
The FDA on February 15, 2019 approved KEYTRUDA® for the adjuvant treatment of patients with Melanoma with involvement of lymph node(s) following complete resection. KEYTRUDA® is a product of Merck & Co., Inc.
Tag: Malignant Melanoma of the Skin
Immunotherapy Effective for Melanoma Metastatic to the Brain
SUMMARY: It is estimated that in the US, approximately 91,270 new cases of melanoma will be diagnosed in 2018 and about 9,320 patients are expected to die of the disease. The incidence of melanoma has been on the rise for the past three decades. Brain metastases are a frequent complication of solid tumors and these patients tend to have a very poor prognosis with a median survival of a few weeks to months. Malignant melanoma has the highest propensity to metastasize to the brain. More than one third of patients with advanced melanoma have brain metastases at the time of diagnosis, and up to 75% of patients have brain metastases at the time of death. Prognosis of patients with melanoma who have brain metastases is poor, with a median Overall Survival of 4-5 months and a 5 year survival of 5%. This is because systemic chemotherapy has minimal antitumor activity in the brain, does not decrease the risk of development of new brain metastases, does not control of extracranial disease and does not improve Overall Survival.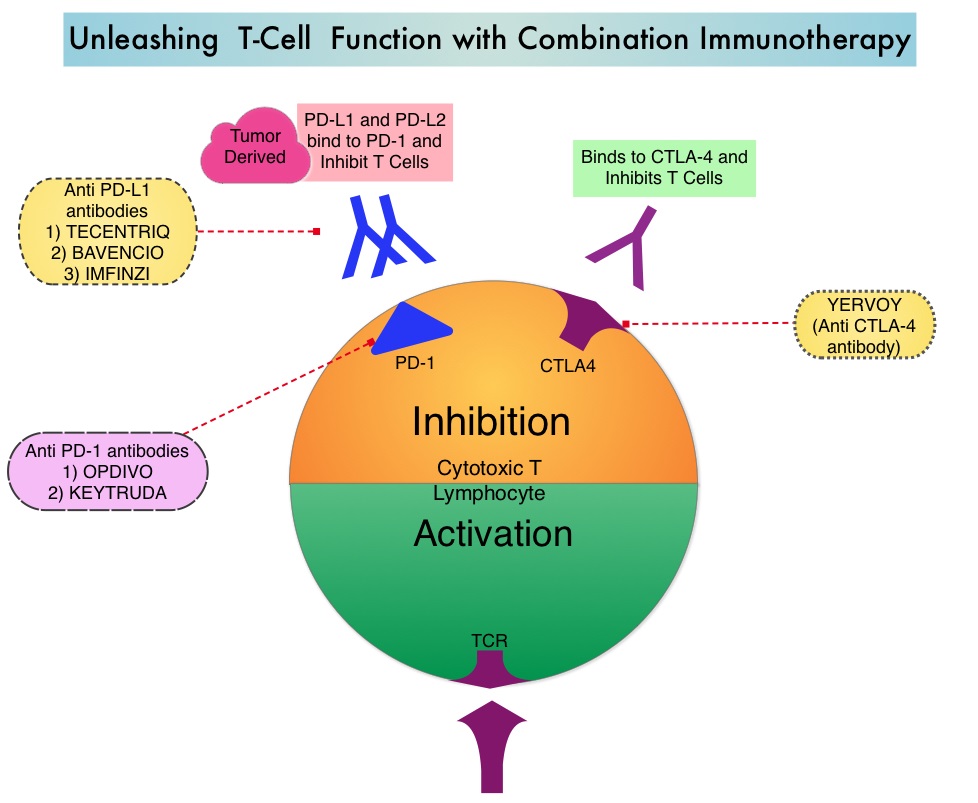
Immune checkpoint inhibitors by blocking immune checkpoint proteins unleash T cells, resulting in T cell proliferation, activation and a therapeutic response. YERVOY® (Ipilimumab) is a fully human immunoglobulin G1 monoclonal antibody that blocks immune checkpoint protein/receptor CTLA-4, and has been shown to have activity against brain metastases from melanoma when used individually as monotherapy. OPDIVO® (Nivolumab) is a fully human, Immunoglobulin G4, anti PD-1 targeted monoclonal antibody. It binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, following which the tumor-specific effector T cells are unleashed. OPDIVO® when combined with YERVOY® significantly improved Overall Survival in patients with previously untreated advanced melanoma, compared with YERVOY® alone, in phase II and III studies. These studies however excluded patients with untreated brain metastases.
