
SUMMARY: It is estimated that approximately 20% of cancer patients in the US take Omega-3 fatty acids in the form of fish oil. Fish oil is a mixture of fatty acids produced from several species of fish and the two most abundant and important fatty acids in fish oil include EicosaPentaenoic Acid (EPA) and DocosaHexaenoic Acid (DHA). Fish oil content in presently available preparations is not standardized and does not require FDA approval. Preclinical studies have demonstrated that mouse tumors recruit mesenchymal stem cells that are specifically activated by platinum based chemotherapy and secrete 2 fatty acids, 12S-HHT and 16:4(n-3)). These fatty acids are called Platinum Induced Fatty Acids (PIFAs) and they have been shown to induce resistance to a broad range of chemotherapeutic agents, by activating a cytoprotective response in the tumor tissue.  Fish oil has relevant levels of fatty acid 16:4(n-3) and preclinical models have shown that the fish oil neutralized the antitumor activity of chemotherapy, thus conferring drug resistance. With this preclinical information and given that cancer patients frequently use fish oil supplements, the authors evaluated the effect of fish oil intake in healthy volunteers, on the plasma levels of fatty acid 16:4(n-3), which has been shown to induce resistance to chemotherapeutic agents. The researchers first conducted a survey to determine what percentage of cancer patients undergoing treatment at a University Medical Center in the Netherlands were taking fish oil supplements. They also analyzed fatty acid 16:4(n-3) content, in 3 brands of fish oil supplements and 4 often consumed species of fish. The authors then randomly selected 30 healthy volunteers for the fish oil study and 20 healthy volunteers for the fish consumption study and the plasma levels of fatty acid 16:4(n-3) was measured after they consumed fish oil or fish, for a period of 2 weeks. They noted that 11% of the cancer patients in their study reported using omega-3 supplements. All fish oils tested contained amounts of fatty acid 16:4(n-3) ranging from 0.2 to 5.7 μM and this was adequate to induce chemoresistance to a variety of chemotherapeutic agents. They noted that there was a significant rise in the plasma 16:4(n-3) fatty acid levels in the healthy volunteers after they consumed fish oil supplements and fish, with high levels of fatty acid 16:4(n-3). Herring and Mackerel fish contained high levels of fatty acid 16:4(n-3), in contrast to Salmon and Tuna. The authors concluded that based on this preclinical data it is best to avoid fish oils and fish such as Herring and Mackerel in the 48 hours surrounding chemotherapy, as the high plasma 16:4(n-3) fatty acid levels may negate the effects of chemotherapy. These recommendations have been adopted by the Dutch Cancer Society and by the Dutch National Working Group for Oncologic Dieticians. Increased Plasma Levels of Chemoresistance-Inducing Fatty Acid 16:4(n-3) After Consumption of Fish and Fish Oil. Daenen LGM, Cirkel GA, Houthuijzen JM, et al. JAMA Oncol. 2015;1:350-358
Fish oil has relevant levels of fatty acid 16:4(n-3) and preclinical models have shown that the fish oil neutralized the antitumor activity of chemotherapy, thus conferring drug resistance. With this preclinical information and given that cancer patients frequently use fish oil supplements, the authors evaluated the effect of fish oil intake in healthy volunteers, on the plasma levels of fatty acid 16:4(n-3), which has been shown to induce resistance to chemotherapeutic agents. The researchers first conducted a survey to determine what percentage of cancer patients undergoing treatment at a University Medical Center in the Netherlands were taking fish oil supplements. They also analyzed fatty acid 16:4(n-3) content, in 3 brands of fish oil supplements and 4 often consumed species of fish. The authors then randomly selected 30 healthy volunteers for the fish oil study and 20 healthy volunteers for the fish consumption study and the plasma levels of fatty acid 16:4(n-3) was measured after they consumed fish oil or fish, for a period of 2 weeks. They noted that 11% of the cancer patients in their study reported using omega-3 supplements. All fish oils tested contained amounts of fatty acid 16:4(n-3) ranging from 0.2 to 5.7 μM and this was adequate to induce chemoresistance to a variety of chemotherapeutic agents. They noted that there was a significant rise in the plasma 16:4(n-3) fatty acid levels in the healthy volunteers after they consumed fish oil supplements and fish, with high levels of fatty acid 16:4(n-3). Herring and Mackerel fish contained high levels of fatty acid 16:4(n-3), in contrast to Salmon and Tuna. The authors concluded that based on this preclinical data it is best to avoid fish oils and fish such as Herring and Mackerel in the 48 hours surrounding chemotherapy, as the high plasma 16:4(n-3) fatty acid levels may negate the effects of chemotherapy. These recommendations have been adopted by the Dutch Cancer Society and by the Dutch National Working Group for Oncologic Dieticians. Increased Plasma Levels of Chemoresistance-Inducing Fatty Acid 16:4(n-3) After Consumption of Fish and Fish Oil. Daenen LGM, Cirkel GA, Houthuijzen JM, et al. JAMA Oncol. 2015;1:350-358
Tag: General Medical Oncology & Hematology
Late Breaking Abstract – ASCO 2015 Adjuvant Whole Brain Radiation Therapy Not Recommended After Stereotactic RadioSurgery
SUMMARY: Brain metastases from an extracranial primary, occur in approximately 15% of cancer patients and this is estimated to be about 400,000 to 600,000 patients annually. The incidence of brain metastases has been on the rise with the availability of more effective systemic therapies and better control of systemic disease. The most frequent malignancies associated with brain metastases include Lung cancer, Breast cancer and Melanoma. Majority of the patients with brain metastases have synchronous extracerebral metastases. A significant number of patients present with solitary or fewer than 3 brain metastases and they may be amenable to focal therapeutic interventions. However, Whole Brain Radiation Therapy (WBRT) has been the standard treatment strategy since the 1950’s. It is also well recognized that WBRT can be associated with neurocognitive dysfunction. Stereotactic RadioSurgery (SRS) is a non-surgical procedure that allows delivery of significantly higher doses of precisely focused radiation to the tumor, compared to conventional radiation therapy, with less collateral damage to the surrounding normal tissue. The technologies used for SRS include GAMMA KNIFE® which uses highly focused gamma rays, Proton Beam therapy which uses ionized hydrogen or Protons, Linear Accelerator and CYBER KNIFE® which use Photons, to target the tumor tissue.
