
The FDA on November 8, 2019 approved REBLOZYL® for treatment of anemia in adult patients with beta Thalassemia who require regular red blood cell transfusions. REBLOZYL® is a product of Celgene Corp.
Tag: General Medical Oncology & Hematology
GIVLAARI® (Givosiran)
The FDA on November 20, 2019 approved GIVLAARI® for adults with Acute Hepatic Porphyria (AHP). GIVLAARI® is a product of Alnylam Pharmaceuticals, Inc.
Antibiotic Treatment Prior to Immune Checkpoint Inhibitor Therapy has a Detrimental Effect on Response Rates and Overall Survival
SUMMARY: The American Cancer Society estimates that in 2019, there will be an estimated 1,762,450 new cancer cases diagnosed and 606,880 cancer deaths in the United States. Immunotherapy with Immune Checkpoint Inhibitors (ICIs) has revolutionized cancer care and has become one of the most effective treatment options by improving Overall Response Rate and prolongation of survival across multiple tumor types. These agents target Programmed cell death protein-1 (PD-1), Programmed cell death ligand-1 (PD-L1), Cytotoxic T-Lymphocyte-Associated protein-4 (CTLA-4), and many other important regulators of the immune system.
Preclinical studies have suggested that immune-based therapies for cancer may have a very complex interplay with the host’s microbiome and there may be a relationship between gut bacteria and immune response to cancer. The crosstalk between microbiota in the gut and the immune system allows for the tolerance of commensal bacteria (normal microflora) and oral food antigens and at the same time enables the immune system to recognize and attack opportunistic bacteria. Immune Checkpoint Inhibitors strongly rely on the influence of the host’s microbiome, and the gut microbial diversity enhances mucosal immunity, dendritic cell function, and antigen presentation. Broad-spectrum antibiotics can alter the bacterial composition and bacterial diversity of our gut, by killing the good bacteria. It has been postulated that this may negate the benefits of immunotherapy and influence treatment outcomes.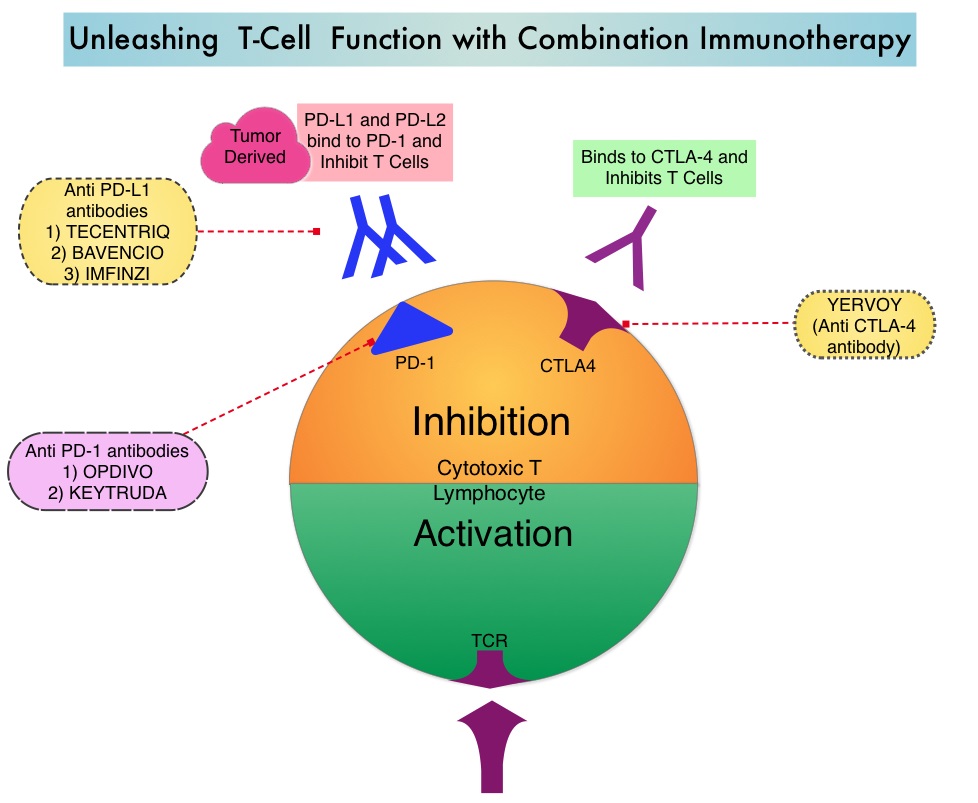
The authors conducted this study to determine whether there was an association between antibiotic therapy administered prior to or concurrently with ICI therapy and Overall Survival (OS) and Response Rates, in patients with cancer, treated with ICIs in routine clinical practice. In this prospective, multicenter cohort study, 196 patients with cancer who received ICI therapy were recruited at two tertiary care centers between January 2015 and April 2018. Majority of enrolled patients had Non-Small Cell Lung Cancer (N=119), but patients with Melanoma (N=38) as well as Urologic and Head and Neck cancers (N=39) were also included in the analysis. The median age was 68 years, and majority of patients had metastatic disease at the time of treatment initiation with ICIs and 96% of patients received anti-PD-1/PD-L1 therapy alone. Broad spectrum antibiotics up to 30 days prior to commencement of ICI qualified as prior antibiotic exposure whereas concurrent treatment with antibiotics was defined as antibiotic treatment from the first day of ICI treatment until cessation. Beta-lactams were the most commonly