SUMMARY: Radiation Therapy involves the use of X-Rays, gamma rays and charged particles for cancer treatment. External-beam radiation therapy is most often delivered using a linear accelerator in the form of Photon beams (either x-rays or gamma rays). Photons have no mass and are packets of energy of an electromagnetic wave. Electrons and Protons are charged particles and Electrons are considered light particles whereas Protons are considered heavy particles. Electron beams are used to irradiate skin and superficial tumors, as they are unable to penetrate deep into the tissues.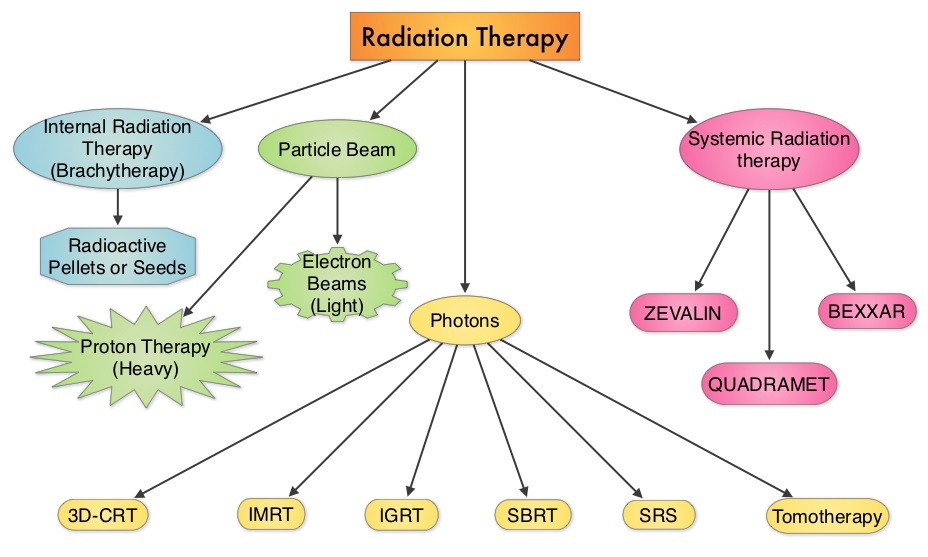 The different types of external beam radiation treatments include 3-Dimensional Conformal Radiation Therapy (3D-CRT) meant to deliver radiation to very precisely shaped target areas, IMRT or Intensity Modulated Radiation Therapy which allows different areas of a tumor or nearby tissues to receive different doses of radiation, Image Guided Radiation Therapy (IGRT) which allows reduction in the planned volume of tissue to be treated as changes in a tumor size are noted during treatment, Stereotactic RadioSurgery (SRS) which can deliver one or more high doses of radiation to a small tumor, Stereotactic Body Radiation Therapy (SBRT) or CYBERKNIFE® which is similar to SRS but also takes the normal motion of the body into account while treating malignancies involving the lung and liver and Proton Beam therapy. Proton beams unlike Photons, enter the skin and travel through the tissues and deposit much of their energy at the end of their path (known as the Bragg peak) and deposit less energy along the way. This is unlike Photons which deposit energy all along the path through the tissues and the deposited dose decreases with increasing depth. As a result, with Proton beam therapy, normal tissues are exposed to less radiation compared with Photons. Despite this advantage, tissue heterogeneity such as organ motion, tumor volume changes during treatment can have a significant negative impact on target coverage for Proton beam therapy and can result in damage to the surrounding tissues and potential complications. The authors in this review discussed the clinical applications of Proton therapy in Adult and Pediatric malignancies. Pediatric patients with malignancies have greater benefit with Proton beam therapy, with a statistically significant lower risk of secondary malignancies and less damage to the developing tissues and organs, compared to Photon therapy (External Beam Radiation Therapy). This clinical benefit may be less so in adult malignancies in spite of superior dosimetry, compared to external beam radiation, as adults are less prone to secondary malignancies compared to children.
The different types of external beam radiation treatments include 3-Dimensional Conformal Radiation Therapy (3D-CRT) meant to deliver radiation to very precisely shaped target areas, IMRT or Intensity Modulated Radiation Therapy which allows different areas of a tumor or nearby tissues to receive different doses of radiation, Image Guided Radiation Therapy (IGRT) which allows reduction in the planned volume of tissue to be treated as changes in a tumor size are noted during treatment, Stereotactic RadioSurgery (SRS) which can deliver one or more high doses of radiation to a small tumor, Stereotactic Body Radiation Therapy (SBRT) or CYBERKNIFE® which is similar to SRS but also takes the normal motion of the body into account while treating malignancies involving the lung and liver and Proton Beam therapy. Proton beams unlike Photons, enter the skin and travel through the tissues and deposit much of their energy at the end of their path (known as the Bragg peak) and deposit less energy along the way. This is unlike Photons which deposit energy all along the path through the tissues and the deposited dose decreases with increasing depth. As a result, with Proton beam therapy, normal tissues are exposed to less radiation compared with Photons. Despite this advantage, tissue heterogeneity such as organ motion, tumor volume changes during treatment can have a significant negative impact on target coverage for Proton beam therapy and can result in damage to the surrounding tissues and potential complications. The authors in this review discussed the clinical applications of Proton therapy in Adult and Pediatric malignancies. Pediatric patients with malignancies have greater benefit with Proton beam therapy, with a statistically significant lower risk of secondary malignancies and less damage to the developing tissues and organs, compared to Photon therapy (External Beam Radiation Therapy). This clinical benefit may be less so in adult malignancies in spite of superior dosimetry, compared to external beam radiation, as adults are less prone to secondary malignancies compared to children.
ADULT MALIGNANCIES
Prostate Cancer: Majority of the patients receiving Proton beam treatment in the United States have prostate cancer. Several randomized trials have concluded that higher radiation dose to the prostate gland leads to better tumor control. Proton beam therapy may deliver this promise, but with associated toxicities, in particular rectal bleeding. This is by virtue of the anatomy of the prostate gland which is deep in the pelvis. Outcomes and patient reported side effects were similar when men with prostate cancer were treated with similar doses of radiation using either Proton beam therapy or External beam radiation therapy. The American Society of Therapeutic Radiology and Oncology (ASTRO) has recommended that Proton beam therapy for patients with prostate cancer should be offered in the context of a clinical trial or registry, as there is not enough evidence suggesting clinical benefit in this patient population.