NCCTG N0574 is a federally funded, randomized phase III clinical trial, designed to determine whether cognitive deterioration occurred less frequently with SRS alone compared to SRS followed by WBRT, in patients with 1-3 brain metastases. In this study, 213 patients with 1-3 brain metastases, each measuring less than 3 cm by contrast MRI, were enrolled and randomized to SRS alone or SRS plus WBRT. All patients underwent cognitive testing before and after treatment. Sixty eight percent (68%) of the enrolled patients had a Lung primary and the median age was 60 years. Baseline characteristics were similar in both treatment groups. The median follow up was 7.2 months. The authors used several tools to assess cognitive dysfunction and the primary endpoint was the cognitive decline at 3 months following treatment. It was noted that at 3 months, with the addition of WBRT to SRS, 91.7% of patients experienced cognitive decline compared with 63.5% for those receiving SRS alone (P=0.0007) and there was statistically significant decline in immediate recall, delayed recall and verbal fluency, in the SRS plus WBRT group. Patients who received SRS plus WBRT also reported significantly worse Quality of Life. There was however better intracranial tumor control at 6 and 12 months with SRS plus WBRT compared to SRS alone (P< 0.001), but this local control had no significant impact on the median Overall Survival (OS), with similar OS outcomes noted in both treatment groups (P=0.93). The authors concluded that the addition of WBRT to SRS can result in significant decline in neurocognitive function, without any Overall Survival benefit, compared to SRS alone. It is therefore recommended that patients with newly diagnosed brain metastases amenable to SRS, be closely monitored after SRS, with consideration given to WBRT, at the time of symptomatic progression. NCCTG N0574 (Alliance): A phase III randomized trial of whole brain radiation therapy (WBRT) in addition to radiosurgery (SRS) in patients with 1 to 3 brain metastases. Brown PD, Asher AL, Ballman KV, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA4)
Higher Risk of Fractures in Hematopoietic Stem Cell Transplant Recipients
SUMMARY: According to the CIBMTR (Center for International Blood and Marrow Transplant Research), in 2012, over 11,000 Hematopoietic Stem Cell Transplants (HSCT) in the US were Autologous and over 7500 were Allogeneic. Multiple myeloma and Lymphoma accounted for 57% of all HSCTs and AML and Myelodysplasia accounted for 51% of Allogeneic HSCTs. There has been an increase in the number of Autologous and Allogeneic transplants for treatment of malignant diseases in elderly patients, with 39% of Autologous transplant recipients and 17% of Allogeneic transplant recipients between 2006-2012 reported to be older than 60 years of age. With increase in the number of long term survivors following transplantation, early and late complications of HSCT have been the focus of increasing attention.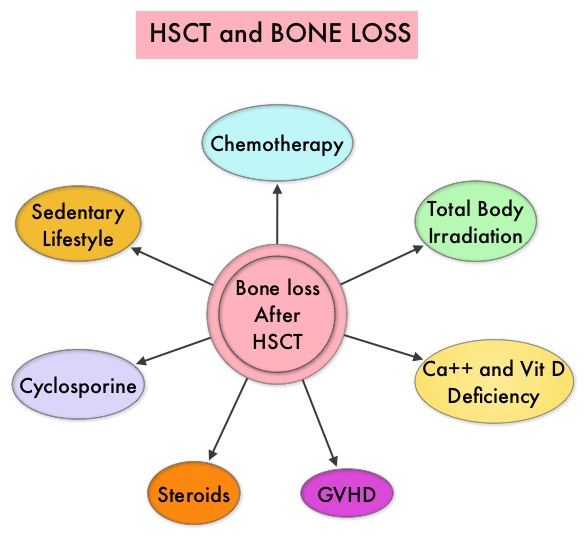 Morbidity and mortality as well as quality of life related to bone loss among long term survivors after HSCT, has been previously published. Factors contributing to bone loss in this patient population include intensive chemotherapy, total body irradiation, post-transplantation glucocorticoid use, reduced intake and metabolism of Calcium and Vitamin D, graft versus host disease, use of Cyclosporine-A and sedentary lifestyle after transplantation. Loss of Bone Mineral Density (BMD) occurs within 6 to 12 months after transplantation at all skeletal sites, followed by initial recovery of BMD in the lumbar spine and a slower recovery of BMD in the femur neck. This bone loss may persist for 48 to 120 months or even longer. The authors in this single institution, retrospective study, calculated the cumulative incidence rates of fractures among survivors of Autologous and Allogeneic Hematopoietic Stem Cell Transplantations (HSCT) and compared the rate of fractures to that of the general US population. Data was collected from 7,620 patients over 18 years of age who underwent HSCT at The University of Texas MD Anderson Cancer Center, from January 1997 to December 2011 and these patients were observed through December 2013. The authors then calculated the cumulative incidence of fractures, with death as a competing risk and the age and sex-specific fracture incidence rates were compared with those in the US general population, using estimated rates from the 1994 National Health Interview Survey and the 2004 National Hospital Discharge Survey. Of the 7,620 patients who underwent HSCT, 56% were male and 51% underwent Autologous and 49% underwent Allogeneic stem cell transplantation.
Morbidity and mortality as well as quality of life related to bone loss among long term survivors after HSCT, has been previously published. Factors contributing to bone loss in this patient population include intensive chemotherapy, total body irradiation, post-transplantation glucocorticoid use, reduced intake and metabolism of Calcium and Vitamin D, graft versus host disease, use of Cyclosporine-A and sedentary lifestyle after transplantation. Loss of Bone Mineral Density (BMD) occurs within 6 to 12 months after transplantation at all skeletal sites, followed by initial recovery of BMD in the lumbar spine and a slower recovery of BMD in the femur neck. This bone loss may persist for 48 to 120 months or even longer. The authors in this single institution, retrospective study, calculated the cumulative incidence rates of fractures among survivors of Autologous and Allogeneic Hematopoietic Stem Cell Transplantations (HSCT) and compared the rate of fractures to that of the general US population. Data was collected from 7,620 patients over 18 years of age who underwent HSCT at The University of Texas MD Anderson Cancer Center, from January 1997 to December 2011 and these patients were observed through December 2013. The authors then calculated the cumulative incidence of fractures, with death as a competing risk and the age and sex-specific fracture incidence rates were compared with those in the US general population, using estimated rates from the 1994 National Health Interview Survey and the 2004 National Hospital Discharge Survey. Of the 7,620 patients who underwent HSCT, 56% were male and 51% underwent Autologous and 49% underwent Allogeneic stem cell transplantation.  The most common reasons for HSCT were hematologic malignancies other than Multiple Myeloma (67%), Multiple Myeloma (22%) and other solid tumors (11%). The median follow up was 85 months. Fractures occurred in 8% of patients (N = 602) of whom 419 patients had an Autologous stem cell transplantation and 183 patients had Allogeneic stem cell transplantation. The incidence of fracture was higher in patients older than age 50 years, 5 times higher among patients with Multiple Myeloma compared to other hematologic malignancies and patients who underwent Autologous transplantation were 45% more likely to develop a fracture than those who underwent an Allogeneic transplantation. When age- and sex-specific fracture incidence rates after HSCT were compared with National Health Interview Survey data, females were at approximately 8 times greater risk and men 45-64 years old were at approximately 7-9 times greater risk of sustaining a fracture. The authors concluded that the incidence of fractures after HSCT is significantly higher and all patients undergoing HSCT should be considered to be at risk for post-transplantation bone loss. Measures to prevent bone loss and fractures include physical exercise, Vitamin D and Calcium supplementation, avoiding tobacco products, abstaining from excess alcohol intake and fall prevention. The authors recommend that patients undergoing HSCT should have a Dual Energy X-ray Absorptiometry scan performed at baseline and at 6 months following transplantation. Increased Incidence of Fractures in Recipients of Hematopoietic Stem-Cell Transplantation. Pundole XN, Barbo AG, Lin H, et al. J Clin Oncol 2015; 33:1364-1370
