Atlas, and the Overall Response Rate (ORR) to anti-PD1/PDL1 therapy of 21 different cancer types obtained from previous clinical trials. The researchers took into consideration more than 30 different variables belonging to three distinct classes: a) those associated with tumor neoantigen landscape (Tumor Mutational Burden-TMB) b) tumor microenvironment and inflammation, and c) the checkpoint inhibitor targets (PD1/PDL1). The performance of each of these variables and their combinations was then evaluated in predicting the ORR to anti-PD1/PDL1 therapy.
It was noted that the most important predictor of response to anti-PD1/PDL1 therapy across cancer types was CD8+ T-cell abundance in the tumor microenvironment, followed by the Tumor Mutational Burden, and a high PD1 gene expression in each cancer type in a fraction of samples. These three top predictors encompassed the three distinct classes considered in this analysis, and their combination was highly predictive of the ORR to anti-PD1/PDL1 therapy, and was able to explain more than 80% of the variance observed across different tumor types.
The authors concluded that in this first systemic evaluation of the different variables associated with PD1/PDL1 therapy response across different tumor types, the three top predictors mentioned above can explain most of the observed cross-cancer response variability. Combining tumor mutational burden, CD8+ T-cell abundance and PD1 mRNA expression accurately predicts response to anti-PD1/PDL1 therapy across cancers. Lee JS and Ruppin E. Presented at: 2019 AACR Annual Meeting; March 29 to April 3, 2019; Atlanta, GA.LB-017/9
Antimicrobial Prophylaxis for Adult Patients with Cancer-Related Immunosuppression ASCO and IDSA Clinical Practice Guideline Update
SUMMARY: Patients undergoing cytotoxic chemotherapy and Hematopoietic Stem Cell Transplantation (HSCT), when neutropenic, are at risk for infection. The risk of infection increases with the depth and duration of neutropenia. The greatest infection risk is among those who experience profound, prolonged neutropenia after chemotherapy. Neutropenia is defined as an absolute neutrophil count of less than 1,000/µL, severe neutropenia as absolute neutrophil count less than 500/µL and profound neutropenia as less than 100/µL. Neutropenia is considered protracted if it lasts for 7 days or more. Fever in neutropenic patients is defined as a single oral temperature of 38.3°C (101°F) or more or a sustained temperature of 38.0°C (100.4°F) or more over a period of 1 hour.
The ASCO in partnership with Infectious Diseases Society of America (IDSA) convened an Expert Panel and updated the 2013 ASCO guideline on antimicrobial prophylaxis for immunosuppressed adult patients undergoing treatment of malignancy. The expert panel conducted a systematic review of relevant studies which included six new or updated meta-analyses and six new primary studies, from May 2011 to November 2016. The guideline recommendations were based on the review of evidence by the Expert Panel.
KEY RECOMMENDATIONS
CLINICAL QUESTION 1 – Antibacterial Prophylaxis: Does antibacterial prophylaxis with a Fluoroquinolone, compared with placebo, no intervention, or another class of antibiotic, reduce the incidence of and mortality as a result of febrile episodes in patients with cancer?
Recommendation: Antibiotic prophylaxis with a Fluoroquinolone is recommended for patients who are at high risk for Febrile Neutropenia or profound, protracted neutropenia, such as those patients with Acute Myeloid Leukemia/Myelodysplastic syndromes (AML/MDS) or Hematopoietic Stem Cell Transplantation (HSCT) treated with myeloablative conditioning regimens. Antibiotic prophylaxis is not routinely recommended for patients with solid tumors, for patients who are at low risk of profound, protracted neutropenia and when CSF prophylaxis effectively reduces the severity and duration of neutropenia.
CLINICAL QUESTION 2 – Antifungal Prophylaxis: Does antifungal prophylaxis with an oral triazole or parenteral Echinocandin, compared with no prophylaxis, or another treatment option, reduce the incidence of and mortality, as a result of febrile episodes in patients with cancer?