Breast Cancer: Proton beam therapy may be of value in select situations, such as patients with bilateral implants after mastectomy and in clinical scenarios where cardiac or pulmonary risks with Photon therapy are not acceptable. This is because of a significant reduction in the radiation doses to the heart, lung and contralateral breast with Proton therapy compared to Photon therapy.
Lung Cancer: Proton beam therapy for NSCLC (Non Small Cell Lung Cancer) is in the early stages of evaluation and has the advantage of reduced radiation to the normal lung and heart. This may be relevant in patients with inoperable early stage NSCLC with poor lung function, prior chest irradiation or in those with multifocal lung cancers requiring more than one treatment course. Proton therapy can be of significant value in patients with Stage IIIA NSCLC who in addition to chemoradiation may be candidates for pneumonectomy, thus sparing the contralateral lung from radiation related toxicities.
Head and Neck Cancers: Proton therapy may be of value in nasopharyngeal carcinoma and malignancies involving the oropharynx and paranasal sinuses. Proton therapy limits the radiation dose to the brain stem, optic structures, mandible and salivary glands, decreasing the risk of xerostomia and osteoradionecrosis of the mandible.
GI Malignancies: Proton beam therapy is the preferable treatment for hepatocellular carcinoma in patients with Child-Pugh class B and class C cirrhosis, as it is able to spare more liver tissue from radiation.
Brain Tumors: Meningiomas are ideal tumors for Proton beam therapy, with less cerebral adverse events and therefore has a positive impact on quality of life of patients. Clinical trials are underway to test this hypothesis.
PEDIATRIC TUMORS
Medulloblastoma- CranioSpinal Irradiation: There is a significant long term advantage with Proton CranioSpinal Irradiation compared to conventional or IMRT photon CSI. There is a 6-12 times lower risk of secondary malignancies due to lower radiation doses to normal tissues. This is more relevant because craniospinal axis irradiation results in the most exposure of a childs tissue to radiation.
Rhabdomyosarcoma: This is the most common soft tissue sarcoma in children arising in the head and neck region and Proton therapy can significantly reduce the mean doses to the retina, optic nerve, parotid and cochlea.
Ependymoma, Craniopharyngioma, Retinoblastoma and Glioma: Proton therapy for these tumors has been associated with lower acute and long term toxicities as well lower risk of secondary malignancies.
The authors concluded that the most benefit for Proton beam therapy is in pediatric malignancies, no significant benefit in skin cancer and marginal benefit in adult lung and prostate cancer. With ongoing advances in the delivery of Proton therapy such as Intensity Modulated Proton Therapy (IMPT) and other expensive therapeutic interventions, economics will take precedence, until and unless a clear clinical benefit is proven. Mitin T and Zietman AL. J Clin Oncol 2014;32:2855-2863
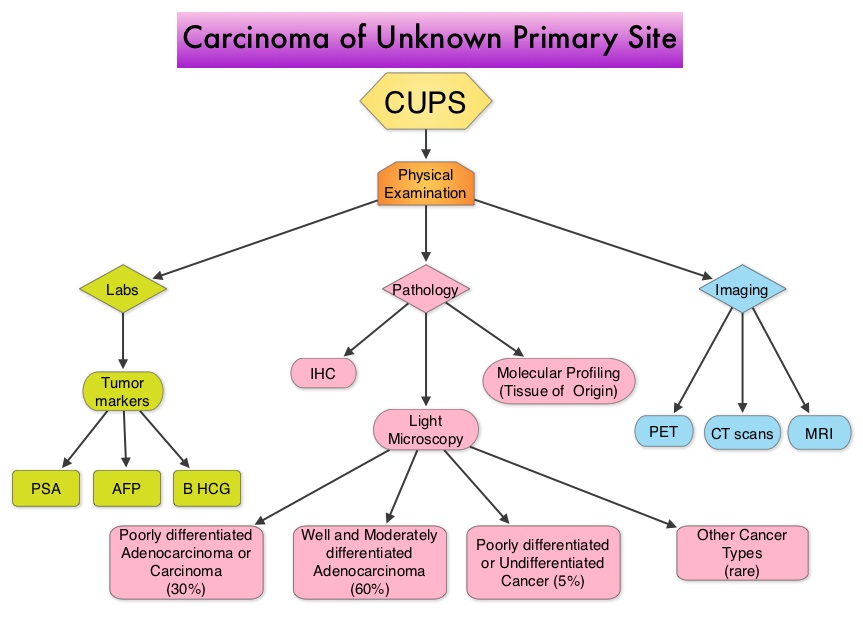 Evaluation of a patient with CUPS starts with gathering and incorporating medical information which includes the patient’s gender, medical history, clinical findings and sites of metastases. A CT scan of the chest, abdomen and pelvis with IV and oral contrast is recommended, although PET (Positron Emission Tomography) or an MRI can be performed in those with renal insufficiency or iodine allergy. PET scan is recommended for those with cervical lymphadenopathy with squamous histology, to help determine the extent of the disease and treatment planning for radiation. PET imaging is also helpful for patients with solitary metastases before locoregional therapies are planned, as well as assessing response in patients with predominantly bone only disease. In women presenting with isolated axillary lymphadenopathy, adenocarcinoma histology, negative mammograms and ultrasound, MRI of the breasts is indicated. With the exception of those patients with CUPS who present with cervical lymphadenopathy, diagnostic procedures such as bronchoscopy, EGD and colonoscopy are not recommended in asymptomatic patients. Tumor markers in general do not have diagnostic value in patients with CUPS although they could be utilized to monitor response to treatment. However, PSA when elevated in a male with adenocarcinoma and osteoblastic metastases, is suggestive of a prostate primary. Similarly an elevated Beta HCG and AFP in a patient with undifferentiated or poorly differentiated carcinoma, is suggestive of an extragonadal germ cell tumor and an elevated AFP is also helpful in making a diagnosis of Hepatoma. Approximately 60% of the patients with CUPS have well or moderately differentiated adenocarcinoma on light microscopy, 30% have poorly differentiated carcinoma or adenocarcinoma, 5% have poorly differentiated or undifferentiated malignancy and 5% have squamous cell carcinoma. Following histological evaluation on light microscopy, the biopsy specimen is further tested using ImmunoHistoChemical stains, using peroxidase labeled antibodies against tumor specific