The most common reasons for HSCT were hematologic malignancies other than Multiple Myeloma (67%), Multiple Myeloma (22%) and other solid tumors (11%). The median follow up was 85 months. Fractures occurred in 8% of patients (N = 602) of whom 419 patients had an Autologous stem cell transplantation and 183 patients had Allogeneic stem cell transplantation. The incidence of fracture was higher in patients older than age 50 years, 5 times higher among patients with Multiple Myeloma compared to other hematologic malignancies and patients who underwent Autologous transplantation were 45% more likely to develop a fracture than those who underwent an Allogeneic transplantation. When age- and sex-specific fracture incidence rates after HSCT were compared with National Health Interview Survey data, females were at approximately 8 times greater risk and men 45-64 years old were at approximately 7-9 times greater risk of sustaining a fracture. The authors concluded that the incidence of fractures after HSCT is significantly higher and all patients undergoing HSCT should be considered to be at risk for post-transplantation bone loss. Measures to prevent bone loss and fractures include physical exercise, Vitamin D and Calcium supplementation, avoiding tobacco products, abstaining from excess alcohol intake and fall prevention. The authors recommend that patients undergoing HSCT should have a Dual Energy X-ray Absorptiometry scan performed at baseline and at 6 months following transplantation. Increased Incidence of Fractures in Recipients of Hematopoietic Stem-Cell Transplantation. Pundole XN, Barbo AG, Lin H, et al. J Clin Oncol 2015; 33:1364-1370
E-Cigarettes – A Policy Statement from the American Association for Cancer Research and the American Society of Clinical Oncology
SUMMARY: According to the American Cancer Society, tobacco use is responsible for nearly 1 in 5 deaths in the United States and accounts for at least 30% of all cancer deaths. Smokeless tobacco products are a major source of cancer causing nitrosamines and increase the risk of developing cancer of the oropharynx, esophagus, and pancreas. Cigarette smoke contains more than 7,000 chemicals, many of which are toxic and some linked to cancer. E-cigarettes or Electronic Nicotine Delivery Systems (ENDS) were first developed in China and introduced to the U.S. market in 2007. 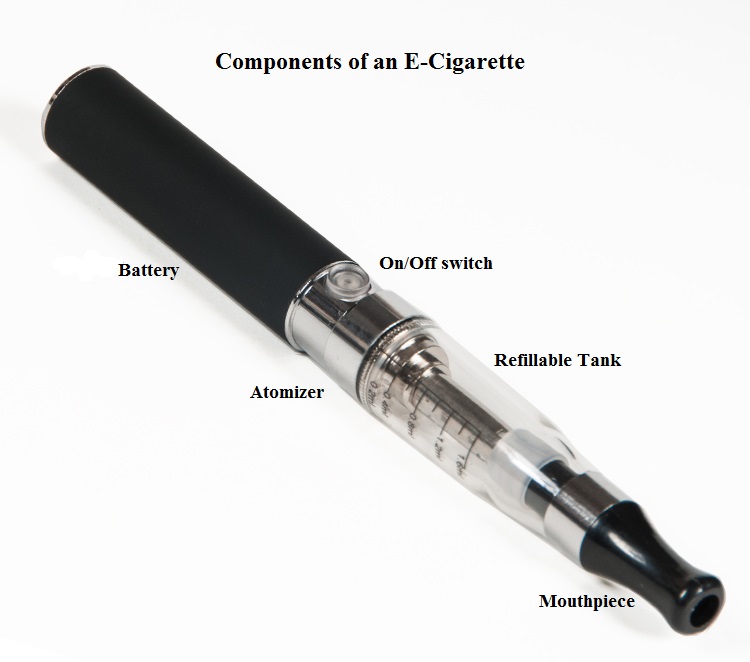 When a smoker inhales through the mouth piece of an E-cigarette, the air flow triggers a sensor that switches on a small lithium battery powered heater, which in turn vaporizes liquid nicotine along with PolyEthylene Glycol (PEG) present in a small cartridge. The PEG vapor looks like smoke. The potent liquid form of nicotine extracted from tobacco is tinctured with fragrant flavors such as chocolate, cherry and bubble gum, coloring substances, as well other chemicals and these e-liquids are powerful neurotoxins. With the rapid growth of the E-cigarette industry and the evidence of potential dangers and risk to public health, particularly children, experts from the world's leading lung organizations were compelled to release a position statement on electronic cigarettes, specifically focusing on their potential adverse effects on human health and calling on government organizations to ban or restrict the use of E-cigarettes, until their impact on health is better understood. According to the National Youth Tobacco Survey, the use of e-cigarettes has tripled from 2013 to 2014 among middle school and high school students. Epidemiological data have shown that nicotine use is a gateway to the use of cocaine and marijuana and subsequent lifelong addiction. E-cigarettes and other Electronic Nicotine Delivery Systems (ENDS), unlike combustible cigarettes and many other tobacco products are not currently regulated by the U.S. Food and Drug Administration.
When a smoker inhales through the mouth piece of an E-cigarette, the air flow triggers a sensor that switches on a small lithium battery powered heater, which in turn vaporizes liquid nicotine along with PolyEthylene Glycol (PEG) present in a small cartridge. The PEG vapor looks like smoke. The potent liquid form of nicotine extracted from tobacco is tinctured with fragrant flavors such as chocolate, cherry and bubble gum, coloring substances, as well other chemicals and these e-liquids are powerful neurotoxins. With the rapid growth of the E-cigarette industry and the evidence of potential dangers and risk to public health, particularly children, experts from the world's leading lung organizations were compelled to release a position statement on electronic cigarettes, specifically focusing on their potential adverse effects on human health and calling on government organizations to ban or restrict the use of E-cigarettes, until their impact on health is better understood. According to the National Youth Tobacco Survey, the use of e-cigarettes has tripled from 2013 to 2014 among middle school and high school students. Epidemiological data have shown that nicotine use is a gateway to the use of cocaine and marijuana and subsequent lifelong addiction. E-cigarettes and other Electronic Nicotine Delivery Systems (ENDS), unlike combustible cigarettes and many other tobacco products are not currently regulated by the U.S. Food and Drug Administration.
The American Association for Cancer Research (AACR) and American Society of Clinical Oncology (ASCO) have therefore made the following recommendations in a joint statement to guide policymakers and have encouraged oncology health care providers, to recommend FDA-approved cessation medications instead of e-cigarettes, to individuals who are interested or trying to quit smoking combustible cigarettes.
1) The FDA Center for Tobacco Products should regulate all ENDS as well as e-liquids containing tobacco-derived nicotine whether they are sold together or separately. ENDS products such as synthetic nicotine that do not meet the statutory definition of tobacco products, should then be regulated by the FDA through other appropriate authorities.
2) Manufacturers of ENDS should be required to register with the FDA and report nicotine concentration and all product and ingredient listings.
3) In the interest of public health, the FDA should exercise its regulatory authority to require safety labels and health warning regarding nicotine addiction.
4) The FDA should restrict all youth oriented marketing of ENDS, to prevent youth from initiating use of ENDS products.
5) The age and identification of customers should be checked by the Internet and mail-order sales agencies of ENDS, at the point of purchase and delivery.
6) ENDS use should be prohibited in places where combustible tobacco product use is prohibited by federal, state, or local law, until the safety of secondhand aerosol exposure is established.
7) All e-liquid containers should be required to have childproof caps.
8) ENDS and liquids containing candy and other youth friendly flavors should be prohibited, unless there is evidence demonstrating these products do not encourage youth uptake.
9) Funding generated through tobacco product taxes, including any potential taxes levied on ENDS, should be used to help support research on ENDS and other tobacco related products, and should not preclude the allocation of federal funding for this research.
10) All information related to ENDS composition, use, and health effects should be disclosed, to enhance policy decisions for ENDS product regulation.
11) In the absence of federal ENDS regulation, state and local governments should implement related regulations to protect public health, including restricting the sale, distribution, marketing, and advertising of electronic nicotine delivery systems to youth.