Recommendation 2.1: Antifungal prophylaxis with an oral triazole or parenteral echinocandin is recommended for patients who are at risk for profound, protracted neutropenia and mucositis, such as most patients with AML/MDS or HSCT. Antifungal prophylaxis is not routinely recommended for patients with solid tumors. Clinicians should be able to differentiate the risks for invasive candidiasis from the risks for invasive mold infection. This is because Fluconazole is active against yeast but not mold whereas Echinocandins and other azole antifungals, such as Posaconozole, Voriconozole, or Isavuconazole are mold-active agents. A mold-active triazole is recommended where the risk of invasive Aspergillosis is more than 6%, such as in patients with AML/MDS during the neutropenic period associated with chemotherapy, in the late stage postallogeneic SCT and/or in the context of GVHD. Antifungal prophylaxis is not routinely recommended for patients who are at low risk of profound, protracted neutropenia and when CSF prophylaxis effectively reduces the severity and duration of neutropenia.
Recommendation 2.2: Prophylaxis is recommended with Trimethoprim-Sulfamethoxazole (TMP-SMX), for patients receiving chemotherapy regimens associated with more than 3.5% risk for pneumonia from Pneumocystis jirovecii (eg, for those on 20 mg or more of prednisone daily for more than 4 weeks). For those hypersensitive to Sulfonamides or unable to tolerate TMP-SMX, alternative options include Dapsone, aerosolized Pentamidine, or Atovaquone.
CLINICAL QUESTION 3 – Antiviral Prophylaxis: Does antiviral prophylaxis reduce the incidence of immunosuppression-related viral infections in patients with cancer compared with no prophylaxis or another treatment option?
Recommendation 3.1: Herpes Simplex Virus-seropositive patients undergoing allogeneic HSCT or leukemia induction therapy should receive prophylaxis with a nucleoside analog such as Acyclovir.
Recommendation 3.2: For patients who are at high risk of Hepatitis B Virus reactivation, treatment with a nucleoside reverse transcription inhibitor (eg, Entecavir or Tenofovir) is recommended.
Recommendation 3.3: Yearly influenza vaccination with inactivated quadrivalent vaccine is recommended for all patients receiving chemotherapy for malignancy and all family and household contacts and health care providers. It is best administered more than 1 week after the last treatment or more than 2 weeks before chemotherapy administration. Individuals older than 65 years should receive the high-dose vaccine.
Recommendation 3.4: The Expert Panel also supports other vaccination recommendations for immunosuppressed adult oncology patients that are contained within the IDSA guideline for vaccination of the immunosuppressed patients.
CLINICAL QUESTION 4 – Do additional precautions, such as hand hygiene, air filtration, or a neutropenic diet, reduce the risk of infection in neutropenic patients with cancer compared with no or other additional precautions?
Recommendation 4.1: All health care workers should comply with hand hygiene and respiratory hygiene/cough etiquette guidelines to reduce the risk for aerosol- and direct or indirect contact-based transmission of pathogenic microorganisms in the health care setting.
Recommendation 4.2: Outpatients with neutropenia from cancer therapy should avoid prolonged contact with environments that have high concentrations of airborne fungal spores (eg, construction and demolition sites, intensive exposure to soil through gardening or digging, or household renovation).
Antimicrobial Prophylaxis for Adult Patients With Cancer-Related Immunosuppression: ASCO and IDSA Clinical Practice Guideline Update. Taplitz RA, Kennedy EB, Bow EJ, et al. J Clin Oncol 2018;36:3043-3054
ELZONRIS® (Tagraxofusp-erzs)
The FDA on December 21, 2018 approved ELZONRIS®, a CD123-directed cytotoxin, for Blastic Plasmacytoid Dendritic Cell Neoplasm (BPDCN) in adults and in pediatric patients 2 years and older. ELZONRIS® is a product of Stemline Therapeutics.
FDA Approves VITRAKVI®, A Novel Tumor Agnostic Therapy for TRK Fusion-Positive Cancers
SUMMARY: The FDA on November 26, 2018, granted accelerated approval to VITRAKVI® (Larotrectinib) for adult and pediatric patients with solid tumors that have a NeuroTrophic Receptor tyrosine Kinase (NTRK) gene fusion without a known acquired resistance mutation, that are either metastatic or where surgical resection is likely to result in severe morbidity, and who have no satisfactory alternative treatments or whose cancer has progressed following treatment. This is the second tissue-agnostic FDA approval for the treatment of cancer. Tumor genomic profiling enables the identification of specific genomic alterations and thereby can provide personalized treatment options with targeted therapies that are specific for those molecular targets. The FDA in May 2017 granted accelerated approval to KEYTRUDA® (Pembrolizumab), for adult and pediatric patients with unresectable or metastatic, MicroSatellite Instability-High (MSI-H) or MisMatch Repair deficient (dMMR) solid tumors. This was the first FDA approval of a systemic cancer treatment, based on a specific genetic biomarker, independent of tumor origin (first tissue/site-agnostic approval).