prescribed antibiotic class, and were given as a single course for less than 7 days. When antibiotics were administered concurrently with ICIs, patients tended to be treated longer and with multiple courses. The common indication for both prior and concurrent antibiotic treatment was respiratory infections, and 15% of patients received antibiotic therapy prior to ICI therapy, whereas 35% of patients received antibiotics concurrently with ICIs. The Primary endpoint was Overall Survival (OS), calculated from the time of ICI therapy commencement and radiologic response to treatment, with disease refractory to ICI therapy defined as progressive disease 6-8 weeks after the first ICI dose, without evidence of pseudoprogression.
In this analysis, antibiotic treatment prior to ICI therapy had a significant adverse effect on Overall Survival, with a median survival of only 2 months for those who received prior antibiotic treatment versus 26 months for antibiotic-naive patients (HR=7.4; P<0.001). Further, patients who had received prior antibiotic treatment had a higher likelihood of primary refractoriness to ICIs, compared to those who did not receive antibiotics (81% versus 44% (P<0.001). The poor OS outcomes when patients received antibiotic treatment prior to ICI therapy were noted, irrespective of tumor site (OS in NSCLC 26 vs 2.5 months, P<0.001, OS in Melanoma 14 vs 3.9 months, P<0.001, OS in other tumors 11 vs 1.1 months, P <0.001). Multivariate analyses confirmed that prior antibiotic therapy and response to ICI therapy were associated with OS, independent of tumor site, disease burden, and performance status. Antibiotic treatment administered concurrently with ICIs however, was not associated with worse Overall Survival.
It was concluded that treatment with antibiotics prior to therapy with Immune Checkpoint Inhibitors in routine clinical practice, is associated with a worse treatment response and Overall Survival in unselected group of patients. This study suggests that timing of antibiotic exposure may be crucial and the authors recommend that studies are urgently required to investigate antibiotic-mediated alterations of gut microbiota as a determinant of poorer outcomes, following treatment with Immune Checkpoint Inhibitors. Association of Prior Antibiotic Treatment With Survival and Response to Immune Checkpoint Inhibitor Therapy in Patients With Cancer. Pinato DJ, Howlett S, Ottaviani D, et al. JAMA Oncol. 2019, Sep 12. doi: 10.1001/jamaoncol.2019.2785. [Epub ahead of print]
Liquid Biopsy DNA Methylation Assay Highly Specific for Cancer Detection and Prognosis
SUMMARY: Screening both healthy and high-risk populations with a peripheral blood sample (liquid biopsy) has the potential to detect cancer at an early stage, with an increased opportunity to offer curative therapies. Screening assays for cancer should be highly specific with a low rate of false-positive results and overdiagnosis. Analysis of cell-free DNA (cfDNA) with a Liquid Biopsy is presently approved to select EGFR targeted therapies (cobas EGFR mutation test), in patients with advanced Non Small Cell Lung Cancer. However, the role of cell-free DNA analysis for early detection of cancer is not well established.
