
SUMMARY: The FDA on October 27, 2015 approved IMLYGIC® (Talimogene laherparepvec or T-VEC), the first FDA-approved oncolytic virus therapy, for the treatment of melanoma lesions in the skin and lymph nodes. The American Cancer Society’s estimates that for 2015, approximately 74,000 new melanomas will be diagnosed in the United States and about 10,000 people are expected to die of the disease. IMLYGIC® is a genetically modified, herpes simplex virus type 1–derived oncolytic immunotherapy designed to induce both local and systemic immune responses. Following injection directly into melanoma lesions, IMLYGIC® selectively replicates within tumors and produces an immunostimulatory protein called Granulocyte-Macrophage Colony Stimulating Factor (GM-CSF). IMLYGIC® causes cell lysis resulting in the release of tumor-derived antigens, which along with the local GM-CSF, recruit and activate antigen-presenting cells, with subsequent induction of tumor-specific T-cell responses. The enhanced systemic antitumor immune response against tumor-derived antigens, eradicates tumor cells elsewhere in the body.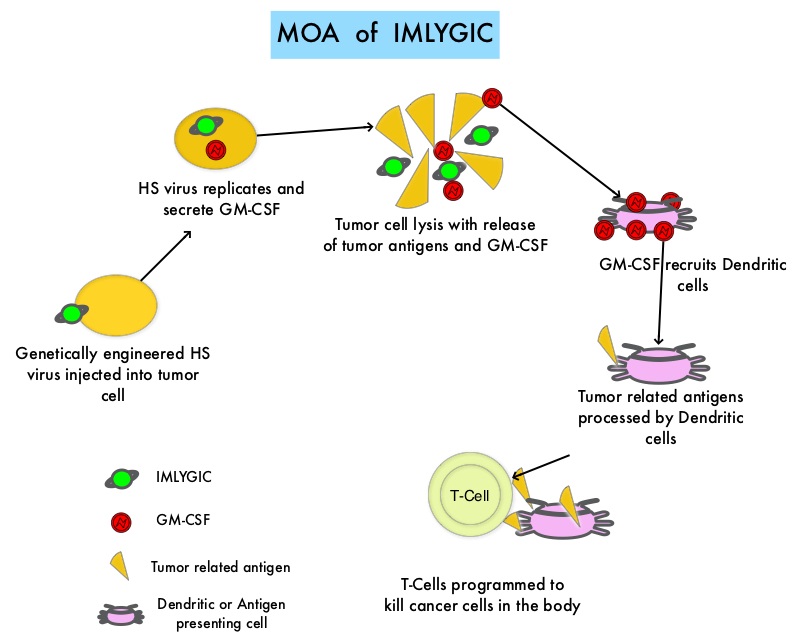
Previously reported single arm phase II study with IMLYGIC® demonstrated an Overall Response Rate (ORR) of 26% in patients with stage IIIC to IV melanoma, with responses noted in both injected and un-injected lesions, including visceral lesions. Oncovex (GM-CSF) Pivotal Trial in Melanoma (OPTiM) is a phase III study in which 436 patients with stage IIIB to IV melanoma, with injectable melanoma lesions that could not be surgically resected, were randomly assigned in a 2:1 ratio to receive intralesional IMLYGIC® (N=295) or subcutaneous GM-CSF (N=141). The enrolled patient’s melanoma lesions in the skin and lymph nodes were treated with IMLYGIC® or a comparator therapy and Injection into visceral lesions was not allowed. Patients in the IMLYGIC® group received a series of injections into the melanoma lesions. Following the initial injection, a second dose was administered three weeks later, followed by additional doses every two weeks for at least six months, unless other treatment was required or until there are were no remaining injectable lesions to treat. Patients in the GM-CSF group received 125 micrograms/m2 subcutaneously once daily for 14 days in 28-day cycles. The median age of patients in the study was 63 years. The primary end point was Durable Response Rate (DRR- Objective Response lasting continuously for 6 months or more). Secondary end points included Overall Survival (OS) and Overall Response Rate.