Electronic Nicotine Delivery Systems: A Policy Statement from the American Association for Cancer Research and the American Society of Clinical Oncology. Brandon TH, Goniewicz ML, Hanna NH, et al. Clin Cancer Res 2015; 21:1-12
Platelet Transfusions Detrimental in TTP and HIT
SUMMARY: Patients with Thrombotic Thrombocytopenic Purpura (TTP), Heparin Induced Thrombocytopenia (HIT) and Immune Thrombocytopenic Purpura (ITP) often receive prophylactic platelet transfusions even though there are no data to support this practice. These transfusions are often given preemptively to reduce the risk for spontaneous bleeding in patients who are thrombocytopenic. Thrombocytopenia refers to a platelet count below the lower limit of the normal range used by the laboratory performing the count. In the United States, a little over 2 million platelet units are transfused annually.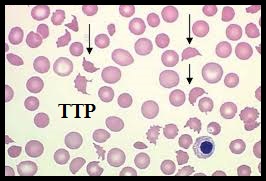 The known risks associated with platelet transfusion include febrile and allergic reactions, Transfusion Related Acute Lung Injury and infections. The authors in this study utilized a Nationwide Inpatient Sample of patients over a 5 year period from 2007-2011and evaluated the risks associated with platelet transfusions.
The known risks associated with platelet transfusion include febrile and allergic reactions, Transfusion Related Acute Lung Injury and infections. The authors in this study utilized a Nationwide Inpatient Sample of patients over a 5 year period from 2007-2011and evaluated the risks associated with platelet transfusions.  They identified 10,624 hospitalizations with TTP and platelet transfusions were reported in 10.1%, 6,332 hospitalizations with HIT and 7.1% received platelet transfusions and 79,980 admissions with ITP and 25.8% received platelet transfusions. The Odds Ratio (OR) was calculated after adjusting for age, gender, clinical severity and acuity. (An Odds Ratio is a measure of association between an exposure and an outcome. The OR represents the odds that an outcome will occur given a particular exposure, compared to the odds of the outcome occurring in the absence of that exposure). The researchers noted some alarming findings. Platelet transfusions in TTP were associated with higher odds of arterial thrombosis (OR=5.8), Acute Myocardial Infarction (OR=2.0) and mortality (OR=2.0). Platelet transfusions in HIT were associated with higher odds of arterial thrombosis (OR=3.4) and mortality (OR=5.2). Platelet transfusions in TTP or HIT however, was not associated with venous thrombosis. There were no increased risks among patients with ITP, who received platelet transfusions. The authors concluded that until future trials provide additional information, platelet transfusions should be considered a relative contraindication in patients with TTP and HIT and should only be used in situations where severe or potentially life threatening bleeding is refractory to other therapies. Platelet transfusions in platelet consumptive disorders are associated with arterial thrombosis and in-hospital mortality. Goel R, Ness PM, Takemoto CM, et al. Blood. 2015;125:1470-1476.
They identified 10,624 hospitalizations with TTP and platelet transfusions were reported in 10.1%, 6,332 hospitalizations with HIT and 7.1% received platelet transfusions and 79,980 admissions with ITP and 25.8% received platelet transfusions. The Odds Ratio (OR) was calculated after adjusting for age, gender, clinical severity and acuity. (An Odds Ratio is a measure of association between an exposure and an outcome. The OR represents the odds that an outcome will occur given a particular exposure, compared to the odds of the outcome occurring in the absence of that exposure). The researchers noted some alarming findings. Platelet transfusions in TTP were associated with higher odds of arterial thrombosis (OR=5.8), Acute Myocardial Infarction (OR=2.0) and mortality (OR=2.0). Platelet transfusions in HIT were associated with higher odds of arterial thrombosis (OR=3.4) and mortality (OR=5.2). Platelet transfusions in TTP or HIT however, was not associated with venous thrombosis. There were no increased risks among patients with ITP, who received platelet transfusions. The authors concluded that until future trials provide additional information, platelet transfusions should be considered a relative contraindication in patients with TTP and HIT and should only be used in situations where severe or potentially life threatening bleeding is refractory to other therapies. Platelet transfusions in platelet consumptive disorders are associated with arterial thrombosis and in-hospital mortality. Goel R, Ness PM, Takemoto CM, et al. Blood. 2015;125:1470-1476.
Clinical Cancer Advances 2015 Annual Report on Progress Against Cancer From the American Society of Clinical Oncology (PART II)
SUMMARY: Cancer mortality rates in the United States have declined 20% from their peak of 215 per 100,000 in 1991 to 172 per 100,000 in 2010. Part II of this Annual Report on Progress Against Cancer explores, ADVANCES IN TREATMENT, ADVANCES IN TUMOR BIOLOGY AND ADVANCES IN PATIENT CARE. Clinical study details for several of these studies can be accessed at www.oncoprescribe.com
ADVANCES IN TREATMENT
COMBINATION THERAPY
Chemotherapy and Radiotherapy significantly improves Survival for Patients with Low-Grade Glioma – Radiotherapy has been the standard first-line treatment for patients with low-grade glioma. In a study involving 251 patients with gliomas which included grade 2 Astrocytoma, Oligoastrocytoma, or Oligodendroglioma, the addition of chemotherapy (PCV regimen – (Procarbazine, Lomustine, and Vincristine) to radiation extended median survival by 5.5 years (13.3 vs 7.8 years, P=0.03; HR=0.59) and also resulted in a longer median Progression Free survival (10.4 vs 4 years, P=0.002; HR=0.50), when compared with radiotherapy alone.
First-Line Chemotherapy Added to Hormone Therapy Improves Survival for Men With Advanced Prostate Cancer – Androgen Deprivation Therapy (ADT) has been the cornerstone of treatment of advanced prostate cancer and is the first treatment intervention for hormone sensitive prostate cancer. Chemotherapy is usually considered for patients who progress on hormone therapy. In a pivotal phase III study which included 790 men with metastatic, hormone-sensitive prostate cancer, the addition of TAXOTERE® (Docetaxel) chemotherapy to ADT improved median Overall Survival by 10 months from 42.3 months in the ADT alone group to 52.7 months in the ADT plus TAXOTERE® group (HR=0.63; P<0.0006). The median time to clinical progression was 19.8 months in the ADT alone group vs 32.7 months in the ADT plus TAXOTERE® group (P < 0.0001).
TARGETED THERAPY
Overcoming Resistance to EGFR Targeted Agents in Lung Cancer– TARCEVA® (Erlotinib) and GILOTRIF® (Afatinib) are recommended as first-line treatments for patients harboring Epidermal Growth Factor Receptor (EGFR) gene mutations, which are detected in 15% of Caucasian and 40% of Asian patients with NSCLC. An additional EGFR mutation (T790M) is responsible for resistance to EGFR-targeted therapy and may be detected in about 50% of those harboring EGFR mutations in Non Small Cell Lung Cancer (NSCLC). AZD9291 and CO-1686 are two new agents which have demonstrated a 50-60% response rate in patients with T790M mutation.
New second-line treatment options for ALK-positive NSCLC – XALKORI® (Crizotinib) significantly improves PFS and Response Rates in patients with ALK-positive NSCLC. Approximately one third of these patients are resistant to XALKORI® and this has been attributed to acquired mutation within the ALK tyrosine kinase domain, amplification of the ALK fusion gene, subtherapeutic inhibition of ALK tyrosine kinase or activation of other pathways that can cause abnormal cell proliferation. ZYKADIA® (Ceritinib) resulted in an overall Response Rate (RR) of 58% and median PFS of 7 months in this patient population, with responses seen in untreated CNS lesions as well.