The Cancer Genome Atlas (TCGA), a landmark cancer genomics program, is a joint effort between the National Cancer Institute and the National Human Genome Research Institute. This program began in 2006 and has molecularly characterized over 20,000 primary cancers and matched normal samples, across 33 different cancer types. After 12 years and contributions from over 11,000 patients, TCGA has deepened our understanding of the molecular basis of cancer, changed the way cancer patients are managed in the clinic, established a rich genomics data resource for the research community and helped advance health and science technologies.
The Circulating Cell-Free Genome Atlas (CCGA) is a prospective, multi-center, observational study and is the largest study ever initiated, to develop a noninvasive, liquid biopsy assay for early cancer detection, based on cell-free DNA (cfDNA). This study completed enrollment of approximately 15,000 participants with and without cancer (56% with 20 tumor types and all clinical stages), across 142 sites in the US and Canada. The principal goal is to develop a noninvasive cancer detection assay and the CCGA was designed to characterize the landscape of genomic cancer signals in the blood and to detect and validate GRAIL’s multi-cancer early detection blood test through three pre-planned sub-studies. The authors in 2018 previously reported that it is possible to detect early-stage lung cancer, with a high degree of specificity, from a simple blood test, using targeted sequencing and whole-genome sequencing. In this substudy, liquid biopsy could accurately detect over 40% of early-stage lung cancers (Stage I-IIIA), with 98% specificity. It was determined that whole-genome bisulfite sequencing for DNA methylation was the most effective approach for early cancer detection. 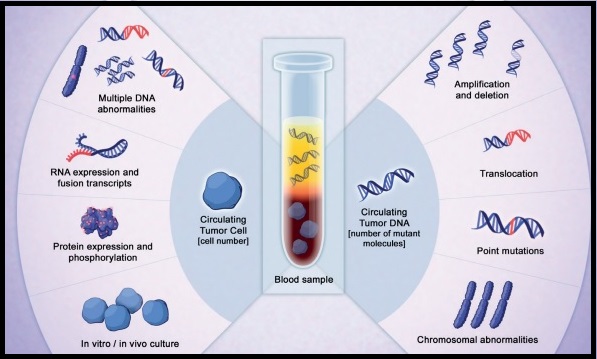
DNA methylation is a natural epigenetic mechanism used by cells to regulate gene expression with some regions of hypermethylation and some regions of hypomethylation, and is a chemical modification to DNA. In cancer, abnormal methylation patterns and the resulting changes in gene expression can contribute to tumor growth (hypermethylation can cause tumor-suppressor genes to be inactivated). Methylation patterns, are unique to the tumor DNA, enabling tumor detection and localization but are not of value when it comes to precision therapies. This is unlike mutations and copy number changes, which can be detected in white blood cells in individuals without cancer as well, leading to false-positives.
In two separate presentations, the authors in this present sub-study reported the results for patients with more than 20 cancer subtypes across all stages and evaluated the prognostic significance of detecting abnormal patterns of cfDNA methylation by whole-genome bisulfite sequencing (WGBS) assay. The goal of targeted methylation assay was to detect both early and advanced disease cancers, and improve clinical outcomes
Liu, MC, et al. reported outcomes for 2,301 participants (1422 had cancer and 879 did not) with more than 20 cancer types (12 prespecified and high-risk cancers included Lung, HR negative Breast, Colorectal, Anorectal, Esophageal, Gastric, Liver, Pancreatic, Head and Neck, Ovary, Myeloma and Lymphoid neoplasms) across all stages. The 12 prespecified cancers account for two thirds of all cancer deaths in the US. At 99% specificity, the sensitivity for these 12 high-risk cancers ranged from 59-86% at early stages (stages I–III). For all 20 cancer types, the overall detection rate across all stages was 55%. Additionally, a Tissue of Origin result was provided for 94% of all cancers detected and of these, the assay correctly identified the Tissue of Origin in 90% of cases, which the authors commented is critical for guiding efficient downstream workup for a positive signal.