A genomic test can be performed on a tumor specimen or on cell-free DNA in plasma (“liquid biopsy”). ImmunoHistoChemistry (IHC) test can be performed on tumor tissue for protein expression that demonstrates a genomic variant known to be a drug target, or to predict sensitivity to a chemotherapeutic drug. Next-generation sequencing (NGS) platforms or second-generation sequencing unlike the first-generation sequencing, known as Sanger sequencing, perform massively parallel sequencing, which allows sequencing of millions of fragments of DNA from a single sample. With this high-throughput sequencing, the entire genome can be sequenced in less than 24 hours. Recently reported genomic profiling studies performed in patients with advanced cancer suggest that actionable mutations are found in 20-40% of patients’ tumors. Next-generation sequencing has enabled the detection of Neurotrophic Tropomyosin Receptor Kinase (NTRK) gene fusions, which was first discovered in colon cancer in 1982. The three TRK family of Tropomyosin Receptor Kinase (TRK) transmembrane proteins TRKA, TRKB, and TRKC are encoded by Neurotrophic Tropomyosin Receptor Kinase genes NTRK1, NTRK2, and NTRK3, respectively. These receptor tyrosine kinases are expressed in human neuronal tissue and are involved in a variety of signaling events such as cell differentiation, cell survival and apoptosis of peripheral and central neurons. They therefore play an essential role in the physiology of development and function of the nervous system. There are over 50 different partner genes that fuse with NTRK genes. Chromosomal fusion involving NTRK genes arise early in cancer development and remain so as tumors grow and metastasize. Gene fusions involving NTRK genes lead to transcription of chimeric TRK proteins which can confer oncogenic potential by increasing cell proliferation and survival. Early clinical evidence suggests that these gene fusions lead to oncogene addiction regardless of tissue of origin. (Oncogene addiction is the dependency of some cancers on one or a few genes for the maintenance of the malignant phenotype). It is estimated that gene fusions involving NTRK genes occurs in about 0.5% to 1% of many common malignancies but in more than 90% of certain rare tumor types, such as salivary gland tumors, a form of juvenile breast cancer, and infantile fibrosarcoma.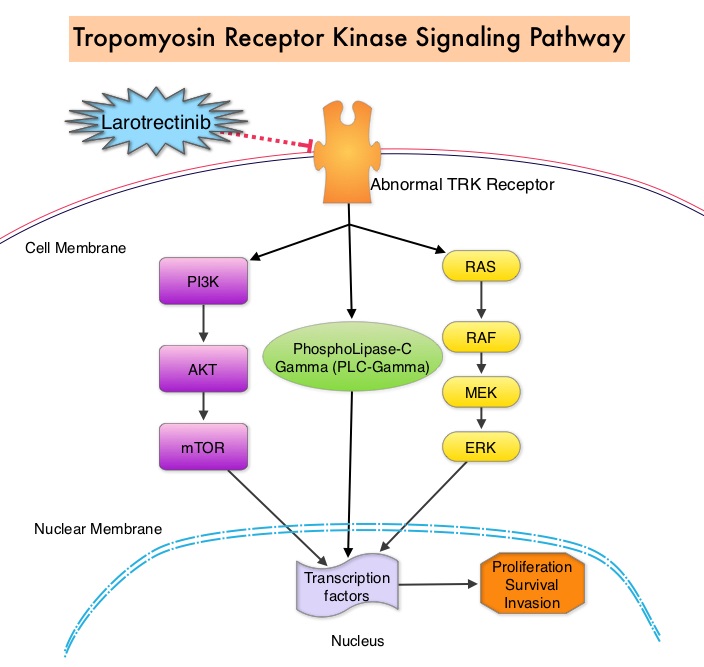
The approval of VITRAKVI®, a potent and highly selective, oral, small molecule inhibitor of all three TRK proteins was based on data from three multicenter, open-label, single-arm clinical trials – LOXO-TRK-14001, a phase I study involving adults, SCOUT, a phase I-II study involving children and NAVIGATE, a phase II study involving adolescents and adults. The authors in this development program included patients of any age and with any tumor type who had chromosomal fusion involving NTRK genes (Age and Tumor agnostic therapy). Positive NTRK gene fusion status was prospectively determined in local laboratories using NGS or Fluorescence In Situ Hybridization (FISH). Treatment efficacy was evaluated in the first 55 patients with unresectable or metastatic solid tumors harboring an NTRK gene fusion enrolled across the three trials. All patients were required to have progressed following systemic therapy for their disease if available, or would have required surgery with significant morbidity for locally advanced disease. Twelve patients were less than 18 years of age. A total of 12 cancer types were represented, with the most common being salivary gland tumors (22%), soft tissue sarcoma (20%), infantile fibrosarcoma (13%), and thyroid cancer (9%). NTRK gene fusions were inferred in three pediatric patients with infantile fibrosarcoma who had a documented ETV6 translocation by FISH. The Primary end point for the combined analysis was the Overall Response Rate (ORR) according to Independent review. Secondary end points included Duration of Response, Progression Free Survival, and safety.