antigens, taking advantage of the similarities in the tumor profiles of primary and metastatic malignancies. After delineating a tumor as carcinoma, lymphoma, sarcoma or melanoma, additional IHC testing can help identify tumors such as a lung primary (postive Thyroid Transcription Factor 1-TTF1and positive CytoKeratin 7- CK7), lower gastrointestinal cancers (positive CK20, positive CDX2 and negative CK7) or a breast primary (positive CK7 and positive Mammaglobin). Tissue-of-Origin molecular profiling is based on the principle that in patients with CUPS, molecular signatures of metastatic tumors are similar to their primary tumor. Tissue-of-Origin molecular profiling is performed using tools such as DNA microarray, quantitative real time polymerase chain reaction assay (rt-PCR) or assays based on messenger RNA (mRNA) or microRNA. These tests are cost-effective and 70% – 90% accurate. This study can be performed on formalin-fixed samples as well as samples from fine needle aspiration. Even though platinum based chemotherapy has been the default regimen for patients with CUPS, histological evaluation of biopsy tissue by light microscopy, IHC testing and molecular profiling assay may complement each other and help guide the Health Care Provider to select site specific therapy. The survival outcomes of CUPS patients with a Tissue-of-Origin molecularly diagnosed profile are comparable to those with similar type advanced cancer with a known primary. The authors concluded that with additional molecular insights into tumor biology and availability of newer therapeutic agents, patients with CUPS and known primary tumors may eventually be treated alike. Varadhachary, GR and Raber, MN. N Engl J Med 2014; 371:757-765
Evaluation of a patient with CUPS starts with gathering and incorporating medical information which includes the patient’s gender, medical history, clinical findings and sites of metastases. A CT scan of the chest, abdomen and pelvis with IV and oral contrast is recommended, although PET (Positron Emission Tomography) or an MRI can be performed in those with renal insufficiency or iodine allergy. PET scan is recommended for those with cervical lymphadenopathy with squamous histology, to help determine the extent of the disease and treatment planning for radiation. PET imaging is also helpful for patients with solitary metastases before locoregional therapies are planned, as well as assessing response in patients with predominantly bone only disease. In women presenting with isolated axillary lymphadenopathy, adenocarcinoma histology, negative mammograms and ultrasound, MRI of the breasts is indicated. With the exception of those patients with CUPS who present with cervical lymphadenopathy, diagnostic procedures such as bronchoscopy, EGD and colonoscopy are not recommended in asymptomatic patients. Tumor markers in general do not have diagnostic value in patients with CUPS although they could be utilized to monitor response to treatment. However, PSA when elevated in a male with adenocarcinoma and osteoblastic metastases, is suggestive of a prostate primary. Similarly an elevated Beta HCG and AFP in a patient with undifferentiated or poorly differentiated carcinoma, is suggestive of an extragonadal germ cell tumor and an elevated AFP is also helpful in making a diagnosis of Hepatoma. Approximately 60% of the patients with CUPS have well or moderately differentiated adenocarcinoma on light microscopy, 30% have poorly differentiated carcinoma or adenocarcinoma, 5% have poorly differentiated or undifferentiated malignancy and 5% have squamous cell carcinoma. Following histological evaluation on light microscopy, the biopsy specimen is further tested using ImmunoHistoChemical stains, using peroxidase labeled antibodies against tumor specific antigens, taking advantage of the similarities in the tumor profiles of primary and metastatic malignancies. After delineating a tumor as carcinoma, lymphoma, sarcoma or melanoma, additional IHC testing can help identify tumors such as a lung primary (postive Thyroid Transcription Factor 1-TTF1and positive CytoKeratin 7- CK7), lower gastrointestinal cancers (positive CK20, positive CDX2 and negative CK7) or a breast primary (positive CK7 and positive Mammaglobin). Tissue-of-Origin molecular profiling is based on the principle that in patients with CUPS, molecular signatures of metastatic tumors are similar to their primary tumor. Tissue-of-Origin molecular profiling is performed using tools such as DNA microarray, quantitative real time polymerase chain reaction assay (rt-PCR) or assays based on messenger RNA (mRNA) or microRNA. These tests are cost-effective and 70% – 90% accurate. This study can be performed on formalin-fixed samples as well as samples from fine needle aspiration. Even though platinum based chemotherapy has been the default regimen for patients with CUPS, histological evaluation of biopsy tissue by light microscopy, IHC testing and molecular profiling assay may complement each other and help guide the Health Care Provider to select site specific therapy. The survival outcomes of CUPS patients with a Tissue-of-Origin molecularly diagnosed