FDA Approves First Treatment for Chemotherapy-Resistant, Advanced Stomach Cancer – CYRAMZA® (Ramucirumab) an angiogenesis inhibitor was approved for the treatment of advanced stomach cancer or gastroesophageal junction adenocarcinoma that progressed during or after chemotherapy. The approval was based on a phase III trial involving 355 patients in which patients treated with CYRAMZA® (Ramucirumab) had longer survival (5.2 vs 3.8 months, HR = 0.78, P=0.047), when compared to placebo.
Lenvatinib: A New Option for a Difficult-to-Treat Thyroid Cancer – LENVIMA® (Lenvatinib) a Tyrosine Kinase Inhibitor, was approved for the treatment of patients with locally recurrent or metastatic, progressive, RadioActive Iodine (RAI)-refractory Differentiated Thyroid Cancer (DTC). In a phase III study involving 392 patients with advanced RAI-refractory Differentiated Thyroid Cancer (DTC), the median Progression Free Survival was 18.3 months in the LENVIMA® group and 3.6 months in the placebo group (HR= 0.21; P<0.001). The objective response rate with LENVIMA® was 64.8% versus 1.5% with placebo (P<0.001). Another targeted drug, NEXAVAR® (Sorafenib), was approved for the same patient population in 2013.
IMMUNOTHERAPY
Both antibody and cell-based immunotherapy approaches have taken center stage in cancer immunotherapy. Check point inhibitors such as anti CTLA-4. Anti PD-1 and anti PDL1 antibodies unleash the immune system allowing the T cells to attack the malignant cells.
Adjuvant Immunotherapy For Early Stage Melanoma – YERVOY® (Ipilimumab), an anti CTLA-4 antibody decreased the relative risk of recurrence by 25% (HR=0.75; P=0.0013), when compared with placebo, in patients with high risk, completely resected, stage III melanoma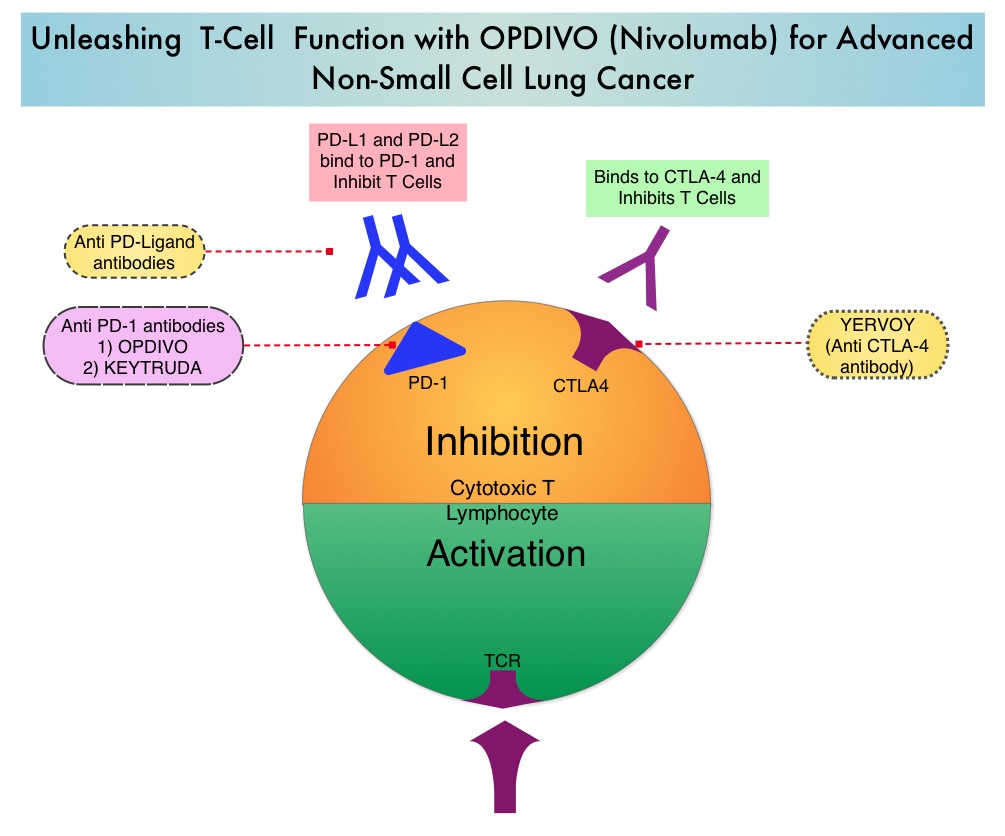
Immunotherapy in Lung Cancer – OPDIVO® (Nivolumab), a PD-1 targeted monoclonal antibody improved overall survival by 41% (HR=0.59; P=0.00025) when compared to TAXOTERE® (Docetaxel) in a randomized phase III trial in patients with metastatic squamous NSCLC, who had experienced disease progression during or after one prior platinum-based chemotherapy regimen. KEYTRUDA® (Pembrolizumab) another PD-1 antibody demonstrated superior responses in patients with lung cancer when the tumors were PD-L1 positive versus PD-L1 negative (23% vs 9%) suggesting that PD-L1 may be a predictor of response to PD-1 and PD-L1 therapies.
Tumor Directed Chimeric Antigen Receptor (CAR) T-Cell Therapy – In this type of immunotherapy, T cells are collected from the patient’s own blood and are genetically engineered to produce special receptors on their surface called chimeric antigen receptors (CAR’s). These cytotoxic T cells with these chimeric antigen receptors on their surface are now able to recognize a specific antigen on tumor cells. These engineered CAR T-cells (CTL019) which are grown in vitro, are then infused into the patient and they in turn proliferate in the patient’s body, recognize and kill cancer cells expressing that specific antigen. In a small study of patients with relapsed or refractory ALL, treatment with autologous Chimeric Antigen Receptor (CAR) T-cells (CTL019 T-cells) resulted in a 90% remission rate with sustained remissions for up to 2 years and overall survival of 78%.
ADVANCES IN TUMOR BIOLOGY
Genomic Profile Based Therapy – In a recent landmark study, analysis of molecular data from approximately 3,500 patients with 12 different forms of cancer, lead to the identification of 11 major molecular subtypes. It was noted that most malignancies that originated from the same tissue or organ had similar genomic profiles. Treatment in the foreseeable future may be based on genomic profile rather than site of origin of the malignancy.
Blood Test Predicts Resistance to Prostate Cancer Therapy – In patients with metastatic CRPC, the presence of Androgen Receptor Variant AR-V7 rather than a normal androgen receptor, in the circulating tumor cells (CTCs) before, during, and after treatment with either XTANDI® (Enzalutamide) or ZYTIGA® (Abiraterone), conferred resistance to these agents. The Androgen Receptor Variant AR-V7 was detected in roughly 40% of patients treated with XTANDI® and 20% of those treated with ZYTIGA®.
Gut Bacteria and Response to Therapy – Two early studies have demonstrated that Intestinal bacteria may be beneficial in priming and mobilizing immune cells to attack tumors. Further, certain chemotherapeutic agents such as CYTOXAN® (Cyclophosphamide) and ELOXATIN® (Oxaliplatin) were less effective when intestinal bacteria were eradicated with antibiotics.