The ORR was 75%, including 22% Complete Responses and 53% Partial Responses. At the time of database lock, median Duration of Response had not been reached. Response duration was 6 months or longer for 73%, 9 months or longer for 63%, and 12 months or longer for 39% of patients. The safety of VITRAKVI® was evaluated in 176 patients enrolled across the three clinical trials, including 44 pediatric patients. The most common adverse reactions (20% or more) with VITRAKVI® were fatigue, nausea, vomiting and abnormal liver function studies. None of the patients on VITRAKVI® discontinued therapy, due to a drug-related adverse event.
It was concluded that TRK fusions defined a unique molecular subgroup of advanced solid tumors in children and adults and VITRAKVI® had marked and durable antitumor activity in patients with TRK fusion-positive cancer, regardless of age of the patient or tumor type. Efficacy of Larotrectinib in TRK Fusion–Positive Cancers in Adults and Children. Drilon A, Laetsch TW, Kummar S, et al. N Engl J Med 2018; 378:731-739
VITRAKVI® (Larotrectinib)
The FDA on November 26, 2018 granted accelerated approval to VITRAKVI® for adult and pediatric patients with solid tumors that have a Neurotrophic Receptor Tyrosine Kinase (NTRK) gene fusion without a known acquired resistance mutation, that are either metastatic or where surgical resection is likely to result in severe morbidity, and who have no satisfactory alternative treatments or whose cancer has progressed following treatment. VITRAKVI® is a product of Loxo Oncology Inc. and Bayer.
GAMIFANT® (Emapalumab)
The FDA on November 20, 2018 approved GAMIFANT®, a monoclonal antibody that binds and neutralizes Interferon Gamma, for adult and pediatric (newborn and older) patients with primary Hemophagocytic Lymphohistiocytosis (HLH) with refractory, recurrent or progressive disease or intolerance with conventional HLH therapy. GAMIFANT® is a product of Novimmune SA.
MULPLETA® (Lusutrombopag)
The FDA on July 31, 2018 approved MULPLETA® for thrombocytopenia in adults with Chronic Liver Disease (CLD) who are scheduled to undergo a medical or dental procedure. MULPLETA® is a product of Shionogi Inc.
Chronic Diseases Associated with Increased Cancer Risk
SUMMARY: Cancer along with Cardiovascular disease, Diabetes, Chronic Kidney Disease and Respiratory disease, account for over 80% of all chronic disease deaths. Gouty arthritis is the most common inflammatory arthritis worldwide. Chronic inflammation may be the common denominator for chronic diseases and cancer, although other mechanisms may come into play. Patients with chronic diseases have associated lifestyle risk factors as well, which can reduce life span and increased cancer risk.
The purpose of this Prospective cohort study was to assess the independent as well as joint associations of several common chronic diseases and disease markers with cancer risk, and to explore the benefit of physical activity in reducing the cancer risk associated with chronic diseases and disease markers.