profile are comparable to those with similar type advanced cancer with a known primary. The authors concluded that with additional molecular insights into tumor biology and availability of newer therapeutic agents, patients with CUPS and known primary tumors may eventually be treated alike. Varadhachary, GR and Raber, MN. N Engl J Med 2014; 371:757-765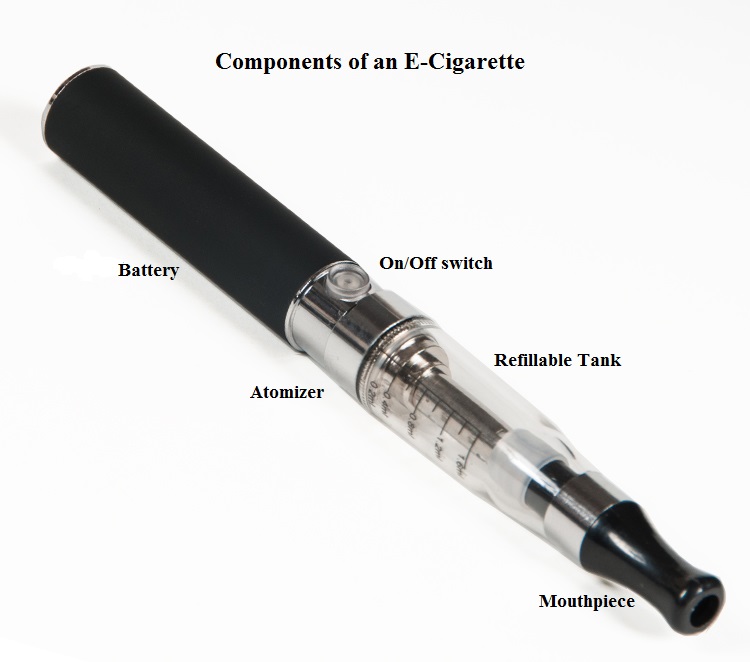 When a smoker inhales through the mouth piece of an E-cigarette, the air flow triggers a sensor that switches on a small lithium battery powered heater, which in turn vaporizes liquid nicotine along with PolyEthylene Glycol (PEG) present in a small cartridge. The PEG vapor looks like smoke. The potent liquid form of nicotine extracted from tobacco is tinctured with fragrant flavors such as chocolate, cherry and bubble gum, coloring substances, as well other chemicals and these e-liquids are powerful neurotoxins. With the rapid growth of the E-cigarette industry and the evidence of potential dangers and risk to public health, particularly children, experts from the world's leading lung organizations were compelled to release a position statement on electronic cigarettes, specifically focusing on their potential adverse effects on human health and calling on government organizations to ban or restrict the use of E-cigarettes, until their impact on health is better understood. With epidemiological data demonstrating that nicotine use is a gateway to the use of cocaine and marijuana and subsequent lifelong addiction, the Forum of International Respiratory Societies (FIRS), an organization composed of the world's leading international respiratory societies including American Thoracic Society (ATS) and the American College of Chest Physicians (ACCP), made the following recommendations. The position statement of the Forum of International Respiratory Societies (FIRS) on electronic nicotine delivery devices includes the following:
When a smoker inhales through the mouth piece of an E-cigarette, the air flow triggers a sensor that switches on a small lithium battery powered heater, which in turn vaporizes liquid nicotine along with PolyEthylene Glycol (PEG) present in a small cartridge. The PEG vapor looks like smoke. The potent liquid form of nicotine extracted from tobacco is tinctured with fragrant flavors such as chocolate, cherry and bubble gum, coloring substances, as well other chemicals and these e-liquids are powerful neurotoxins. With the rapid growth of the E-cigarette industry and the evidence of potential dangers and risk to public health, particularly children, experts from the world's leading lung organizations were compelled to release a position statement on electronic cigarettes, specifically focusing on their potential adverse effects on human health and calling on government organizations to ban or restrict the use of E-cigarettes, until their impact on health is better understood. With epidemiological data demonstrating that nicotine use is a gateway to the use of cocaine and marijuana and subsequent lifelong addiction, the Forum of International Respiratory Societies (FIRS), an organization composed of the world's leading international respiratory societies including American Thoracic Society (ATS) and the American College of Chest Physicians (ACCP), made the following recommendations. The position statement of the Forum of International Respiratory Societies (FIRS) on electronic nicotine delivery devices includes the following: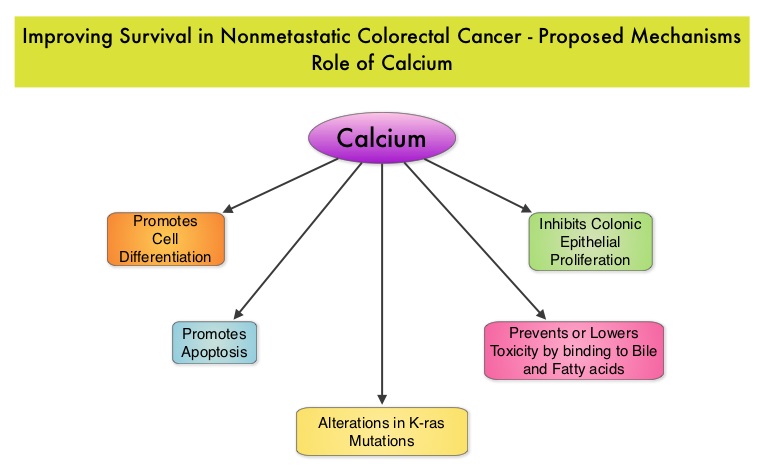 Milk, in addition to being a rich source of dietary Calcium and Vitamin D is a primary dietary source of conjugated linoleic acid which has been shown to inhibit colon cancer cell growth. Dairy products also provide other beneficial components such as butyric acid, lactoferrin and fermentation products. The impact of milk and dairy products on CRC survival however has remained unclear. The Cancer Prevention Study – II Nutrition Cohort is a prospective study of cancer incidence that began in 1992. Participants in this study (N=184,000) were provided a self administered questionnaire and baseline information about their dietary habits (including dietary Calcium and Vitamin D, as well as Calcium, Vitamin D and multivitamin supplements), physical activity, body size, cancer screening and early detection, etc. was collected and follow up questionnaires were sent every other year to update information and learn about new cancer diagnosis. Patients were followed up until June 2009 and by the end of this period, 3,832 individuals who had no history of disease at baseline had been diagnosed with invasive colon or rectal cancer. After excluding patients with distant metastatic disease, 2,284 patients were included in this analysis and among them, 1,111 patients reported post diagnosis diet. The primary outcome of this study was all cause mortality and the secondary outcome was mortality resulting from colorectal cancer. Using standard statistical models, the investigators noted that post CRC diagnosis total Calcium intake and milk intake, was inversely associated with all-cause mortality and significantly reduced CRC specific mortality.