CheckMate 204 is an open-label, multicenter, phase II study, conducted at 28 sites in the United States and the authors in this study evaluated the efficacy and safety of OPDIVO® plus YERVOY® in patients with melanoma who had untreated brain metastases. This study enrolled 101 patients with metastatic melanoma and at least one measurable, nonirradiated brain metastasis (tumor diameter 0.5-3 cm) and no neurologic symptoms. Patients received OPDIVO® 1 mg/kg plus YERVOY® 3 mg/kg every 3 weeks for up to four doses, followed by OPDIVO® 3 mg/kg every 2 weeks until progression or unacceptable toxic effects. The median age was 59 years, 44% of patients had PD-L1 expression of 1% or more, 22% of the patients had 3 or more target lesions and 17% had received previous systemic anticancer therapy, with BRAF inhibitor being the most common (11%), a MEK inhibitor (9%), or both. Patients with known leptomeningeal involvement, those with metastases larger than 3 cm in diameter, and those patients receiving glucocorticoid therapy, were excluded from the study. The Primary end point was the rate of intracranial clinical benefit, defined as the percentage of patients who had stable disease for at least 6 months, Complete Response, or Partial Response. Of the 101 patients enrolled, 94 patients had a minimum follow up of 6 months (median follow up 14.0 months), and could be evaluated for the Primary end point.
With a median follow up of 14 months, the rate of intracranial clinical benefit was 57%, with a Complete Response rate of 26%, Partial Response rate of 30%, and 2% of the patients had stable disease for at least 6 months. Similar rates of Objective Response Rate (50%) and Clinical Benefit (56%) were observed for extracranial lesions. The median time to intracranial response was 2.3 months. The safety profile of the regimen was similar to that reported in patients with melanoma who did not have brain metastases, and treatment-related grade 3/ 4 Adverse Events were reported in 55% of patients.
It was concluded that OPDIVO® combined with YERVOY® is an effective treatment for metastatic melanoma patients with asymptomatic, untreated brain metastases. In this study, patients had clinically meaningful intracranial efficacy, concordant with extracranial activity. The safety profile in this population was similar to that reported in studies involving patients without brain metastases. This regimen should be considered as first-line therapy for all eligible metastatic melanoma patients, with brain metastases. Combined Nivolumab and Ipilimumab in Melanoma Metastatic to the Brain. Tawbi HA, Forsyth PA, Algazi A, et al. N Engl J Med 2018; 379:789-790
BRAFTOVI® (Encorafenib) and MEKTOVI® (Binimetinib)
The FDA on June 27, 2018 approved BRAFTOVI® and MEKTOVI® in combination for patients with unresectable or metastatic melanoma with a BRAF V600E or V600K mutation, as detected by an FDA-approved test. BRAFTOVI® and MEKTOVI® are products of Array BioPharma Inc.