This study cohort consisted of 405,878 participants and the authors selected five common chronic diseases for evaluation, which account for most of the disease burden worldwide. They included Cardiovascular disease and associated markers such as diastolic blood pressure and systolic blood pressure, total cholesterol level, and heart rate, Diabetes and fasting blood glucose level using WHO criteria, Chronic Kidney Disease markers such as dipstick proteinuria and estimated Glomerular Filtration Rate using National Kidney Foundation criteria, Pulmonary disease markers such as Forced Expiratory Volume in one second and Forced Vital Capacity using Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria and Gouty arthritis marker such as uric acid. In this study, 48% were men and 52% were women. These participants were followed for an average of 8.7 years and the main outcome measures were cancer incidence and cancer mortality overall, as well as cancer specific incidence and mortality. The eight chronic diseases or markers included Blood Pressure, Total Cholesterol, Heart Rate, Diabetes, Proteinuria, Glomerular Filtration Rate, Pulmonary disease and Gouty arthritis marker Uric acid.
The authors observed a statistically significantly increased risk of incident cancer for the eight diseases and markers individually with the exception of Blood Pressure and Pulmonary disease. All eight diseases and markers were statistically significantly associated with risk of cancer death. Population Attributable Fraction (PAF) is the proportional reduction in population disease or mortality that would occur if exposure to a risk factor were reduced to an alternative ideal exposure scenario (eg. no tobacco use). The PAFs of cancer incidence or cancer mortality from the eight chronic diseases and markers together were comparable to those from five major lifestyle factors – ever smoking, insufficient physical activity, insufficient fruit and vegetable intake, ever alcohol consumption, and non-ideal BMI, combined (cancer incidence: 20.5% versus 24.8%; cancer mortality: 38.9% versus 39.7%). Among physically active (versus inactive) participants, the increased cancer risk associated with chronic diseases and markers was decreased by 48% for cancer incidence and 27% for cancer mortality.
It was concluded that chronic diseases contribute to more than 20% of the risk for incident cancer and more than one third of the risk for cancer death and is as important as five major lifestyle factors combined. Physical activity is associated with significant reduction in the cancer risk associated with chronic diseases. Cancer risk associated with chronic diseases and disease markers: prospective cohort study. Tu H, Wen CP, Tsai SP, et al. BMJ 2018;360:k134
Late Breaking Abstract – ASCO 2018 Broad Range of MSI-H tumors Linked with Lynch Syndrome
SUMMARY: The FDA in 2017 granted accelerated approval to KEYTRUDA® (Pembrolizumab), a PD-1 blocking antibody, for adult and pediatric patients with unresectable or metastatic, MicroSatellite Instability-High (MSI-H) or MisMatch Repair Deficient (dMMR) solid tumors that have progressed following prior treatment, and who have no satisfactory alternative treatment options. This has led to routine MSI-H/dMMR testing in advanced solid tumors. The DNA MisMatchRepair (MMR) system is responsible for molecular surveillance and works as an editing tool that identifies errors within the microsatellite regions of DNA and removes them. Defective MMR system leads to MSI (Micro Satellite Instability) and hypermutation, triggering an enhanced antitumor immune response. MSI is therefore a hallmark of defective/deficient DNA MisMatchRepair (dMMR) system and occurs in 15% of all colorectal cancers.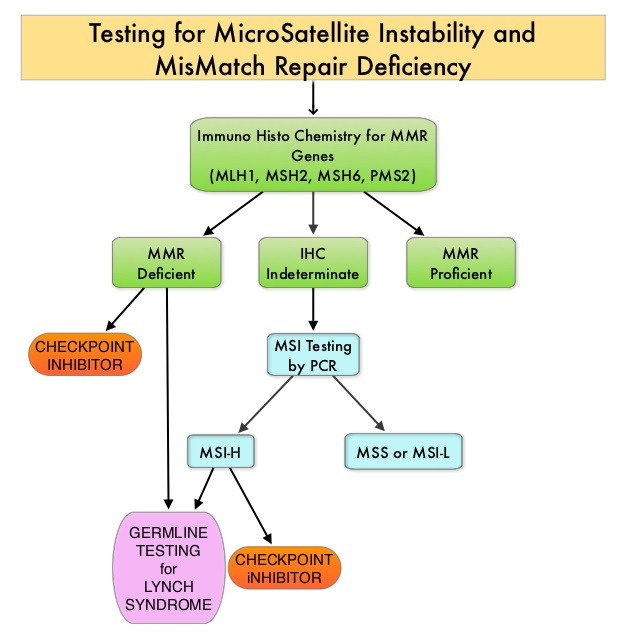