Milk, in addition to being a rich source of dietary Calcium and Vitamin D is a primary dietary source of conjugated linoleic acid which has been shown to inhibit colon cancer cell growth. Dairy products also provide other beneficial components such as butyric acid, lactoferrin and fermentation products. The impact of milk and dairy products on CRC survival however has remained unclear. The Cancer Prevention Study – II Nutrition Cohort is a prospective study of cancer incidence that began in 1992. Participants in this study (N=184,000) were provided a self administered questionnaire and baseline information about their dietary habits (including dietary Calcium and Vitamin D, as well as Calcium, Vitamin D and multivitamin supplements), physical activity, body size, cancer screening and early detection, etc. was collected and follow up questionnaires were sent every other year to update information and learn about new cancer diagnosis. Patients were followed up until June 2009 and by the end of this period, 3,832 individuals who had no history of disease at baseline had been diagnosed with invasive colon or rectal cancer. After excluding patients with distant metastatic disease, 2,284 patients were included in this analysis and among them, 1,111 patients reported post diagnosis diet. The primary outcome of this study was all cause mortality and the secondary outcome was mortality resulting from colorectal cancer. Using standard statistical models, the investigators noted that post CRC diagnosis total Calcium intake and milk intake, was inversely associated with all-cause mortality and significantly reduced CRC specific mortality.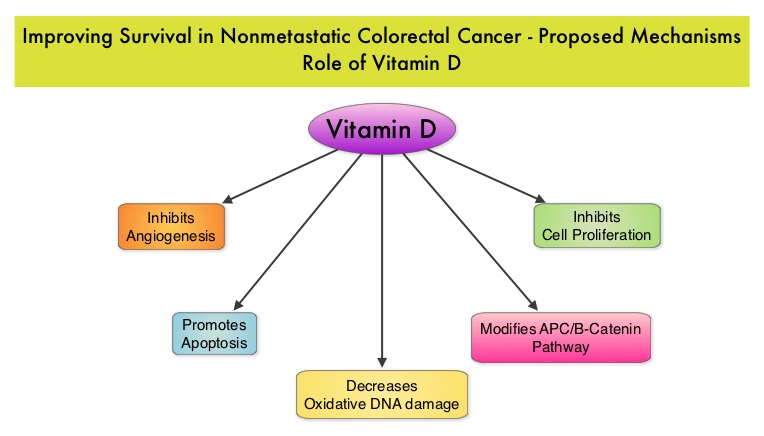 This benefit however, was not seen with Vitamin D intake. Also of interest, pre-diagnosis Calcium, Vitamin D, and dairy product intakes did not influence mortality outcomes. The authors concluded that higher post-diagnosis intakes of total Calcium and milk may be associated with lower risk of death among patients with non-metastatic ColoRectal Cancer. In a more recent publication, it has been reported that there is a strong association between plasma level of 25-hydroxyvitamin D (25-OHD) and CRC specific mortality, with better outcomes in patients with Stage I-III CRC, who had higher plasma levels of 25-OHD (Zgaga L, et al. J Clin Oncol 2014;32:2430-2439). With 30-35% of the malignancies attributed to dietary habits, the onus is therefore on the treating physicians to provide nutrition counseling during and after cancer treatment and is not to be ignored. Yang B, McCullough ML, Gapstur SM, et al. J Clin Oncol 2014;32:2335-2343
This benefit however, was not seen with Vitamin D intake. Also of interest, pre-diagnosis Calcium, Vitamin D, and dairy product intakes did not influence mortality outcomes. The authors concluded that higher post-diagnosis intakes of total Calcium and milk may be associated with lower risk of death among patients with non-metastatic ColoRectal Cancer. In a more recent publication, it has been reported that there is a strong association between plasma level of 25-hydroxyvitamin D (25-OHD) and CRC specific mortality, with better outcomes in patients with Stage I-III CRC, who had higher plasma levels of 25-OHD (Zgaga L, et al. J Clin Oncol 2014;32:2430-2439). With 30-35% of the malignancies attributed to dietary habits, the onus is therefore on the treating physicians to provide nutrition counseling during and after cancer treatment and is not to be ignored. Yang B, McCullough ML, Gapstur SM, et al. J Clin Oncol 2014;32:2335-2343
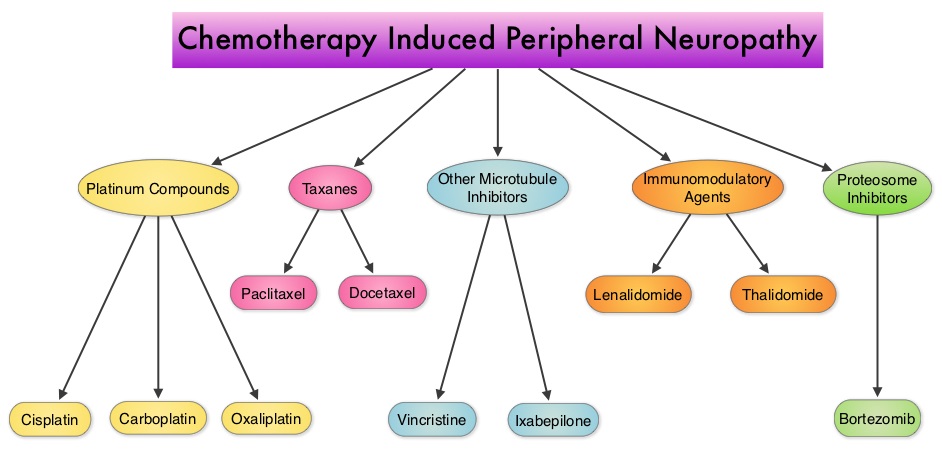 The following chemotherapeutic agents are associated with varying degrees of peripheral neuropathy – Platinum compounds (Cisplatin, Carboplatin and Oxaliplatin), Taxanes (Paclitaxel, Docetaxel), Immunomodulatory agents (Thalidomide, Lenalidomide), Other Microtubule inhibitors (Vincristine, Ixabepilone) and Proteosome Inhibitors (Bortezomib). It may be necessary to screen and rescreen patients for neuropathic pain, as patients may not be forthcoming with this complaint. Management of Neuropathic pain may include systemic treatment with adjuvant analgesics, topical therapies and psychosocial support. The management of Chemotherapy Induced Peripheral Neuropathy has mostly been extrapolated from validated studies on diabetic neuropathy. The first line treatment for Chemotherapy Induced Neuropathic Pain includes antidepressants and anticonvulsants, which if not effective on their own, can be combined with opioids. TriCyclic Antidepressants (TCA’s) such as Amitriptyline and Nortriptyline (PAMELOR®) can be considered as first line choice for appropriate patients, although its mechanism of action is uncertain and 20% of the patients discontinue therapy because of adverse effects.