Oxnard GR, et al. performed an exploratory longitudinal analysis and reported the results of the Overall Survival of 1,320 participants with more than 20 cancer types in this substudy, thereby evaluating the prognostic significance of detection by this assay. Across all stages of disease, cancers detected by cfDNA whole-genome bisulfite sequencing for DNA methylation were associated with significantly worse survival than those not detected by the blood test. The 2-year Overall Survival was less than 50% among patients whose cancers were detected by the assay compared with 2-year OS of over 90% for those whose cancers were not detected by this assay. The poor prognostic ability of this assay was seen in both cancers that presented with symptoms and those found via screening suggesting that DNA–based detection with this methylation assay may be an indicator of prognosis. In multivariate analysis, cancers detected by this assay had double the risk of death (HR=2.6; P< 0.001) when accounting for clinical stage, cancer type, histologic grade, age, sex, and method of diagnosis and also had comparable prognostic significance to clinical stage (P <0.001).
It was concluded from these two presentations that cfDNA test based on the presence of DNA methylation is highly specific at detecting high-risk malignancies, with very high accuracy for identifying the tissue of origin, and may also have prognostic value.
Genome-wide Cell-free DNA (cfDNA) Methylation Signatures and Effect on Tissue of Origin (TOO) Performance. Liu MC, Jamshidi A, Venn O, et al. 2019 ASCO Annual Meeting. Abstract 3049. Presented June 1, 2019.
Prognostic significance of blood-based cancer detection in plasma cell-free DNA (cfDNA): Evaluating risk of overdiagnosis. Oxnard GR, Chen X, Fung ET, et al. 2019 ASCO Annual Meeting. Abstract 1545. Presented June 3, 2019.
ROZLYTREK® (Entrectinib)
The FDA on August 15, 2019 granted accelerated approval to ROZLYTREK® for adults and pediatric patients 12 years of age and older with solid tumors that have a Neurotrophic Tyrosine Receptor Kinase (NTRK) gene fusion without a known acquired resistance mutation, are metastatic or where surgical resection is likely to result in severe morbidity, and have progressed following treatment or have no satisfactory standard therapy. ROZLYTREK® is a product of Genentech Inc.
TURALIO® (Pexidartinib)
The FDA on August 2, 2019 approved TURALIO® capsules for adult patients with symptomatic Tenosynovial Giant Cell Tumor (TGCT) associated with severe morbidity or functional limitations and not amenable to improvement with surgery. TURALIO® is the first systemic therapy approved for patients with TGCT. TURALIO® is a product of Daiichi Sankyo, Inc.
Anticonvulsant Prophylaxis and Steroid Use in Adults with Metastatic Brain Tumors ASCO and SNO Endorsement of the Congress of Neurological Surgeons Guidelines
SUMMARY: Brain metastases are the most common intracranial tumors in adults in the United States. In patients with systemic malignancies, brain metastases occur in 10-30% of adults, with Lung, Breast, and Melanoma continuing to be the leading cause of brain metastases. The incidence of brain metastases may be on the rise due to both improved imaging techniques, as well as better control of extracerebral disease from advances in systemic therapy.
The Congress of Neurological Surgeons (CNS) developed a series of guidelines for the treatment of adult patients with metastatic brain tumors, including systemic therapy and supportive care topics. The ASCO/SNO (Society of NeuroOncology) Expert Panel determined that the recommendations from the CNS anticonvulsants and steroids guidelines, published January 9, 2019, are clear, thorough, and based on the most relevant scientific evidence. ASCO/SNO endorsed these two CNS guidelines with minor alterations. This guideline was developed by a multidisciplinary Expert Panel that included a patient representative and an ASCO guidelines staff member with health research methodology expertise.