ADVANCES IN PATIENT CARE
Early Initiation of Palliative Care Improves Patient Well Being – In a study of close to 500 patients with advanced cancer early palliative care improved, quality of life at the end of life, spiritual well-being, symptom severity, and satisfaction with care at 4 months after diagnosis.
Pregnancy After Breast Cancer Treatment – Premature Ovarian Failure (POF) is a common unintended consequence of chemotherapy in premenopausal women. Besides loss of fertility, which can influence treatment decisions in young women, ovarian failure can lead to menopausal symptoms, sexual dysfunction and loss of bone density. Two studies reported a promising new way of preserve fertility. In the POEMS (Prevention of Early Menopause Study) phase III trial, the addition of ZOLADEX® (Goserelin) to chemotherapy decreased the POF to 8% compared to 22% with chemotherapy alone (P=0.04). More women in the ZOLADEX® group achieved at least one pregnancy (21%) compared to 11% in the chemotherapy alone group (P=0.03). In a different study, similar findings were noted with the addition of another hormonal agent, TRELSTAR® (Triptorelin) to chemotherapy.
Masters GA, Krilov L, Bailey HH , et al. Published online before print January 20, 2015, doi: 10.1200/JCO.2014.59.9746
Cancers associated with BRCA1 and BRCA2 mutations other than Breast and Ovarian
SUMMARY:Approximately 5-10% of all Breast and Ovarian cancers are caused by inherited genetic factors and are typically the result from inherited mutations in either the BRCA1 or BRCA2 gene. BRCA1 and BRCA2 are tumor suppressor genes located on chromosome 17 and chromosome 13 respectively.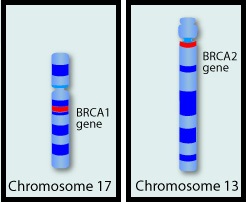 They control cell growth by repairing DNA damage and thus prevent tumor development. Mutations in these genes predispose an individual to develop malignant tumors. The presence of BRCA1 and BRCA2 mutations can significantly increase the lifetime risk for developing Breast and Ovarian cancer, as high as 85% and 40% respectively. While the association of BRCA1 and BRCA2 mutations with Breast and Ovarian cancer risks is well-established, the potential association of these mutations with other cancers has remained unclear. This study was conducted to evaluate the incidence of cancers other than Breast and Ovarian cancer, in known BRCA1 and BRCA2 mutation carriers. The study population included 1072 patients who had received genetic counseling at the UT MD Anderson Cancer Center between 1997 and 2013 and had a confirmed BRCA1 (N=613) or BRCA2 (N=459) mutation. The authors then compared the cancer incidence of the study population with the United States Cancer Statistics. The expected and observed numbers of cancer cases were calculated at 5 year intervals to take into consideration different age-related incidence rates. Standardized Incidence Ratios (SIRs) for each cancer type was then calculated for the entire sample and for BRCA1 mutation carriers and BRCA2 mutation carriers separately. {Standardized Incidence Ratio (SIR) is used to determine if the occurrence of cancer in a relatively small population is high or low. A SIR of 1 would indicate no increase or decrease, SIR of 1.5 indicates an excess of 50%, SIR of 2 indicates an excess of 100%}. Among the study population, 1177 cancers comprising 30 different cancer types were identified. There was no significant increase in cancers other than Breast and Ovarian cancer in individuals with BRCA1 mutation, but there was a trend of increasing incidence of Melanoma in BRCA1 mutation carriers, compared to general population. Individuals with BRCA2 mutation however had significantly higher incidence of Pancreatic cancer in both men and women (SIR= 21.7; P < 0.001), Prostate cancer in men (SIR= 4.9; P = 0.002) and a trend of increasing incidence of Cervical cancer, compared to general population. The authors concluded that their findings support the NCCN practice guidelines for this patient population which includes screening for male Breast cancer, Prostate cancer and Melanoma, acknowledging that specific screening guidelines for Pancreatic cancer do not exist. Mersch J, Jackson MA, Park M, et al. Cancer 2015; 121:269-275
They control cell growth by repairing DNA damage and thus prevent tumor development. Mutations in these genes predispose an individual to develop malignant tumors. The presence of BRCA1 and BRCA2 mutations can significantly increase the lifetime risk for developing Breast and Ovarian cancer, as high as 85% and 40% respectively. While the association of BRCA1 and BRCA2 mutations with Breast and Ovarian cancer risks is well-established, the potential association of these mutations with other cancers has remained unclear. This study was conducted to evaluate the incidence of cancers other than Breast and Ovarian cancer, in known BRCA1 and BRCA2 mutation carriers. The study population included 1072 patients who had received genetic counseling at the UT MD Anderson Cancer Center between 1997 and 2013 and had a confirmed BRCA1 (N=613) or BRCA2 (N=459) mutation. The authors then compared the cancer incidence of the study population with the United States Cancer Statistics. The expected and observed numbers of cancer cases were calculated at 5 year intervals to take into consideration different age-related incidence rates. Standardized Incidence Ratios (SIRs) for each cancer type was then calculated for the entire sample and for BRCA1 mutation carriers and BRCA2 mutation carriers separately. {Standardized Incidence Ratio (SIR) is used to determine if the occurrence of cancer in a relatively small population is high or low. A SIR of 1 would indicate no increase or decrease, SIR of 1.5 indicates an excess of 50%, SIR of 2 indicates an excess of 100%}. Among the study population, 1177 cancers comprising 30 different cancer types were identified. There was no significant increase in cancers other than Breast and Ovarian cancer in individuals with BRCA1 mutation, but there was a trend of increasing incidence of Melanoma in BRCA1 mutation carriers, compared to general population. Individuals with BRCA2 mutation however had significantly higher incidence of Pancreatic cancer in both men and women (SIR= 21.7; P < 0.001), Prostate cancer in men (SIR= 4.9; P = 0.002) and a trend of increasing incidence of Cervical cancer, compared to general population. The authors concluded that their findings support the NCCN practice guidelines for this patient population which includes screening for male Breast cancer, Prostate cancer and Melanoma, acknowledging that specific screening guidelines for Pancreatic cancer do not exist. Mersch J, Jackson MA, Park M, et al. Cancer 2015; 121:269-275
Clinical Cancer Advances 2015 Annual Report on Progress Against Cancer From the American Society of Clinical Oncology (PART I)
SUMMARY: Cancer mortality rates in the United States have declined 20% from their peak of 215 per 100,000 in 1991 to 172 per 100,000 in 2010. With more than half a million Americans diagnosed with cancer each year, recent advances in cancer treatment and research has lead to improved survival and better quality of life, with 14.5 million cancer survivors alive in the US today. This Annual Report on Progress Against Cancer explored the clinical advances of the prior year (2014), that made the greatest impact on improving cancer care. This report was developed based on research published in peer-reviewed scientific and medical journals and information presented at major scientific meetings over a one year period between October 2013 to September 2014. A brief summary of this report (Part I) is presented. Part I includes, ADVANCE OF THE YEAR and ADVANCES IN PREVENTION AND SCREENING. Clinical trial details for several of these studies can be accessed at www.oncoprescribe.com
ADVANCE OF THE YEAR – TREATMENT OF CHRONIC LYMPHOCYTIC LEUKEMIA
Chronic Lymphocytic Leukemia (CLL) is the most common form of adult leukemia and is more common in the elderly. Four new therapies associated with fewer toxicities compared with standard therapy, were recently approved for patients with CLL.