FDA Approves Adjuvant TAFINLAR® plus MEKINIST® for Stage III BRAF-Mutated Melanoma
SUMMARY: The FDA on April 30, 2018, granted regular approval to TAFINLAR® (Dabrafenib) and MEKINIST® (Trametinib), in combination, for the adjuvant treatment of patients with melanoma with BRAF V600E or V600K mutations, as detected by an FDA-approved test, and involvement of lymph node(s), following complete resection. It is estimated that in the US, approximately 91,270 new cases of melanoma will be diagnosed in 2018 and about 9,320 patients are expected to die of the disease. The incidence of melanoma has been on the rise for the past three decades. Surgical resection with a curative intent is the standard of care for patients with early stage melanoma, with a 5-year survival rate of 98% for stage I disease and 90% for stage II disease. Stage III malignant melanoma however is a heterogeneous disease, and the risk of recurrence is dependent on the number of positive nodes, as well as presence of palpable versus microscopic nodal disease. Further, patients with a metastatic focus of more than 1 mm in greatest dimension in the affected lymph node, have a significantly higher risk of recurrence or death than those with a metastasis of 1 mm or less. Patients with stage IIIA disease have a disease-specific survival rate of 78% whereas those patients with stage IIIB and stage IIIC disease have disease-specific survival rates of 59% and 40% respectively.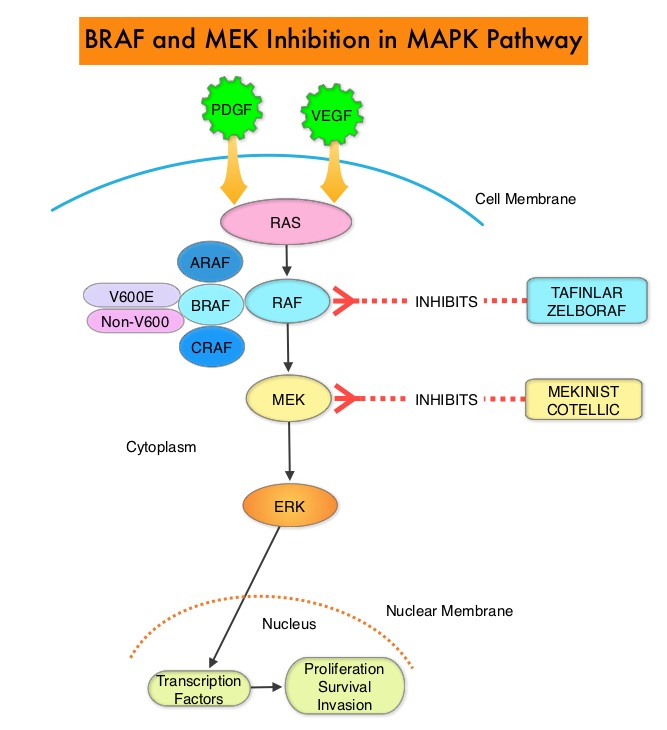
The Mitogen-Activated Protein Kinase pathway (MAPK pathway) is an important signaling pathway which enables the cell to respond to external stimuli. This pathway plays a dual role, regulating cytokine production and participating in cytokine dependent signaling cascade. The MAPK pathway of interest is the RAS-RAF-MEK-ERK pathway. The RAF family of kinases includes ARAF, BRAF and CRAF signaling molecules. BRAF is a very important intermediary of the RAS-RAF-MEK-ERK pathway. BRAF mutations have been demonstrated in 6-8% of all malignancies. The most common BRAF mutation in melanoma is at the V600E/K site and is detected in approximately 50% of melanomas and result in constitutive activation of the MAPK pathway.
TAFINLAR®,is a selective oral BRAF inhibitor and MEKINIST® is a potent and selective inhibitor of MEK gene, which is downstream from RAF in the MAPK pathway. In patients with BRAF V600 mutation-positive unresectable or metastatic melanoma, a combination of TAFINLAR® and MEKINIST® resulted in a median Overall Survival (OS) of more than 2 years, with approximately 20% of the patients remaining progression free at 3 years. These encouraging results led to the study of this combination in patients with stage III melanoma, with BRAFV600E or V600K mutations, after complete surgical resection.
This FDA approval was based on COMBI-AD, an international, multi-center, randomized, double-blind, placebo-controlled, phase III trial, in which 870 patients with completely resected, stage III melanoma and with BRAF V600E or V600K mutations were enrolled. Patients were randomly assigned in a 1:1 to receive TAFINLAR® 150 mg orally twice daily in combination with MEKINIST® 2 mg orally once daily (N=438) or two matched placebos (N=432). Treatment was given for 12 months. Eligible patients had undergone completion lymphadenectomy, with no clinical or radiographic evidence of residual regional node disease. None of the patients had received previous systemic anticancer treatment or radiotherapy for melanoma. BRAF V600 mutation status was confirmed in primary tumor tissue or lymph node tissue by a central reference laboratory. The median age was 50 years. Both treatment groups were well balanced and 18% had stage IIIA disease, 41% had stage IIIB disease, and 40% had stage IIIC disease. Of the enrolled patients, 91% had a BRAF V600E mutation, and 9% had a BRAF V600K mutation. The Primary end point was Relapse Free Survival (RFS) and Secondary end points included Overall Survival (OS), Distant metastasis-free survival, Freedom from relapse, and Safety.