Guideline Questions
CNS Anticonvulsant Guideline
1) Do prophylactic antiepileptic drugs decrease the risk of seizures in nonsurgical patients with brain metastases who are otherwise seizure free?
2) Do prophylactic antiepileptic drugs decrease the risk of seizures in patients with brain metastases and no prior history of seizures in the postoperative setting?
CNS Steroids Guideline
1) Do steroids improve neurologic symptoms and/or quality of life in patients with metastatic brain tumors compared with supportive care only or other treatment options?
2) If steroids are administered, what dose should be given?
Target Population
Adults with metastatic brain tumors.
Target Audience
Medical oncologists, Neurologists, and others who provide care for adults with metastatic brain tumors.
Recommendations
CNS Anticonvulsants Guideline:
1) Prophylactic antiepileptic drugs are not recommended for routine use in patients with brain metastases who did not undergo surgical resection and who are otherwise seizure free.
2) Routine postcraniotomy antiepileptic drug use for seizure-free patients with brain metastases is not recommended.
CNS Steroids Guideline: Steroid Therapy Versus No Steroid Therapy
Patients with asymptomatic brain metastases without mass effect:
Insufficient evidence exists to make a treatment recommendation for this clinical scenario.
Patients with brain metastases with mild symptoms related to mass effect:
1) Corticosteroids are recommended to provide temporary symptomatic relief of symptoms related to increased intracranial pressure and edema secondary to brain metastases. It is recommended for patients who are symptomatic from metastatic disease to the brain that a starting dose of Dexamethasone 4 to 8 mg/day be considered. Patients with brain metastases with moderate to severe symptoms related to mass effect
2) Corticosteroids are recommended to provide temporary symptomatic relief of symptoms related to increased intracranial pressure and edema secondary to brain metastases. If patients exhibit severe symptoms that are consistent with increased intracranial pressure, it is recommended that higher doses, such as Dexamethasone 16 mg/day or more, be considered.
Choice of steroid:
If corticosteroids are administered, Dexamethasone is the best drug choice, given the available evidence.
Duration of corticosteroid administration:
Corticosteroids, if administered, should be tapered as rapidly as possible, but no faster than clinically tolerated, on the basis of an individualized treatment regimen and a full understanding of the long-term sequelae of corticosteroid therapy.
ASCO/SNO Expert Panel comment: The Panel’s expert opinion is that, given the important adverse effects of steroids, the minimum effective dose (often no more than 4 mg) should be used where possible and night-time doses of steroids should be avoided to minimize toxicity.
Note regarding CNS Level 3 recommendation classification: CNS defines a Level 3 recommendation as, one based on “Evidence from case series, comparative studies with historical controls, case reports, and expert opinion, as well as significantly flawed randomized controlled trials”
Anticonvulsant Prophylaxis and Steroid Use in Adults With Metastatic Brain Tumors: ASCO and SNO Endorsement of the Congress of Neurological Surgeons Guidelines. Chang SM, Messersmith H, Ahluwalia M, et al. J Clin Oncol 2019;37:1130-1135
ASCO/ASH Update on Erythropoiesis Stimulating Agents for Cancer-Associated Anemia
SUMMARY: The American Society of Clinical Oncology (ASCO) along with American Society of Hematology (ASH) updated recommendations for use of Erythropoiesis Stimulating Agents (ESAs) in patients with cancer. The primary literature review included 15 meta-analyses of Randomized Clinical Trials and two Randomized Clinical Trials. These recommendations were developed using a systematic review of the literature from January, 2010, through May, 2018, and clinical experience.
Guideline question: When and how should Erythropoiesis Stimulating Agents (ESAs) be used to manage anemia in adults with cancer?
Target population: Adults with Cancer and Anemia.
Target audience: Oncologists, Hematologists, Oncology Nurses, Oncology Pharmacists, and other health care professionals who care for patients with cancer, and patients with cancer.
RECOMMENDATIONS
Clinical question 1: To reduce the need for RBC transfusions, should ESAs be offered to patients who have chemotherapy-associated anemia?