Defective MisMatchRepair can be a sporadic or heritable event. Defective MisMatchRepair can manifest as a germline mutation occurring in MisMatchRepair genes including MLH1, MSH2, MSH6, PMS2 and EPCAM. This produces Lynch Syndrome often called Hereditary Nonpolyposis Colorectal Carcinoma – HNPCC, an Autosomal Dominant disorder, that is often associated with a high risk for Colorectal and Endometrial carcinoma, as well as several other malignancies including Ovary, Stomach, Small bowel, Hepatobiliary tract, Brain and Skin. MSI is a hallmark of Lynch Syndrome-associated cancers. MSI tumors tend to have better outcomes and this has been attributed to the abundance of tumor infiltrating lymphocytes in these tumors from increase immunogenicity. These tumors therefore are susceptible to blockade with immune checkpoint inhibitors. MSI testing is performed using a PCR based assay and MSI-High refers to instability at 2 or more of the 5 mononucleotide repeat markers and MSI-Low refers to instability at 1 of the 5 markers. Patients are considered Micro Satellite Stable (MSS) if no instability occurs. MSI-L and MSS are grouped together because MSI-L tumors are uncommon and behave similar to MSS tumors. Tumors considered MSI-H have deficiency of one or more of the DNA MisMatchRepair genes. MMR gene deficiency can be detected by ImmunoHistoChemistry (IHC). NCCN Guidelines recommend MMR or MSI testing for all patients with a history of Colon or Rectal cancer. Unlike Colorectal and Endometrial cancer, where MSI-H/dMMR testing is routinely undertaken, the characterization of Lynch Syndrome across heterogeneous MSI-H/dMMR tumors is unknown.
The aim of the study was to determine the prevalence of germline mutations in the DNA mismatch repair genes diagnostic of Lynch Syndrome, across MSI-H tumors. The researchers in this study analyzed 15,045 tumor samples collected from patients with more than 50 different types of cancer using a comprehensive genomic test called MSK-IMPACT (Integrated Mutation Profiling of Actionable Cancer Targets), a next-generation sequencing platform. The MSK-IMPACT assay is a qualitative in-vitro diagnostic test that uses targeted next-generation sequencing of Formalin Fixed Paraffin-Embedded (FFPE) tumor tissue matched with normal specimens, from patients with solid tumors, to detect tumor gene alterations in a broad multigene panel. It is the first multiplex tumor profiling test to receive FDA authorization. The MSK-IMPACT test can look for gene mutations and other errors in all solid tumors, regardless of their origin.
Scores of less than 3, 3-9 and 10 or more were designated MSS, MSI-Indeterminate (MSI-I) or MSI-H status, respectively. Germline mutations were assessed in MLH1, MSH2, MSH6, PMS2, EPCAM. ImmunoHistoChemical staining (IHC) for dMMR, and tumor signatures in Lynch Syndrome patients were assessed.
Of the tumor samples analyzed, 93.2% were MSS, 4.6% were MSI-I, and 2.2% were MSI-H. Germline mutations indicative of Lynch Syndrome were identified in 0.3% of microsatellite-stable tumors, 1.9% of MSI-I tumors, and 16.3% of MSI-H tumors (P<0.001). The authors noted that nearly 50% of patients with MSI-H/MSI-I tumors identified as having Lynch Syndrome, had cancers other than colorectal or endometrial carcinoma – the two malignancies that are typically seen with Lynch Syndrome. The cancer types identified that were previously not linked to or rarely, linked to the Lynch Syndrome, included Mesothelioma, Sarcoma, Adrenocortical cancer, Melanoma, Prostate and Ovarian germ cell cancer. Nearly 40% of these patients did not meet the genetic testing criteria for Lynch Syndrome. MMR-deficiency was found in 98.3% of MSI-I/MSI-H tumor samples.
It was concluded that MSI-H/dMMR tumors, regardless of cancer type and irrespective of the family history, should prompt germline testing for the evaluation of Lynch Syndrome. This will increase the ability to recognize Lynch Syndrome, not only in the patients tested, but also in at-risk family members, thus enabling the implementation of enhanced surveillance and risk reduction measures. Pan-cancer microsatellite instability to predict for presence of Lynch syndrome. Schwark AL, Srinivasan P, Kemel Y, et al. J Clin Oncol 36, 2018 (suppl; abstr LBA1509)