Two Effective Treatment Options for Patients with Newly Diagnosed CLL
GAZYVA® (Obinutuzumab) is a fully humanized, third generation, type II, anti-CD20 monoclonal antibody that selectivity binds to the extracellular domain of the CD20 antigen on malignant human B cells. In a phase III trial involving 589 treatment naïve CLL patients, GAZYVA® in combination with LEUKERAN® (Chlorambucil) more than doubled the Progression Free Survival (PFS) from 11.1 months with LEUKERAN® alone to 26.7 months (HR=0.18, P<0.001). The combination of GAZYVA® and LEUKERAN® also prolonged Overall Survival (OS) when compared to LEUKERAN® alone (HR=0.41; P=0.002). This benefit however was not noted with the RITUXAN® plus LEUKERAN® combination. Treatment with GAZYVA® plus LEUKERAN® when compared with RITUXAN® plus LEUKERAN® resulted in a longer PFS (26.7 vs15.2 months; HR=0.39; P<0.001), higher complete response rates (20.7% vs 7.0%) and deeper molecular responses.
ARZERRA® (Ofatumumab), a second generation fully human IgG 1 monoclonal antibody, which targets a different region (different epitope) of the CD20 molecule in combination with LEUKERAN®, was compared with LEUKERAN® alone, as first line treatment in a study involving 447 CLL patients. The median PFS was 22.4 months for patients receiving ARZERRA® in combination with LEUKERAN® compared with 13.1 months for those receiving single agent LEUKERAN® (HR=0.57, P< 0.001). The Objective Response Rate was higher with the combination regimen versus single agent LEUKERAN® (82% vs 69%, P=0.001).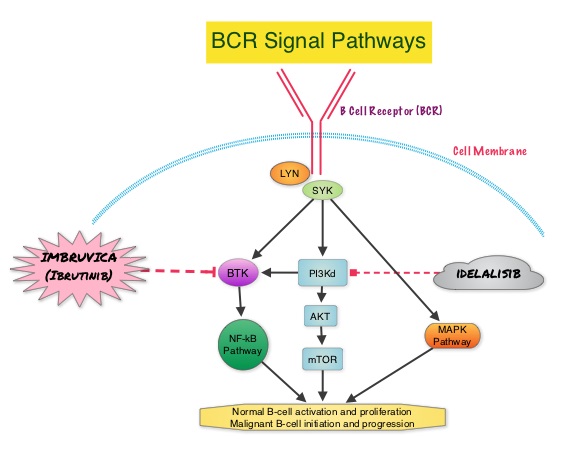
Two New Non-Chemotherapy Alternatives for Relapsed and Treatment-Resistant CLL
IMBRUVICA® (Ibrutinib) is an oral, irreversible inhibitor of BTK and inhibits cell proliferation and promotes programmed cell death (Apoptosis). IMBRUVICA® was compared to single agent ARZERRA® in a phase III trial involving 391 patients with relapsed CLL. Thirty percent (30%) of the patients had deletion of chromosome 17p. At a median follow up of 9.4 months, IMBRUVICA® significantly prolonged PFS compared to ARZERRA® (median not reached vs 8.1 months; HR 0.215, P<0.0001) with a 78.5% reduction in the risk of disease progression and also significantly improved OS (median not reached, HR 0.43, P=0.0049) when compared with ARZERRA®, with a 57% reduction in the risk of death.
In a phase III study involving 220 previously treated patients with recurrent CLL, ZYDELIG® (Idelalisib), a highly selective oral inhibitor of the enzyme PhosphoInositide 3-Kinase (PI3K) that specifically blocks the delta isoform of PI3K enzyme and its signaling pathway, was combined with RITUXAN® and compared with placebo given along with RITUXAN®. The median PFS with ZYDELIG® in combination with RITUXAN® was significantly prolonged compared with Placebo and RITUXAN® (10.7 months vs 5.5 months). An improvement in the Overall Survival (OS) was also noted in the ZYDELIG® group compared with patients in the RITUXAN® and placebo group (HR = 0.28; P = 0.018).
ADVANCES IN PREVENTION AND SCREENING
Breast Cancer Prevention
The only two drugs currently approved by the FDA to prevent breast cancer are NOLVADEX® (Tamoxifen) and EVISTA® (Raloxifene). These agents block the estrogen receptors and can be used in both pre and postmenopausal women. NOLVADEX® is however associated with thromboembolic evens as well as endometrial carcinoma. ARIMIDEX® (Anastrozole), an Aromatase Inhibitor (AI), in a randomized, double blind, placebo controlled trial, involving 3864 women at increased risk of breast cancer, reduced this risk of breast cancer by 53% compared to placebo, over a 5-year period (P<0.0001), in post-menopausal women. This benefit with ARIMIDEX® was accomplished without increase in the risk of heart attacks or fractures, compared with placebo. There was however increase in the incidence of joint and muscle pain as well as hot flushes and night sweats. Another AI, AROMASIN® (Exemestane) in a previously published study (MAP.3 trial) significantly reduced the incidence of all breast cancers by 53% and invasive breast cancers by 65%, after a median follow up of 3 years.
Screening for Lung Cancer
The United States Preventive Services Task Force (USPSTF) recommended annual screening for lung cancer with Low Dose Computed Tomography in adult individuals, between ages 55 to 80 years who have a 30 pack-year smoking history and currently smoke or have quit within the past 15 years. Screening should be discontinued once a person has not smoked for 15 years or develops a health problem that substantially limits life expectancy or the ability or willingness to have curative lung surgery. The use of Low Dose CT (LDCT) scans for 3 years in this high risk, healthy patients, resulted in a 20% reduction in Lung cancer mortality, compared to screening with a chest X-Ray in the NCI-sponsored National Lung Screening Trial (NLST).
Masters GA, Krilov L, Bailey HH, et al. Published online before print January 20, 2015, doi: 10.1200/JCO.2014.59.9746
Platelet Transfusion A Clinical Practice Guideline from the AABB
SUMMARY: Platelets are often transfused preemptively to reduce the risk for spontaneous bleeding in patients who are thrombocytopenic following chemotherapy or hematopoietic stem cell transplantation. In the United States, a little over 2 million platelet units are transfused annually. The risks associated with platelet transfusion such as febrile and allergic reactions, Transfusion Related Acute Lung Injury and infections, have to be taken into consideration before transfusion is planned. Further, unlike other blood products, platelets must be stored at room temperature and this limits the platelet unit shelf life to only 5 days, to prevent the risk for bacterial growth during storage. This in turn is an additional burden to the hospital blood banks. The AABB (American Association of Blood Banks) commissioned and funded the development of platelet transfusion guidelines with the help of 21 experts from various specialties of medicine, after a systematic review of 17 randomized controlled trials and 53 observational studies. A platelet unit in this guideline refers to 1 apheresis platelet unit or a pool of 4-6 whole blood derived platelet concentrates, containing approximately 3- 4 x 1011 platelets. Thrombocytopenia refers to a platelet count below the lower limit of the normal range used by the laboratory performing the count. Six recommendations were made for 4 different clinical settings.