Recommendation 1.1. Depending on clinical circumstances, ESAs may be offered to patients with chemotherapy-associated anemia whose cancer treatment is not curative in intent and whose hemoglobin has declined to less than 10 g/dL. RBC transfusion is also an option, depending on the severity of the anemia or clinical circumstances
Recommendation 1.2. ESAs should not be offered to patients with chemotherapy-associated anemia whose cancer treatment is curative in intent
Clinical question 2: To reduce the need for RBC transfusions, should ESAs be offered to anemic patients with cancer who are not receiving concurrent myelosuppressive chemotherapy?
Recommendation 2.1. ESAs should not be offered to most patients with nonchemotherapy-associated anemia
Recommendation 2.2. ESAs may be offered to patients with lower risk MyeloDysplastic Syndromes and a serum Erythropoietin level 500 IU/L or less.
Clinical question 3: What special considerations apply to adult patients with nonmyeloid hematologic malignancies who are receiving concurrent myelosuppressive chemotherapy?
Recommendation 3. In patients with Myeloma, Non-Hodgkin Lymphoma, or Chronic Lymphocytic Leukemia, clinicians should observe the hematologic response to cancer treatment before considering an ESA. Particular caution should be exercised in the use of ESAs concomitant with treatment strategies and diseases where risk of thromboembolic complications is increased (see Recommendations 4 and 6). In all cases, blood transfusion is a treatment option that should be considered
Clinical question 4: What examinations and diagnostic tests should be performed before making a decision about using an ESA to identify patients who are likely to benefit from an ESA?
Recommendation 4. Before offering an ESA, clinicians should conduct an appropriate history, physical examination, and diagnostic tests to identify alternative causes of anemia aside from chemotherapy or an underlying hematopoietic malignancy. Such causes should be appropriately addressed before considering the use of ESAs. Suggested baseline investigations include thorough drug exposure history, peripheral blood smear review, analyses where indicated, for Iron, TIBC, Ferritin, Transferrin saturation, Folate, Vitamin B12, or Hemoglobinopathy screening, assessment of Reticulocyte count, occult blood loss and renal Insufficiency and baseline Erythropoietin level and TSH. Investigations may also include Direct Antiglobulin Testing (eg, Coombs test) for patients with Chronic Lymphocytic Leukemia, Non-Hodgkin Lymphoma, or a history of autoimmune disease.
Clinical question 5: Among adult patients who receive an ESA for chemotherapy-associated anemia, do Darbepoetin, Epoetin beta and alfa originator, and currently available biosimilars of Epoetin alfa differ with respect to safety or efficacy?
Recommendation 5. The Expert Panel considers Epoetin beta and alfa, Darbepoetin, and biosimilar Epoetin alfa to be equivalent with respect to effectiveness and safety
Clinical question 6: Do ESAs increase the risk of thromboembolism?
Recommendation 6. ESAs increase the risk of thromboembolism, and clinicians should carefully weigh the risks of thromboembolism and use caution and clinical judgment when considering use of these agents
Clinical question 7: Among adult patients who will receive an ESA for chemotherapy-associated anemia, what are recommendations for ESA dosing and dose modifications?
Recommendation 7. It is recommended that starting and modifying doses of ESAs follow FDA guidelines
Clinical question 8: Among adult patients who will receive an ESA for chemotherapy-associated anemia, what is the recommended target HgB level?
Recommendation 8. HgB may be increased to the lowest concentration needed to avoid or reduce the need for RBC transfusions, which may vary by patient and condition
Clinical question 9: Among adult patients with chemotherapy-associated anemia who do not respond to ESA therapy (less than 1 to 2 g/dL increase in HgB or no decrease in transfusion requirements), does continuation of ESA therapy beyond 6-8 weeks provide a benefit?
Recommendation 9. ESAs should be discontinued in patients who do not respond within 6-8 weeks. Patients who do not respond to ESA treatment should be reevaluated for underlying tumor progression, Iron deficiency, or other etiologies for anemia
Clinical question 10: Among adult patients with chemotherapy-associated anemia, does Iron supplementation concurrent with an ESA reduce transfusion requirements?