The DRR was significantly higher among patients receiving IMLYGIC® than among those given GM-CSF (16.3% vs 2.1%; P<0.001). The Overall Response Rate was also higher with IMLYGIC® compared to GM-CSF (26.4% vs 5.7%; P<0.001). Approximately 11% of patients receiving IMLYGIC® experienced a Complete Response compared to less than 1% for those receiving GM-CSF. The median Time to Treatment Failure was 8.2 months with IMLYGIC® and 2.9 months with GM-CSF (HR=0.42) and median Overall Survival was 23.3 months and 18.9 months, respectively (HR=0.79; P=0.051). In an exploratory subset analysis, the benefit with IMLYGIC® was more pronounced among patients with stage IIIB, IIIC, or IV M1a disease, as well as among patients who were treatment naïve. The most common side effects were fatigue, chills, fever, nausea, flu-like symptoms and pain at the injection site. IMLYGIC® should not be given to individuals with suppressed immune systems or who are pregnant because IMLYGIC® is a modified live oncolytic herpes virus therapy and herpes virus infection can potentially occur.
The authors concluded that IMLYGIC® is the first oncolytic immunotherapy to demonstrate therapeutic benefit in patients with advanced unresectable melanoma and may be another novel therapeutic option for patients with metastatic melanoma. Combining IMLYGIC® with T-Cell checkpoint inhibitor, YERVOY® (Ipilimumab) is presently being explored and thus far has shown encouraging results with minimal added toxicities. Talimogene Laherparepvec Improves Durable Response Rate in Patients With Advanced Melanoma. Andtbacka RH, Kaufman HL, Collichio F, et al. Published online before print May 26, 2015, doi: 10.1200/JCO.2014.58.3377
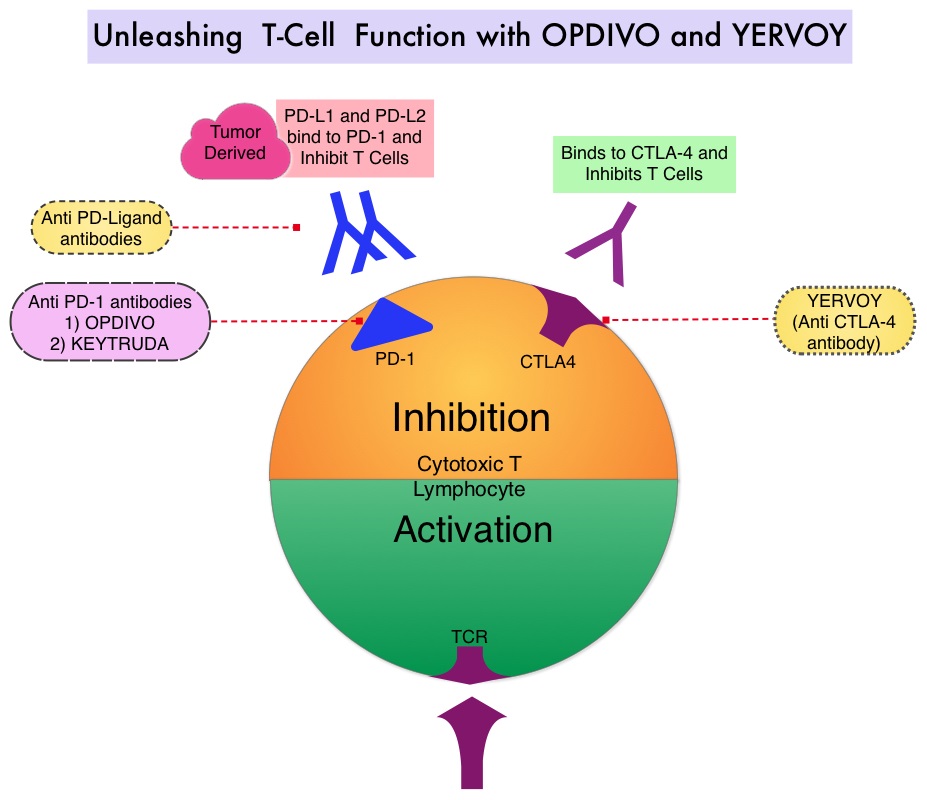
 Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4, also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. CA184-024 is a phase III trial in which treatment naïve patients with stage IIIc, N3 (unresectable), or stage IV melanoma were randomly assigned to receive YERVOY® 10 mg/kg IV given along with Dacarbazine 850 mg/m2 IV (N=250) or placebo plus Dacarbazine 850 mg/m2 IV (N=252) administered every 3 weeks for 4 doses followed by Dacarbazine given alone every 3 weeks through week 22. Responders and those with stable disease from week 12 through week 24 were then allowed to receive YERVOY® or placebo as maintenance therapy given every 12 weeks beginning at week 24, until disease progression or unacceptable toxicity. Dacarbazine was not given during the maintenance phase. The median Overall Survival was significantly longer in the group treated with YERVOY® plus Dacarbazine than in patients treated with placebo plus Dacarbazine (11.2 vs 9.1 months, HR=0.72; P< 0.001). This Overall Survival benefit was maintained after 3 years of follow up and toxicities were manageable.
Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4, also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. CA184-024 is a phase III trial in which treatment naïve patients with stage IIIc, N3 (unresectable), or stage IV melanoma were randomly assigned to receive YERVOY® 10 mg/kg IV given along with Dacarbazine 850 mg/m2 IV (N=250) or placebo plus Dacarbazine 850 mg/m2 IV (N=252) administered every 3 weeks for 4 doses followed by Dacarbazine given alone every 3 weeks through week 22. Responders and those with stable disease from week 12 through week 24 were then allowed to receive YERVOY® or placebo as maintenance therapy given every 12 weeks beginning at week 24, until disease progression or unacceptable toxicity. Dacarbazine was not given during the maintenance phase. The median Overall Survival was significantly longer in the group treated with YERVOY® plus Dacarbazine than in patients treated with placebo plus Dacarbazine (11.2 vs 9.1 months, HR=0.72; P< 0.001). This Overall Survival benefit was maintained after 3 years of follow up and toxicities were manageable.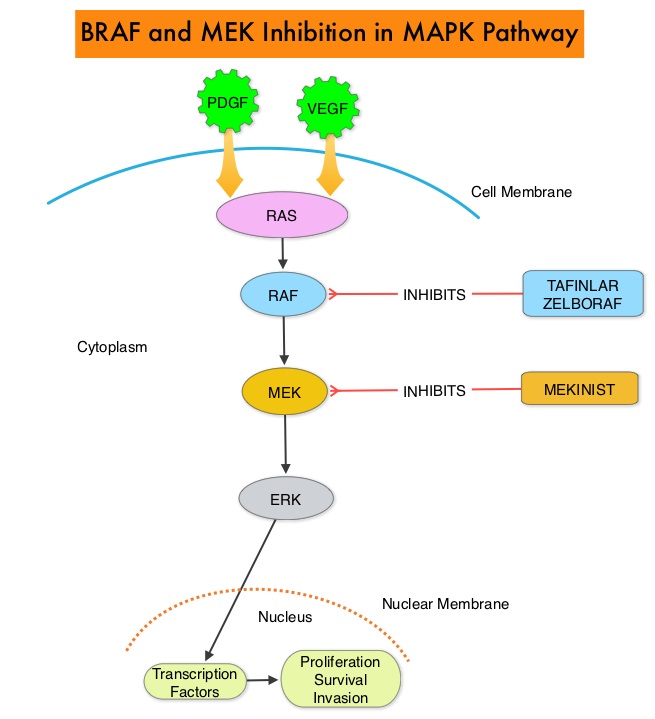 Squamous cell carcinoma’s were seen in about 6% of the patients treated with BRAF inhibitors. Paradoxical activation of the MAPK pathway in cells without a BRAF mutation has been implicated in the emergence of drug resistance and increased incidence of BRAF-inhibitor induced skin tumors. The addition of a MEK inhibitor such as MEKINIST® (Trametinib) to a BRAF inhibitor such as TAFINLAR®, has addressed some of these limitations, in previously published studies, with improvement in Progression Free Survival. MEKINIST® is a potent and selective inhibitor of MEK gene, which is downstream from RAF in the MAPK pathway and has been shown to significantly improve Progression Free Survival, Response Rate and Overall Survival, when compared to chemotherapy, in advanced melanoma patients with BRAF V600E/K mutations. The authors in this open label, randomized, phase III trial, evaluated the outcomes, comparing a combination of TAFINLAR® and MEKINIST® with single agent ZELBORAF® , in previously untreated and unresectable Stage IIIC or IV melanoma patients with BRAF V600E or V600K mutations. Eligible patients (N=704) were assigned in a 1:1 ratio to receive either a combination of TAFINLAR® (Dabrafenib), 150 mg PO BID and MEKINIST ® (Trametinib) 2 mg PO QD or ZELBORAF® (Vemurafenib) 960 mg PO BID, as first line therapy. The primary end point of this