Hospitalized Adult Patients with Therapy-Induced Hypoproliferative Thrombocytopenia
Recommendation 1: The AABB recommends that platelets should be transfused prophylactically to reduce the risk for spontaneous bleeding in hospitalized adult patients with therapy-induced hypoproliferative thrombocytopenia. The AABB recommends transfusing hospitalized adult patients with a platelet count of 10 × 109 cells/L or less to reduce the risk for spontaneous bleeding. The AABB recommends transfusing up to a single apheresis unit or equivalent. Greater doses are not more effective, and lower doses equal to one half of a standard apheresis unit are equally effective.
Adult Patients Having Minor Invasive Procedures
Recommendation 2: The AABB suggests prophylactic platelet transfusion for patients having elective central venous catheter placement with a platelet count less than 20 × 109 cells/L.
Recommendation 3: The AABB suggests prophylactic platelet transfusion for patients having elective diagnostic lumbar puncture with a platelet count less than 50 × 109 cells/L.
Adult Patients Having Major Elective Non-neuraxial Surgery
Recommendation 4: The AABB suggests prophylactic platelet transfusion for patients having major elective non-neuraxial surgery with a platelet count less than 50 × 109 cells/L.
Recommendation 5: The AABB recommends against routine prophylactic platelet transfusion for patients who are non-thrombocytopenic and have cardiac surgery with cardiopulmonary bypass. The AABB suggests platelet transfusion for patients having bypass who exhibit perioperative bleeding with thrombocytopenia and/or evidence of platelet dysfunction.
Adult Patients Receiving Antiplatelet Therapy Who Have Intracranial Hemorrhage (Traumatic or Spontaneous)
Recommendation 6: The AABB cannot recommend for or against platelet transfusion for patients receiving antiplatelet therapy who have intracranial hemorrhage (traumatic or spontaneous).
The authors acknowledge that the platelet transfusion threshold recommendations made by the various medical specialty societies, may be different, but the evidence based recommendations provided herein, will complement clinical judgment, as individualized decisions are made, to transfuse platelets. Kaufman RM, Djulbegovic B, Gernsheimer T, et al. Ann Intern Med. 2015;162:205-213.
The Second ASH CHOOSING WISELY® Campaign Five Hematologic Tests and Treatments to Question
SUMMARY: CHOOSING WISELY® is a quality improvement initiative led by the American Board of Internal Medicine Foundation in collaboration with leading medical societies in the United States such as the American Society of Hematology (ASH). This organization was established to improve quality of medical care, after it was noted that about 25% of the tests ordered at the time of hospital admission and 65% of the tests ordered on subsequent days were avoidable. Further, there is ample evidence to suggest that reducing unneeded investigations can decrease costs, increase patient satisfaction and quality of care. CHOOSING WISELY® has challenged medical societies to identify 5 tests, procedures or treatments, within each specialty's clinical domain, that are offered to patients, despite the lack of evidence demonstrating its benefit. The goal is to make positive changes in the actual delivery of patient care. The 2014 Task Force was comprised of 13 individuals representing a broad spectrum of hematologic expertise including malignant, benign, adult, and pediatric specialists. The five final recommendations of the 2014 ASH Choosing Wisely Campaign are summarized below. Practicing hematologists should give due consideration to these recommendations which are evidence based and cost effective.
ASH recommendation #1: In patients with a first VTE (Venous ThromboEmbolism) provoked by a major, transient VTE risk factor such as surgery, trauma, or an intravascular catheter, do not treat with an anticoagulant for more than 3 months. There is a low risk of VTE recurrence after three months in this setting and anticoagulation for VTE continued beyond three months may be associated with increased bleeding risk, particularly in the elderly and those with comorbidities. This recommendation is not applicable to patients with non-major, transient VTE risk factors such as travel-associated immobility, pregnancy or hormone use. Women who experience a first VTE during pregnancy should receive anticoagulation until at least six weeks post-partum, for a minimum total duration of three months or longer. VTEs occurring in the context of estrogen supplements are associated with a low recurrence rate following discontinuation of hormonal therapy/oral contraceptives and three months of anticoagulation may be adequate. However, the optimal duration of anticoagulation for VTEs provoked by hormones or by travel remains unclear and should be determined on a on a case-by-case basis.
ASH recommendation #2: Routine transfusion of PRBC for chronic anemia or uncomplicated pain crises in patients with sickle cell disease is not recommended as these patients who are predominantly African Americans, are at an especially higher risk for alloimmunization to minor blood group antigens, which can result in delayed-hemolytic transfusion reactions, as well as difficulty finding compatible blood when necessary. The baseline hemoglobin values range between 7 and 10g/dL in stable patients with severe sickle cell disease and these patients are often able to tolerate a 1-2g/dL decreases in their hemoglobin values following IV hydration. Further, data does not strongly support that episodic red cell transfusion reduces pain during acute vaso-occlusive crises. Moreover, iron overload from repeated transfusions can cause significant morbidity and mortality in patients with sickle cell disease.
ASH recommendation #3: Unlike in other lymphoproliferative diseases, routine surveillance CT scans are not recommended in patients with asymptomatic, early stage chronic lymphocytic leukemia (CLL). Both the Rai and Binet staging systems are based on physical exam findings and complete blood counts and prognosis can be assessed with molecular mutational analyses. CT scans are therefore not necessary and can be potentially harmful, by exposing patients to radiation and may also trigger additional workup to evaluate incidental findings (Cascade effect), that may not be of importance.
ASH recommendation #4: Do not test or treat for suspected Heparin-Induced Thrombocytopenia (HIT) in patients with a Low pretest probability of HIT. The 4Ts is a pretest scoring system for HIT and incorporates 4 components of HIT which include magnitude of thrombocytopenia, timing of thrombocytopenia with respect to heparin exposure, thrombosis or other sequelae of HIT and likelihood of other causes of thrombocytopenia. The 4Ts score is the sum of the values for each of the 4 categories. A score of 0-3 is classified as Low, 4-5 as Intermediate and 6-8 as High pretest probability for HIT. The negative predictive value of a Low 4T’s score is close to 100% in adults. Further, Enzyme ImmunoAssays (EIA) for HIT have a high false positive rate and a positive EIA HIT test results in a patient with a Low 4T’s score is much more likely to represent a false positive value than true positive. Confirmatory testing with serotonin release assays are not easily available and can be expensive. Misdiagnosing HIT can harm patients by denying them a heparin preparation in the future and the use of alternative, expensive anticoagulants such as Argatroban in these thrombocytopenic patients can be associated with a higher risk of bleeding. For these reasons, testing for HIT is only cost-effective when the pre-test probability of HIT is greater than 8%, which corresponds to an Intermediate or High 4T’s score
ASH recommendation #5: Do not treat patients with Immune Thrombocytopenic Purpura (ITP) in the absence of bleeding or a very low platelet count. ITP is often a temporary condition in children and resolves without treatment and treatment is not recommended in childhood ITP unless there is bleeding or risk factors for bleeding. ITP in adults is usually a chronic disease with remissions and exacerbations and patients with a platelet count of 30,000/microL or more and with no bleeding, can be observed without intervention. Steroids can impair glucose metabolism, increase infection risk, cause adrenal suppression and in children can cause growth impairment. Splenectomy is associated with perioperative risks and small risk of life threatening infections. Rituximab can cause Hepatitis B reactivation and TPO receptor agonists are only cost-effective in the setting of severe ITP, refractory to other treatment interventions.
Hicks LK, Bering H, Carson KR, et al. Prepublished online December 3, 2014; doi:10.1182/blood-2014-09-599399