Recommendation 10. Iron replacement may be used to improve HgB response and reduce RBC transfusions for patients receiving ESA with or without iron deficiency. Baseline and periodic monitoring of Iron, total Iron-Binding Capacity, Transferrin saturation, or Frritin levels is recommended
Management of cancer-associated anemia with erythropoiesis-stimulating agents: ASCO/ASH clinical practice guideline update. Bohlius J, Bohlke K, Castelli R, et al. Blood Advances 2019;3:1197-1210
Vitiligo Associated with Reduced Risk of Internal Malignancies
SUMMARY: Vitiligo is a common acquired skin disorder affecting 1% of the population worldwide. Vitiligo is generally considered to be an autoimmune disorder and is characterized by destruction of melanocytes resulting in patchy loss of skin pigmentation. CD8 positive T cells have been implicated in the progression of Vitiligo. Approximately 15-25% of individuals with Vitiligo are also affected by at least one other autoimmune disorder, such as autoimmune Thyroid disease, Rheumatoid arthritis, type 1 Diabetes, Psoriasis, Pernicious anemia, Addison disease, or Systemic Lupus Erythematosus.
There is epidemiologic evidence demonstrating reduced risks of both Melanoma and non-Melanoma skin cancers (NMSCs) in patients with Vitiligo, suggesting that Vitiligo-associated autoimmunity exerts immune surveillance on skin cells other than melanocytes. Further, it has been shown that the occurrence of de novo Vitiligo following treatment with Immune Checkpoint Inhibitors may be a surrogate marker for improved survival in patients with advanced Melanoma. This suggests that increased T-cell activity following blockade of immune checkpoints, targets cancer cells as well as melanocytes in the skin.
The benefit of increased T-cell activity on cancers of internal organs in patients with Vitiligo, however has been unclear. In this publication, the authors evaluated whether autoreactive T-cell responses to melanocytes in patients with Vitiligo would affect tumor immunosurveillance in different internal organs.
We conducted a nationwide population-based cohort study to explore the risk of internal malignancies in patients with Vitiligo using the 10-year Korean National Health Insurance (NHI) claims database from 2007-2016. This study included 101,078 patients with Vitiligo and 202,156 controls without Vitiligo. Patients were 20 years or older with Vitiligo and had at least two contacts with a physician. The authors examined the overall risk for the development of internal malignancies and organ-specific cancer risks in each group.
It was noted that after the analysis was adjusted for age, sex, and comorbidities, the overall risk of internal malignancies was significantly lower in patients with Vitiligo than in controls (HR=0.86; P<0.001). This risk reduction was more so in men than in women and younger patients 20-30 yrs old with Vitiligo, had notably reduced risk than patients 40 yrs or older. With regards to organ-specific malignancies, patients with Vitiligo had a remarkably decreased risk of cancer in the Colon and Rectum (HR=0.62; P<0.001), Ovary (HR=0.62; P<0.001), and Lung (HR=0.75; P<0.001).