study was Overall Survival. Secondary end points included Progression Free Survival, Overall Response Rate, duration of response, and safety. At the preplanned interim analysis, the Overall Survival at 12 months was 72% in the combination therapy group and 65% in the single agent ZELBORAF® group (HR=0.69; P=0.005). The median Progression Free Survival was 11.4 months in the combination therapy group and 7.3 months in the ZELBORAF® group (HR=0.56; P<0.001). The objective response rate was 64% with combination therapy and 51% with single agent ZELBORAF® (P<0.001). There was no difference in the rates of severe adverse events and study drug discontinuations between the two groups. Skin cancers such as Squamous cell carcinoma and Keratoacanthoma occurred in 1% of patients in the combination therapy group and 18% of those treated with ZELBORAF® . The authors concluded that a combination of BRAF inhibitor TAFINLAR® and MEK inhibitor MEKINIST® significantly improved Overall Survival as compared with ZELBORAF® monotherapy, with a 31% relative reduction in the risk of death, in previously untreated patients with metastatic melanoma, with BRAF V600E or V600K mutations. This benefit was accomplished without increased overall toxicity. Robert C, Karaszewska B, Schachter J, et al. N Engl J Med 2015; 372:30-39
Squamous cell carcinoma’s were seen in about 6% of the patients treated with BRAF inhibitors. Paradoxical activation of the MAPK pathway in cells without a BRAF mutation has been implicated in the emergence of drug resistance and increased incidence of BRAF-inhibitor induced skin tumors. The addition of a MEK inhibitor such as MEKINIST® (Trametinib) to a BRAF inhibitor such as TAFINLAR®, has addressed some of these limitations, in previously published studies, with improvement in Progression Free Survival. MEKINIST® is a potent and selective inhibitor of MEK gene, which is downstream from RAF in the MAPK pathway and has been shown to significantly improve Progression Free Survival, Response Rate and Overall Survival, when compared to chemotherapy, in advanced melanoma patients with BRAF V600E/K mutations. The authors in this open label, randomized, phase III trial, evaluated the outcomes, comparing a combination of TAFINLAR® and MEKINIST® with single agent ZELBORAF® , in previously untreated and unresectable Stage IIIC or IV melanoma patients with BRAF V600E or V600K mutations. Eligible patients (N=704) were assigned in a 1:1 ratio to receive either a combination