At a median follow up of 2.8 years, the estimated 3-year RFS rate was 58% in the combination therapy group and 39% in the placebo group (HR=0.47; P<0.001), and this represented a 53% lower risk of relapse. At the time of this analysis, median RFS rate had not yet been reached in the combination therapy group and was 16.6 months in the placebo group. The improved RFS benefit with the combination therapy was consistent across patient subgroups, regardless of lymph node involvement or primary tumor ulceration. The risk of distant metastases or death was reduced by 49% with the combination therapy versus placebo (HR=0.51; P<0.001). The safety profile of TAFINLAR® plus MEKINIST® was consistent with that observed with the combination, in patients with metastatic melanoma, and the common side effects were pyrexia, fatigue, nausea, vomiting, diarrhea, headache, rash, arthralgia, and myalgia.
It was concluded that adjuvant combination therapy with TAFINLAR® plus MEKINIST® in patients with stage III melanoma with BRAF V600E or V600K mutations, resulted in a significantly lower risk of recurrence, compared to placebo, with no new adverse events. With more than half the patients with stage III melanoma having a recurrence after surgery, this first effective oral targeted combination therapy, will be an important adjuvant treatment option. Adjuvant Dabrafenib plus Trametinib in Stage III BRAF-Mutated Melanoma. Long GV, Hauschild A, Santinami M, et al. N Engl J Med 2017; 377:1813-1823
TAFINLAR® and MEKINIST®
The FDA on April 30, 2018 granted regular approval to TAFINLAR® (Dabrafenib) and MEKINIST® (Trametinib), in combination, for the adjuvant treatment of patients with Melanoma with BRAF V600E or V600K mutations, as detected by an FDA-approved test, and involvement of lymph node(s), following complete resection. TAFINLAR® and MEKINIST® are products of Novartis Pharmaceuticals Corp.
FDA Approves OPDIVO® for Adjuvant Treatment of Malignant Melanoma
The FDA on December 20, 2017, granted regular approval to the anti-PD1 monoclonal antibody, OPDIVO® (Nivolumab) for the adjuvant treatment of patients with melanoma with involvement of lymph nodes or in patients with metastatic disease who have undergone complete resection. The approved adjuvant therapies over the past two decades, for patients with high-risk melanoma have included high-dose INTRON® A (Interferon alfa-2b), SYLATRON® (peginterferon alfa-2b), and high-dose YERVOY® (Ipilimumab). The significant toxicities associated with these adjuvant interventions, precluded the wide spread use of adjuvant therapy in high risk melanoma.
OPDIVO® is a less toxic, better tolerated, adjuvant treatment option than YERVOY®, for patients with resected stage IIIB/C and IV melanoma, regardless of BRAF mutation. The Recurrence Free Survival rate at 18 months with OPDIVO® was 66.4% compared with 52.7% for YERVOY® and this meant a 35% reduction in the risk of recurrence or death with the OPDIVO® versus YERVOY®. This will fulfill the unmet need for adjuvant therapies, with improved benefit-risk ratio, for this patient group.