The following chemotherapeutic agents are associated with varying degrees of peripheral neuropathy – Platinum compounds (Cisplatin, Carboplatin and Oxaliplatin), Taxanes (Paclitaxel, Docetaxel), Immunomodulatory agents (Thalidomide, Lenalidomide), Other Microtubule inhibitors (Vincristine, Ixabepilone) and Proteosome Inhibitors (Bortezomib). It may be necessary to screen and rescreen patients for neuropathic pain, as patients may not be forthcoming with this complaint. Management of Neuropathic pain may include systemic treatment with adjuvant analgesics, topical therapies and psychosocial support. The management of Chemotherapy Induced Peripheral Neuropathy has mostly been extrapolated from validated studies on diabetic neuropathy. The first line treatment for Chemotherapy Induced Neuropathic Pain includes antidepressants and anticonvulsants, which if not effective on their own, can be combined with opioids. TriCyclic Antidepressants (TCA’s) such as Amitriptyline and Nortriptyline (PAMELOR®) can be considered as first line choice for appropriate patients, although its mechanism of action is uncertain and 20% of the patients discontinue therapy because of adverse effects.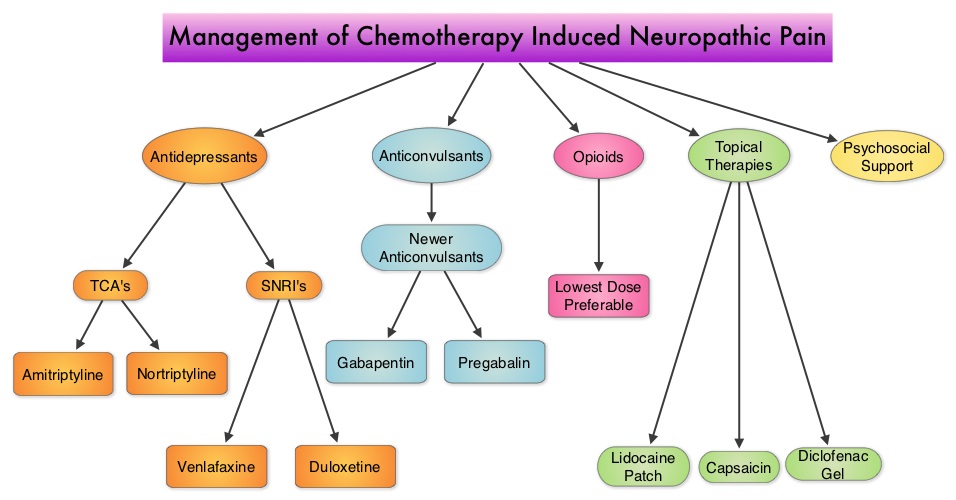 Patients may be able to better tolerate these agents if started at a lower dose and dose titrated slowly every three to five days. Peripheral neuropathic pain has been attributed to an unbalanced release of norepinephrine and serotonin from the neurons. Serotonin-Norepinephrine Reuptake Inhibitors (SNRI’s), including Venlafaxine (EFFEXOR®) and Duloxetine (CYMBALTA®), are better tolerated and have fewer drug interactions than TCA’s. EFFEXOR® in one study significantly relieved Oxaliplatin induced neuropathic pain in more than two thirds of the patients when compared to placebo and a third of the patients had complete pain relief. There is however limited evidence showing a beneficial role of Selective Serotonin Reuptake Inhibitors (SSRI’s) such as Citalopram (CELEXA®) and Paroxetine (PAXIL®) for neuropathic pain. As a note of caution, SNRI’s such as EFFEXOR® and CYMBALTA®, can interact with Tamoxifen, prescribed to patients with breast cancer, preventing Tamoxifen from converting to its active form. The dose of antidepressants needed to alleviate neuropathic pain is not dependent on antidepressant activity and may be lower than that recommended for treatment of depression. The newer anticonvulsants such as Gabapentin (NEURONTIN®), Pregabalin (LYRICA®) are preferable first line agents for the treatment of neuropathic pain rather than traditional, older agents such as Carbamazepine (TEGRETOL®), Phenytoin (DILANTIN®) and Valproate (DEPAKOTE®), as the newer agents are associated with fewer drug interactions. The newer agents bind to the alpha2-delta subunit of the calcium-sensitive channels, modulating neurotransmitter release. Of the newer agents, NEURONTIN® (Gabapentin) is not protein bound and is excreted unchanged in the urine and therefore has fewer drug interactions. If opioids are a consideration for neuropathic pain relief, the lowest dose is recommended. Topical therapies for neuropathic pain have the advantage of controlling pain without systemic side effects. It therefore can be combined with systemic treatment. Lidocaine 5% patches (LIDODERM®) block neuronal sodium channels whereas Capsaicin cream (ZOSTRIX®) stimulates the C fibers to release and subsequently deplete substance P, there by blocking pain signaling to the brain. Diclofenac gel 1% when applied once a day, concentrates in the dermis and has less gastrointestinal side effects and may be beneficial for neuropathic pain. A combination of Ketamine 1% and Amitriptyline 2% cream applied topically has also been promising in a small study. Patients experiencing refractory pain may benefit with the use of Transcutaneous Electrical Nerve Stimulation (TENS), although referral to the pain clinic may be appropriate. Psychosocial support utilizing a team of specialists and social workers/counsellors, should be an integral part of pain management. Kvale E and Urba SG. National Comprehensive Cancer Network (NCCN) 19th Annual Conference, March 13 – 15, 2014; Hollywood, Florida
Patients may be able to better tolerate these agents if started at a lower dose and dose titrated slowly every three to five days. Peripheral neuropathic pain has been attributed to an unbalanced release of norepinephrine and serotonin from the neurons. Serotonin-Norepinephrine Reuptake Inhibitors (SNRI’s), including Venlafaxine (EFFEXOR®) and Duloxetine (CYMBALTA®), are better tolerated and have fewer drug interactions than TCA’s. EFFEXOR® in one study significantly relieved Oxaliplatin induced neuropathic pain in more than two thirds of the patients when compared to placebo and a third of the patients had complete pain relief. There is however limited evidence showing a beneficial role of Selective Serotonin Reuptake Inhibitors (SSRI’s) such as Citalopram (CELEXA®) and Paroxetine (PAXIL®) for neuropathic pain. As a note of caution, SNRI’s such as EFFEXOR® and CYMBALTA®, can interact with Tamoxifen, prescribed to patients with breast cancer, preventing Tamoxifen from converting to its active form. The dose of antidepressants needed to alleviate neuropathic pain is not dependent on antidepressant activity and may be lower than that recommended for treatment of depression. The newer anticonvulsants such as Gabapentin (NEURONTIN®), Pregabalin (LYRICA®) are preferable first line agents for the treatment of neuropathic pain rather than traditional, older agents such as Carbamazepine (TEGRETOL®), Phenytoin (DILANTIN®) and Valproate (DEPAKOTE®), as the newer agents are associated with fewer drug interactions. The newer agents bind to the alpha2-delta subunit of the calcium-sensitive channels, modulating neurotransmitter release. Of the newer agents, NEURONTIN® (Gabapentin) is not protein bound and is excreted unchanged in the urine and therefore has fewer drug interactions. If opioids are a consideration for neuropathic pain relief, the lowest dose is recommended. Topical therapies for neuropathic pain have the advantage of controlling pain without systemic side effects. It therefore can be combined with systemic treatment. Lidocaine 5% patches (LIDODERM®) block neuronal sodium channels whereas Capsaicin cream (ZOSTRIX®) stimulates the C fibers to release and subsequently deplete substance P, there by blocking pain signaling to the brain. Diclofenac gel 1% when applied once a day, concentrates in the dermis and has less gastrointestinal side effects and may be beneficial for neuropathic pain. A combination of Ketamine 1% and Amitriptyline 2% cream applied topically has also been promising in a small study. Patients experiencing refractory pain may benefit with the use of Transcutaneous Electrical Nerve Stimulation (TENS), although referral to the pain clinic may be appropriate. Psychosocial support utilizing a team of specialists and social workers/counsellors, should be an integral part of pain management. Kvale E and Urba SG. National Comprehensive Cancer Network (NCCN) 19th Annual Conference, March 13 – 15, 2014; Hollywood, Florida
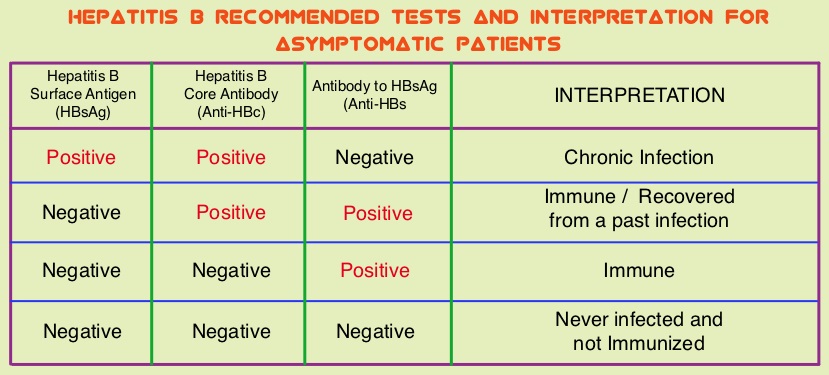 The CDC updated their recommendations in 2008 and recommended HBV screening for patients receiving cytotoxic chemotherapy or immunotherapy. The American Society of Clinical Oncology in 2010 rendered a Provisional Clinical Opinion (PCO) suggesting that there was insufficient evidence to recommend routine screening for HBV in cancer patients,but screening may be considered for patient populations at high risk or for those who are to receive highly immunosuppressive therapies including anti-CD20 monoclonal antibody therapy such as Rituximab (RITUXAN®). To evaluate compliance with these recommendations, the authors in this study retrospectively reviewed charts of patients with Low grade Non Hodgkins Lymphoma at a teritiary care center and documented the various studies performed, as a part of the pretreatment workup, between January 2005 and December 2011. They noted that only 19% of the total patients and 25% of the patients who received RITUXAN® had HBV screening done. The authors concluded that this was a significant deviation from the recommended guidelines and these findings resulted in the implementation of stricter measures for HBV screening at this teritiary care center. Screening for HBV should include testing for Hepatitis B surface antigen (HBsAg), Antibody to Hepatitis B core antigen (anti-HBc) and Antibody to Hepatitis B surface antigen (Anti-HBs). Patients positive for HBsAg and anti-HBc as well as those who are negative for HBsAg and positive for anti-HBc, should have testing for HBV viral load using serum HBV DNA and those without active disease should receive prophylactic antiviral therapy and be closely monitored for HBV reactivation. Prophylaxis is usually started one week before initiating chemotherapy and continued for at least 6 months after completion of chemotherapy, although the actual duration of prophylactic antiviral therapy remains unclear. If HBV reactivation is noted, chemotherapy should be immediately discontinued. Given the prevalence of chronic Hepatitis B in the United States, screening for HBV should become a routine part of pretreatment evaluation in cancer patients. Abbi KK, Gorris M, Skeel RT. Am J Ther. 2013;June 28.
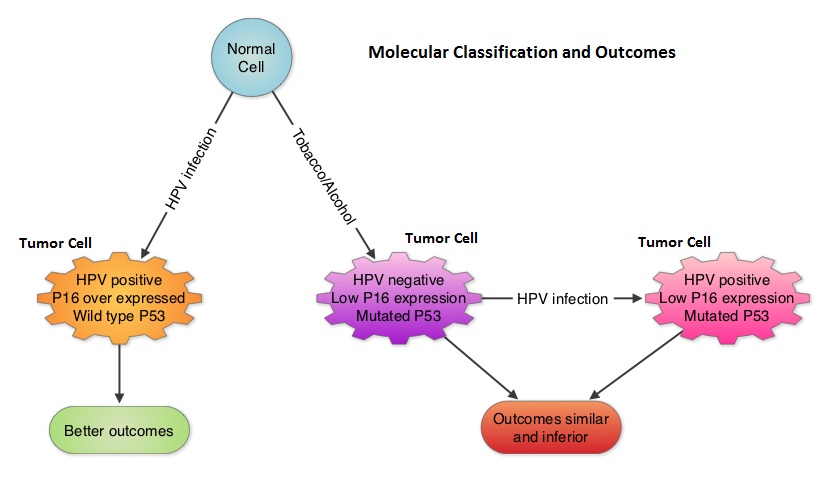
The CDC updated their recommendations in 2008 and recommended HBV screening for patients receiving cytotoxic chemotherapy or immunotherapy. The American Society of Clinical Oncology in 2010 rendered a Provisional Clinical Opinion (PCO) suggesting that there was insufficient evidence to recommend routine screening for HBV in cancer patients,but screening may be considered for patient populations at high risk or for those who are to receive highly immunosuppressive therapies including anti-CD20 monoclonal antibody therapy such as Rituximab (RITUXAN®). To evaluate compliance with these recommendations, the authors in this study retrospectively reviewed charts of patients with Low grade Non Hodgkins Lymphoma at a teritiary care center and documented the various studies performed, as a part of the pretreatment workup, between January 2005 and December 2011. They noted that only 19% of the total patients and 25% of the patients who received RITUXAN® had HBV screening done. The authors concluded that this was a significant deviation from the recommended guidelines and these findings resulted in the implementation of stricter measures for HBV screening at this teritiary care center. Screening for HBV should include testing for Hepatitis B surface antigen (HBsAg), Antibody to Hepatitis B core antigen (anti-HBc) and Antibody to Hepatitis B surface antigen (Anti-HBs). Patients positive for HBsAg and anti-HBc as well as those who are negative for HBsAg and positive for anti-HBc, should have testing for HBV viral load using serum HBV DNA and those without active disease should receive prophylactic antiviral therapy and be closely monitored for HBV reactivation. Prophylaxis is usually started one week before initiating chemotherapy and continued for at least 6 months after completion of chemotherapy, although the actual duration of prophylactic antiviral therapy remains unclear. If HBV reactivation is noted, chemotherapy should be immediately discontinued. Given the prevalence of chronic Hepatitis B in the United States, screening for HBV should become a routine part of pretreatment evaluation in cancer patients. Abbi KK, Gorris M, Skeel RT. Am J Ther. 2013;June 28.