of TAFINLAR® (Dabrafenib), 150 mg PO BID and MEKINIST ® (Trametinib) 2 mg PO QD or ZELBORAF® (Vemurafenib) 960 mg PO BID, as first line therapy. The primary end point of this study was Overall Survival. Secondary end points included Progression Free Survival, Overall Response Rate, duration of response, and safety. At the preplanned interim analysis, the Overall Survival at 12 months was 72% in the combination therapy group and 65% in the single agent ZELBORAF® group (HR=0.69; P=0.005). The median Progression Free Survival was 11.4 months in the combination therapy group and 7.3 months in the ZELBORAF® group (HR=0.56; P<0.001). The objective response rate was 64% with combination therapy and 51% with single agent ZELBORAF® (P<0.001). There was no difference in the rates of severe adverse events and study drug discontinuations between the two groups. Skin cancers such as Squamous cell carcinoma and Keratoacanthoma occurred in 1% of patients in the combination therapy group and 18% of those treated with ZELBORAF® . The authors concluded that a combination of BRAF inhibitor TAFINLAR® and MEK inhibitor MEKINIST® significantly improved Overall Survival as compared with ZELBORAF® monotherapy, with a 31% relative reduction in the risk of death, in previously untreated patients with metastatic melanoma, with BRAF V600E or V600K mutations. This benefit was accomplished without increased overall toxicity. Robert C, Karaszewska B, Schachter J, et al. N Engl J Med 2015; 372:30-39
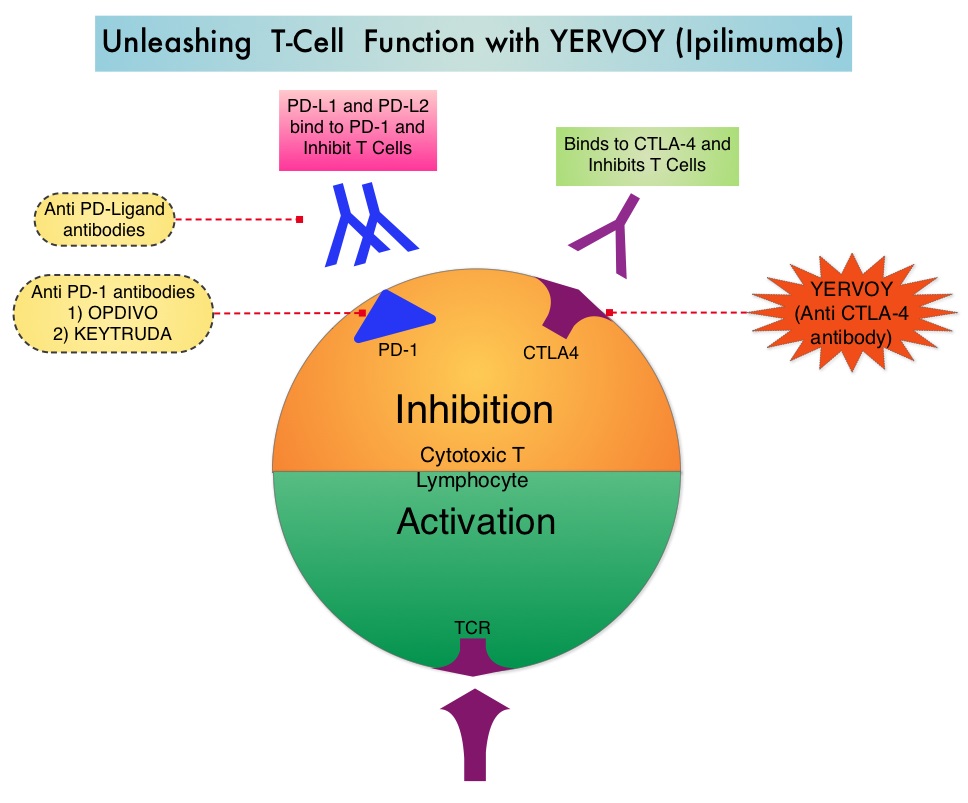
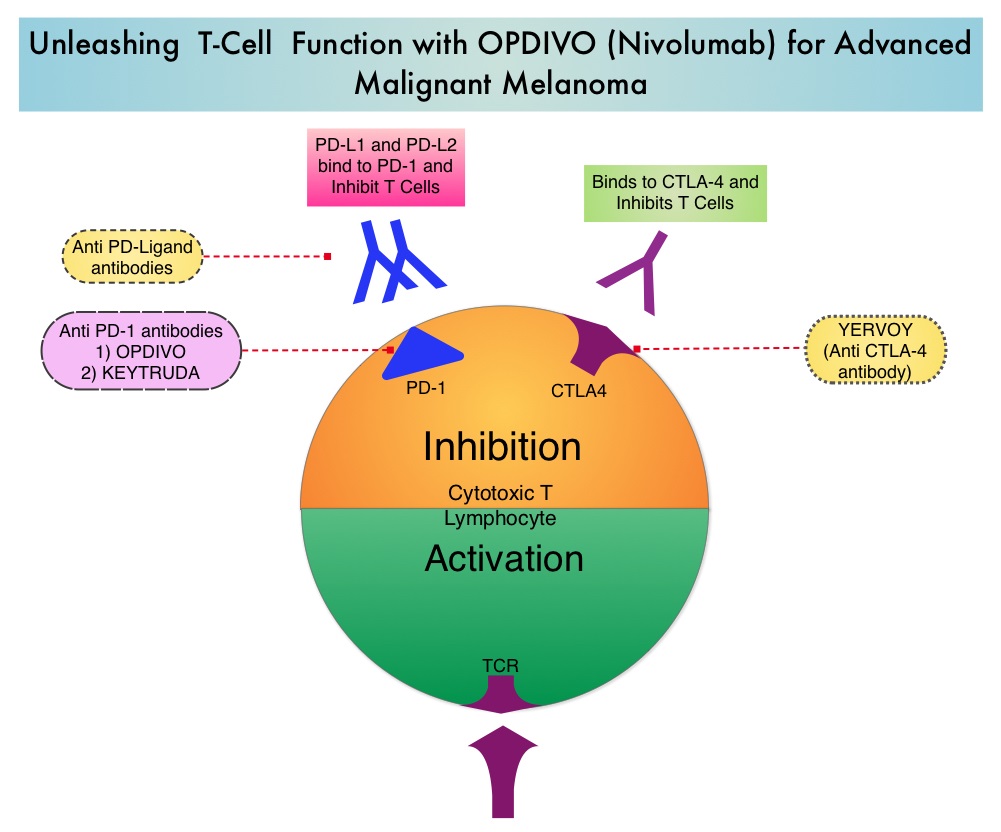 The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. OPDIVO® (Nivolumab) is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the T cells. OPDIVO® in previously conducted studies demonstrated durable antitumor activity and promising overall survival (OS) in pretreated patients. CheckMate-037 is an open label, randomized, phase III study, in which 370 patients with unresectable or metastatic melanoma, received OPDIVO® 3 mg/kg IV every 2 weeks (N=268) or investigator’s choice of chemotherapy, which included either Dacarbazine or a combination of Carboplatin plus Paclitaxel given every 3 weeks (N=102). Treatment was continued until disease progression or unacceptable toxicity. Eligible patients were required to have disease progression following YERVOY® (Ipilimumab) and a BRAF inhibitor if BRAF V600 mutation positive. The primary endpoints were ORR and overall survival. Early findings (Objective