Late Breaking Abstract – ESMO 2017 FDA Approves OPDIVO® for Adjuvant Treatment of Malignant Melanoma
SUMMARY: The FDA on December 20, 2017, granted regular approval to the anti-PD1 monoclonal antibody, OPDIVO® (Nivolumab) for the adjuvant treatment of patients with melanoma with involvement of lymph nodes or in patients with metastatic disease who have undergone complete resection. OPDIVO® was previously approved for the treatment of patients with unresectable or metastatic melanoma. It is estimated that in the US, approximately 91,270 new cases of melanoma will be diagnosed in 2018 and about 9,320 patients are expected to die of the disease. The incidence of melanoma has been on the rise for the past three decades. Stage III malignant melanoma is a heterogeneous disease and the risk of recurrence is dependent on the number of positive nodes as well as presence of palpable versus microscopic nodal disease. Further, patients with a metastatic focus of more than 1 mm in greatest dimension in the affected lymph node, have a significantly higher risk of recurrence or death than those with a metastasis of 1 mm or less. Patients with stage IIIA disease have a disease-specific survival rate of 78%, whereas those with stage IIIB and stage IIIC disease have a disease specific survival rates of 59% and 40% respectively.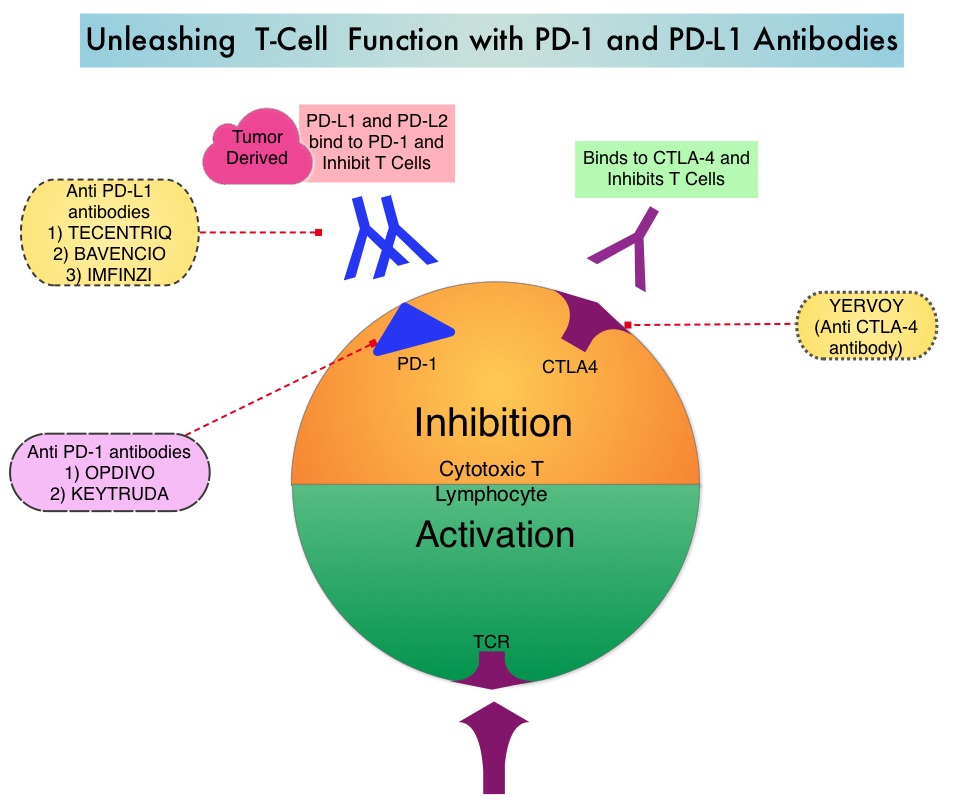
Immune checkpoints are cell surface inhibitory proteins/receptors that harness the immune system and prevent uncontrolled immune reactions. Immune checkpoint proteins (“gate keepers”) suppress antitumor immunity. Antibodies targeting these, membrane bound, inhibitory, Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc., block the Immune checkpoint proteins and unleash T cells, resulting in T cell proliferation, activation and a therapeutic response.
The approved adjuvant therapies over the past two decades, for patients with high-risk melanoma have included high-dose INTRON® A (Interferon alfa-2b), SYLATRON® (peginterferon alfa-2b), and high-dose YERVOY® (Ipilimumab). The significant toxicities associated with these adjuvant interventions, precluded the wide spread use of adjuvant therapy in high risk melanoma. YERVOY® was approved by the FDA for the adjuvant treatment of patients with completely resected, Stage III melanoma, based on an improvement in Relapse Free Survival, when compared to placebo, in a randomized phase III trial. In this study however, over 50% of the patients treated with the recommended high dose YERVOY® experienced grade 3/4 toxicities. There is therefore an unmet need for adjuvant therapies, with improved benefit-risk ratio, for this patient group.