It was concluded that Vitiligo was associated with a reduced risk of internal malignancies overall. The authors from the findings of this study postulated that autoimmune diseases, including Vitiligo, may provide immune surveillance for the development of cancer beyond the targeted organ. Markedly Reduced Risk of Internal Malignancies in Patients With Vitiligo: A Nationwide Population-Based Cohort Study. Bae JM, Chung KY, Yun SJ, et al. J Clin Oncol 2019;37:903-911
FDA Approves JAKAFI® for Acute GVHD
SUMMARY: The FDA on May 24, 2019 approved JAKAFI® (Ruxolitinib) for steroid-refractory acute Graft-Versus-Host Disease (GVHD) in adult and pediatric patients 12 years and older. Acute GVHD is a frequent and severe inflammatory complication of allogeneic Hematopoietic Cell Transplantation (HCT), and is a reaction of donor immune cells against host tissues. It is estimated that in the US over 8000 patients undergo allogeneic HCT each year and about 35-50% of recipients will develop acute GVHD, which remains a significant cause of morbidity and mortality in allogeneic HCT recipients. Following the preparative regimen, a series of inflammatory reactions lead to damage to the host epithelial cells by activated donor T cells. GVHD can be acute or chronic, with acute GVHD typically occurring within the first 100 days following an allogeneic transplant. Approximately 40% of patients with acute GVHD have severe disease, with a one year survival of 50% or less. Acute GVHD typically involves the skin, often starting in the palms and soles (rash/dermatitis), liver (hepatitis/jaundice), and gastrointestinal tract (abdominal pain/diarrhea). Acute GVHD is a clinical diagnosis, although histologic confirmation may be extremely helpful, if the symptoms and presentation are atypical. Risk factors for the development of acute GVHD include degree of HLA disparity, gender disparity, increased age of both the recipient and the donor, multiparous female donors, ineffective GVHD prophylaxis, intensity of the transplant conditioning regimen and the source of graft (peripheral blood or bone marrow greater than umbilical cord blood).
Risk factors for the development of acute GVHD include degree of HLA disparity, gender disparity, increased age of both the recipient and the donor, multiparous female donors, ineffective GVHD prophylaxis, intensity of the transplant conditioning regimen and the source of graft (peripheral blood or bone marrow greater than umbilical cord blood).
Patients with acute GVHD are often treated by optimizing their immunosuppression and adding methylprednisolone, with approximately 50% of patients responding to this intervention. If symptoms do not improve after a week or if progression is noted after 3 days of treatment, patients receive salvage immunosuppressive intervention, since no standard treatment with meaningful benefit has been identified.
JAKAFI® (Ruxolitinib) is a potent JAK1 and JAK2 inhibitor and exerts its mechanism of action by targeting and inhibiting the dysregulated JAK2-STAT signaling pathway. JAKAFI® in animal models was shown to reduce IL-1β, IL-6, or IFN-γ and TNF and other cytokines implicated in lymphocyte activation characteristic of GVHD. In previously published studies, JAKAFI® when used in patients with refractory GVHD demonstrated an Overall Response Rate of 85% in acute or chronic GVHD, with a 25% Complete Remission rate.
In previously published studies, JAKAFI® when used in patients with refractory GVHD demonstrated an Overall Response Rate of 85% in acute or chronic GVHD, with a 25% Complete Remission rate.
The present FDA approval was based on data from REACH1 study, which is an open-label, single-arm, multicenter, phase II trial of JAKAFI® in combination with corticosteroids, in patients with steroid-refractory grade II-IV acute GVHD. Of the 71 patients enrolled in this study, 49 patients were refractory to steroids alone, 12 patients had received two or more prior therapies for GVHD and 10 patients did not otherwise meet the FDA definition of steroid-refractory state. JAKAFI® was administered at 5 mg orally twice daily, and the dose could be increased to 10 mg twice daily after three days, in the absence of toxicity.
The Primary endpoint of this trial was the Day 28 Overall Response Rate (ORR), defined as a Complete Response (CR), Very Good Partial Response (VGPR) or Partial Response (PR), based on the Center for International Blood and Marrow Transplant Research (CIBMTR) criteria. The Day 28 ORR in the 49 patient’s refractory to steroids alone was 57% with a CR rate of 31%. The most frequently reported adverse reactions were infections (55%) and edema (51%), and the most common laboratory abnormalities were anemia, thrombocytopenia and neutropenia.
It was concluded that for patients with acute GVHD who do not adequately respond to steroids, therapies are limited and JAKAFI® is a new treatment option that fulfills this unmet need. Results from REACH1, a Single-Arm Phase 2 Study of Ruxolitinib in Combination with Corticosteroids for the Treatment of Steroid-Refractory Acute Graft-Vs-Host Disease. Jagasia M, Perales M-A, Schroeder MA, et al. Blood 2018 132:601; doi: https://doi.org/10.1182/blood-2018-99-116342