Response Rate-ORR) in the first 120 patients who were treated with OPDIVO® and in 47 patients treated with chemotherapy and had a minimum 6 months follow up (planned interim analysis), was presented at the 2014 ESMO Congress. The Objective Response Rate (ORR) was 32% in the OPDIVO® group and 11% in the chemotherapy group. The median time to response was 2.1 months in the OPDIVO® group and 3.5 months with chemotherapy. The majority, (95%) of responses at 6 months were ongoing in the OPDIVO® group and the median duration of response was not reached. The most common (greater than or equal to 20%) adverse reaction in the OPDIVO® group was rash. Grade 3 and 4 adverse events were seen in 2-5% of patients receiving OPDIVO® and included abdominal pain, hyponatremia, elevated liver enzymes and increased lipase. Clinically significant immune-mediated adverse reactions were pneumonitis, colitis, hepatitis, nephritis, and thyroid dysfunction. OPDIVO® is a new and novel treatment option for patients with advanced melanoma and is a welcome addition, as we try to better understand tumor immunology. Weber JS, Minor DR, D'Angelo S, et al. ESMO 2014, LBA3_PR
The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. OPDIVO® (Nivolumab) is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the T cells. OPDIVO® in previously conducted studies demonstrated durable antitumor activity and promising overall survival (OS) in pretreated patients. CheckMate-037 is an open label, randomized, phase III study, in which 370 patients with unresectable or metastatic melanoma, received OPDIVO® 3 mg/kg IV every 2 weeks (N=268) or investigator’s choice of chemotherapy, which included either Dacarbazine or a combination of Carboplatin plus Paclitaxel given every 3 weeks (N=102). Treatment was continued until disease progression or unacceptable toxicity. Eligible patients were required to have disease progression following YERVOY® (Ipilimumab) and a BRAF inhibitor if BRAF V600 mutation positive. The primary endpoints were ORR and overall survival. Early findings (Objective Response Rate-ORR) in the first 120 patients who were treated with OPDIVO® and in 47 patients treated with chemotherapy and had a minimum 6 months follow up (planned interim analysis), was presented at the 2014 ESMO Congress. The Objective Response Rate (ORR) was 32% in the OPDIVO® group and 11% in the chemotherapy group. The median time to response was 2.1 months in the OPDIVO® group and 3.5 months with chemotherapy. The