OPDIVO® (Nivolumab) is a fully human, immunoglobulin G4 monoclonal antibody that targets PD-1 receptor. Monotherapy with OPDIVO®, in heavily pretreated advanced Melanoma patients can result in more than a third of patients (34%) being alive, 5 years after starting treatment. The present approval by the FDA was based on CheckMate 238 trial, which is a double-blind, phase III study that included 906 patients with completely resected, Stage IIIB/C or Stage IV melanoma. Patients were randomized in a 1:1 ratio to receive either OPDIVO® 3 mg/kg IV, every 2 weeks (N=453) or YERVOY® 10 mg/kg IV, every 3 weeks (N=453) for 4 doses, then every 12 weeks beginning at week 24, for up to 1 year. Both treatment groups were well balanced. The Primary end point was Recurrence Free Survival (RFS).
The Recurrence Free Survival rate at 18 months with OPDIVO® was 66.4% compared with 52.7% for YERVOY® (HR=0.65; P<0.0001). This meant a 35% reduction in the risk of recurrence or death with the OPDIVO® versus YERVOY®. The most common adverse reactions were headache, fatigue, nausea, diarrhea, abdominal discomfort, rash, pruritus and musculoskeletal pain. OPDIVO® was associated with significantly fewer treatment-related grade 3/4 toxicities compared to YERVOY® (14% versus 46%). Treatment was discontinued due to toxicities in approximately 10% of the patients in the OPDIVO® group, compared with 42% of patients in the YERVOY® group.
The authors concluded that OPDIVO® is a less toxic, better tolerated, adjuvant treatment option than YERVOY®, for patients with resected stage IIIB/C and IV melanoma, regardless of BRAF mutation, with a superior Relapse Free Survival rate. Weber J, Mandala M, Del Vecchio M, et al. Adjuvant therapy with nivolumab (NIVO) versus ipilimumab (IPI) after complete resection of stage III/IV melanoma: a randomized, double-blind, phase 3 trial (CheckMate 238). Presented at ESMO 2017 Congress; September 8-12, 2017; Madrid, Spain. Abstract LBA8_PR.
OPDIVO® (Nivolumab)
The FDA on December 20, 2017 granted regular approval to the anti-PD1 monoclonal antibody OPDIVO® for the adjuvant treatment of patients with melanoma with involvement of lymph nodes or in patients with metastatic disease who have undergone complete resection. OPDIVO® was previously approved for the treatment of patients with unresectable or metastatic melanoma. OPDIVO® is a product of Bristol-Myers Squibb Company.
OPDIVO® and YERVOY® Combination Improves Overall Survival in Advanced Melanoma
SUMMARY: It is estimated that in the US, about 87,110 new cases of melanoma will be diagnosed in 2017 and about 9,730 patients will die of the disease. The incidence of melanoma has been on the rise for the past three decades. A better understanding of Immune checkpoints has opened the doors for the discovery of novel immune targets. Immune checkpoints are cell surface inhibitory proteins/receptors that harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies have been developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By blocking the Immune checkpoint proteins, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response.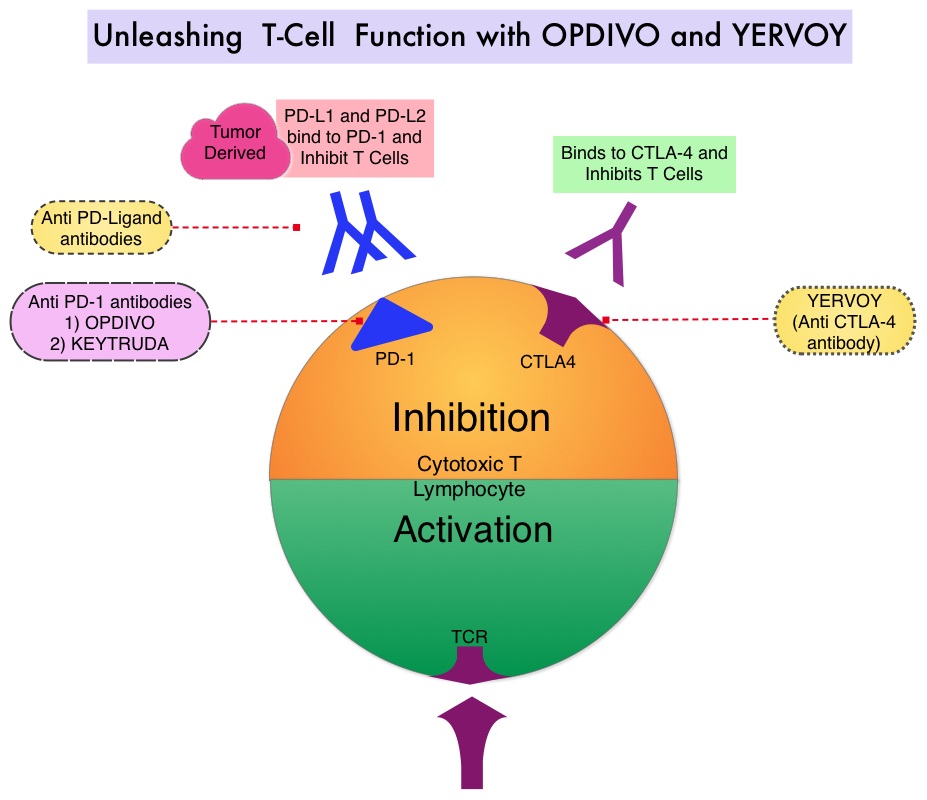