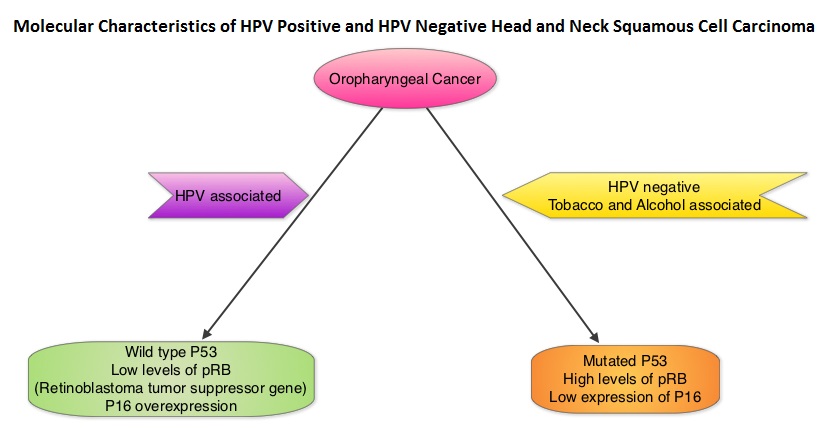 Chronic immunosuppression as seen in patients with HIV and in patients undergoing solid organ transplantation, may increase the risk for HPV infections. Patients with HPV associated oropharyngeal cancer typically are younger males, tend not to smoke or drink and present with poorly differentiated, non keratinizing tumors with basaloid morphology, compared to those with HPV negative tumors. Clinical characteristics of HPV positive oropharyngeal cancer patients with best outcomes include, those with fewer than 10 pack year smoking history and lower tumor stage. Several retrospective trials as well as some small prospective studies have shown that HPV positive oropharygeal cancers when treated with chemoradiation have significantly higher response rates, progression free survival, overall survival and better local and regional disease control. In the TAX 324 randomized phase III trial, patients received induction treatment with 3 cycles of TAXOTERE®, Cisplatin and 5-Fluorouracil (5-FU) or Cisplatin and 5-FU followed by chemoradiation with concurrent PARAPLATIN® (Carboplatin). Even though the 3 drug induction treatment group had superior outcomes compared to those who received 2 drug induction regimen in the intent to treat population, on retrospective analysis, patients with HPV positive oropharyngeal cancer had a significantly longer 5 year progression free survival (78% vs 28%) and overall survival, with an 80% reduction in mortality (HR=0.20, P<0.0001), compared to HPV negative patients, regardless of induction treatment. Other studies have shown that HPV positive patients who undergo surgery alone for oropharyngeal cancer do not appear to reap these favorable benefits, suggesting that the improved prognosis in the HPV positive patients with oropharyngeal cancer is related to chemotherapy and radiation. It also appears that HPV positive patients with oropharyngeal cancer have a better prognosis with treatment when their tumors are P53 wild type and express P16. With regards to EGFR and P16, there appears to be an inverse correlation between P16 and EGFR expression and patients with tumors expressing P16 and not EGFR have a significantly higher 5 year disease free and overall survival compared to those whose tumors overexpress EGFR but not P16. This information may have significant therapeutic implications and studies are underway trying to address this group of patients with targeted and less intense treatments. It should be noted that HPV positive status has a favorable prognostic value only for oropharyngeal primary cancers and not for other cancers of the head and neck.
Chronic immunosuppression as seen in patients with HIV and in patients undergoing solid organ transplantation, may increase the risk for HPV infections. Patients with HPV associated oropharyngeal cancer typically are younger males, tend not to smoke or drink and present with poorly differentiated, non keratinizing tumors with basaloid morphology, compared to those with HPV negative tumors. Clinical characteristics of HPV positive oropharyngeal cancer patients with best outcomes include, those with fewer than 10 pack year smoking history and lower tumor stage. Several retrospective trials as well as some small prospective studies have shown that HPV positive oropharygeal cancers when treated with chemoradiation have significantly higher response rates, progression free survival, overall survival and better local and regional disease control. In the TAX 324 randomized phase III trial, patients received induction treatment with 3 cycles of TAXOTERE®, Cisplatin and 5-Fluorouracil (5-FU) or Cisplatin and 5-FU followed by chemoradiation with concurrent PARAPLATIN® (Carboplatin). Even though the 3 drug induction treatment group had superior outcomes compared to those who received 2 drug induction regimen in the intent to treat population, on retrospective analysis, patients with HPV positive oropharyngeal cancer had a significantly longer 5 year progression free survival (78% vs 28%) and overall survival, with an 80% reduction in mortality (HR=0.20, P<0.0001), compared to HPV negative patients, regardless of induction treatment. Other studies have shown that HPV positive patients who undergo surgery alone for oropharyngeal cancer do not appear to reap these favorable benefits, suggesting that the improved prognosis in the HPV positive patients with oropharyngeal cancer is related to chemotherapy and radiation. It also appears that HPV positive patients with oropharyngeal cancer have a better prognosis with treatment when their tumors are P53 wild type and express P16. With regards to EGFR and P16, there appears to be an inverse correlation between P16 and EGFR expression and patients with tumors expressing P16 and not EGFR have a significantly higher 5 year disease free and overall survival compared to those whose tumors overexpress EGFR but not P16. This information may have significant therapeutic implications and studies are underway trying to address this group of patients with targeted and less intense treatments. It should be noted that HPV positive status has a favorable prognostic value only for oropharyngeal primary cancers and not for other cancers of the head and neck.