YERVOY® (Ipilimumab) is a fully human immunoglobulin G1 monoclonal antibody that blocks Immune checkpoint protein/receptor CTLA-4, and was the first systemic therapy to show prolonged Overall Survival (OS) among patients with advanced melanoma, in randomized phase III trials. YERVOY® in a pooled analysis of data from 12 studies showed a 3-year Overall Survival of 26% among treatment naive patients and survival up to 10 years in approximately 20% of all patients, with advanced melanoma. The two PD-1 inhibitors of interest are OPDIVO® (Nivolumab) and KEYTRUDA® (Pembrolizumab), which are fully human, Immunoglobulin G4, anti-PD-1 targeted monoclonal antibodies, which bind to the PD-1 receptor and block its interaction with ligands PD-L1 and PD-L2, following which the tumor-specific effector T cells are unleashed. They are thus able to undo PD-1 pathway-mediated inhibition of the immune response. When compared with YERVOY®, in patients with advanced melanoma, PD-1 inhibitors, both OPDIVO® and KEYTRUDA®, have demonstrated superior Overall Survival (OS), Progression Free Survival (PFS), and Objective Response Rate (ORR), with a better safety profile. OPDIVO® in combination with YERVOY® in a phase I study resulted in an Overall Survival of 68% at 3 years among patients with advanced melanoma, regardless of prior therapies.
CheckMate 067 is a phase III study which enrolled treatment naïve patients with advanced melanoma, and the authors in a previous publication reported significantly longer PFS and higher rates of ORR with OPDIVO® plus YERVOY® and with OPDIVO® alone, compared with single agent YERVOY®. In this publication, the authors provided the first analysis of 3-year OS data from the CheckMate 067 trial. In this double-blind, phase III study, patients with previously untreated advanced melanoma were randomly assigned in a 1:1:1 ratio to receive one of the three regimens: OPDIVO® 1 mg/kg every 3 weeks plus YERVOY® 3 mg/kg every 3 weeks for four doses, followed by OPDIVO® 3 mg/kg every 2 weeks (N=314); OPDIVO® 3 mg/kg every 2 weeks plus placebo (N=316); or YERVOY® 3 mg/kg every 3 weeks for four doses plus placebo (N=315). Randomization was stratified according to BRAF mutation status, metastasis stage, and Programmed cell Death Ligand 1 (PD-L1) status. Treatment was continued until disease progression or unacceptable toxicities. The two primary end points were PFS and OS in the OPDIVO® plus YERVOY® group and in the OPDIVO® group versus the YERVOY® group.
The median OS at a minimum follow up of 36 months, had not been reached in the OPDIVO® plus YERVOY® group and was 37.6 months in the OPDIVO® group, compared with 19.9 months in the YERVOY® group (Hazard Ratio for death with OPDIVO® plus YERVOY® versus YERVOY®=0.55 (P<0.001); Hazard Ratio for death with OPDIVO® versus YERVOY®=0.65 (P<0.001). The OS at 3 years in the OPDIVO® plus YERVOY® group was 58% and in the OPDIVO® group was 52%, as compared with 34% in the YERVOY® group. Grade 3 or 4 treatment-related toxicities, as expected were higher in the OPDIVO® plus YERVOY® group at 59% compared with 21% in the OPDIVO® group, and 28% in the YERVOY® group.
It was concluded that in patients with previously untreated advanced melanoma, significantly longer Overall Survival can be achieved with OPDIVO® plus YERVOY® combination therapy or with OPDIVO® alone, compared with single agent YERVOY®. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. Wolchok JD, Chiarion-Sileni V, Gonzalez R, et al. N Engl J Med 2017; 377:1345-1356
Restricting Indoor Tanning Can Impact Melanoma Incidence and Treatment Costs
SUMMARY: It is estimated that in the US, about 87,110 new cases of melanoma will be diagnosed in 2017 and about 9,730 patients will die of the disease. The incidence of melanoma has been on the rise for the past three decades. A major risk factor for most skin cancers is exposure to UltraViolet (UV) radiation, which damages the DNA of skin cells. The main source of UV rays is sunlight, tanning lamps and tanning beds. UV exposure also can cause cataracts and ocular melanoma. Indoor tanning, exposes individuals to both UVA and UVB rays and is particularly dangerous for those who begin indoor tanning during adolescence or early adulthood, putting them at a higher risk of developing melanoma. The association between indoor tanning beds, including those with the newer tanning technology, and melanoma, has been well established with a 22-34% increase in the risk of developing melanoma with indoor tanning. The International Agency for Research on Cancer has classified indoor tanning as a Class I carcinogen, based on its significant association with malignant melanoma. Indoor tanning with resulting exposure to ultraviolet radiation is a potentially modifiable behavior. According to the 2015 Youth Risk Behavior Surveillance System, approximately 15% of the high school teens are indoor tanning and according to the 2010 National Health Interview Survey, indoor tanners tended to be young, non-Hispanic white women of whom 32% are aged 18 to 21 years.
The authors in this study estimated the health and economic benefits of reducing indoor tanning in the United States. Using a statistical model that takes into consideration risk, that continues over time (Markov model), the authors estimated the number of melanoma cases and deaths that could be prevented and melanoma treatment costs saved, by reducing indoor tanning among minors younger than 18 years. These estimations were based on a cohort of 61.2 million individuals aged 14 years or younger in the United States and the probability of these individuals using indoor tanning, based on data from the 2013 Youth Risk Behavior Survey. The prevalence of indoor tanning was based on a recent meta-analysis.
The researchers noted that restricting the use of indoor tanning among minors younger than 18 years was estimated to prevent 61,839 cases of melanoma (4.9% reduction) and 6,735 melanoma deaths (4.7% reduction), over the lifetime of this group of individuals. The treatment cost-savings from these reductions was estimated to be $342.9 million over the lifetime of these individuals. These health and economic benefits increased as indoor tanning was further reduced.
The authors concluded that reducing indoor tanning has the potential to reduce melanoma incidence, mortality, and treatment costs, emphasizing the importance of continued public health efforts to identify and implement effective strategies to prevent melanoma. The potential impact of reducing indoor tanning on melanoma prevention and treatment costs in the United States: An economic analysis. Guy GP, Zhang Y, Ekwueme DU, et al. Journal of the American Academy of Dermatology 2017;76:226-233