majority, (95%) of responses at 6 months were ongoing in the OPDIVO® group and the median duration of response was not reached. The most common (greater than or equal to 20%) adverse reaction in the OPDIVO® group was rash. Grade 3 and 4 adverse events were seen in 2-5% of patients receiving OPDIVO® and included abdominal pain, hyponatremia, elevated liver enzymes and increased lipase. Clinically significant immune-mediated adverse reactions were pneumonitis, colitis, hepatitis, nephritis, and thyroid dysfunction. OPDIVO® is a new and novel treatment option for patients with advanced melanoma and is a welcome addition, as we try to better understand tumor immunology. Weber JS, Minor DR, D'Angelo S, et al. ESMO 2014, LBA3_PR
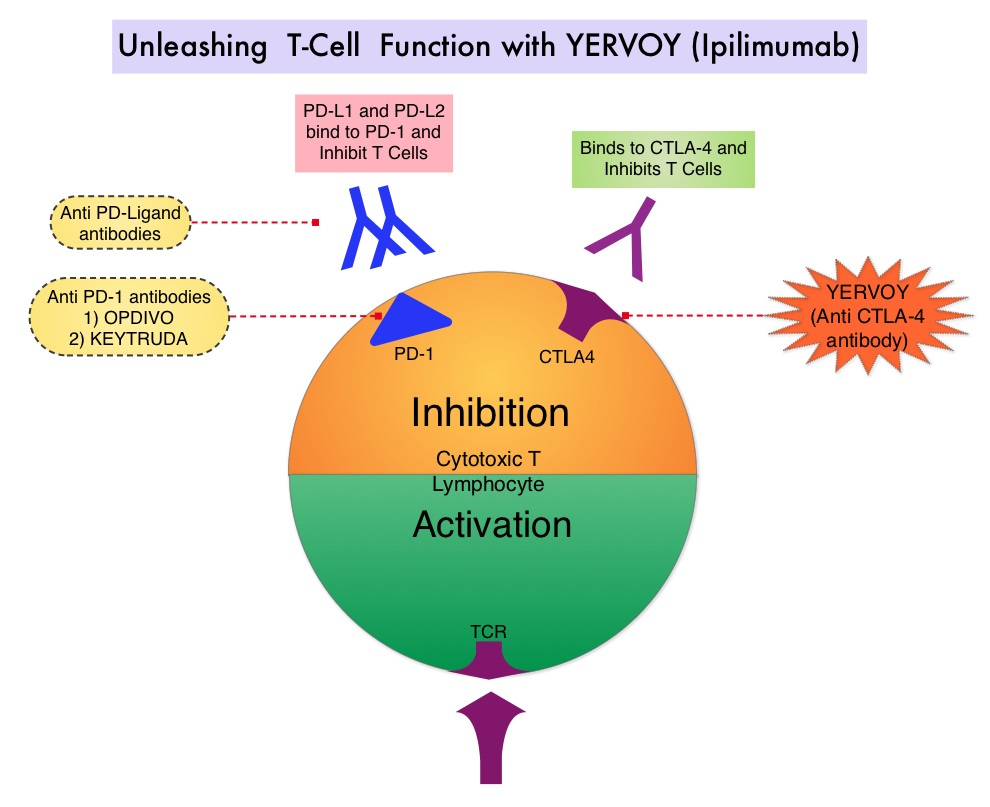
 Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The authors in this randomized study, compared the efficacy of YERVOY® (Ipilimumab) plus Sargramostim with YERVOY® alone, for treatment of metastatic melanoma. The rationale for this study was based on the synergy that was noted between YERVOY® and GM-CSF in preclinical models. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® is a fully human IgG1monoclonal antibody that blocks Immune checkpoint protein/receptor CTLA- 4 and counteracts immune regulatory cells. YERVOY® has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. GM-CSF is a cytokine that enhances the antitumor activity of T and B lymphocytes by activating the antigen presenting dendritic cells and recruiting macrophages. It however can induce negative regulatory immune responses.
Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152), PD-1(Programmed cell Death 1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The authors in this randomized study, compared the efficacy of YERVOY® (Ipilimumab) plus Sargramostim with YERVOY® alone, for treatment of metastatic melanoma. The rationale for this study was based on the synergy that was noted between YERVOY® and GM-CSF in preclinical models. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® is a fully human IgG1monoclonal antibody that blocks Immune checkpoint protein/receptor CTLA- 4 and counteracts immune regulatory cells. YERVOY® has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. GM-CSF is a cytokine that enhances the antitumor activity of T and B lymphocytes by activating the antigen presenting dendritic cells and recruiting macrophages. It however can induce negative regulatory immune responses.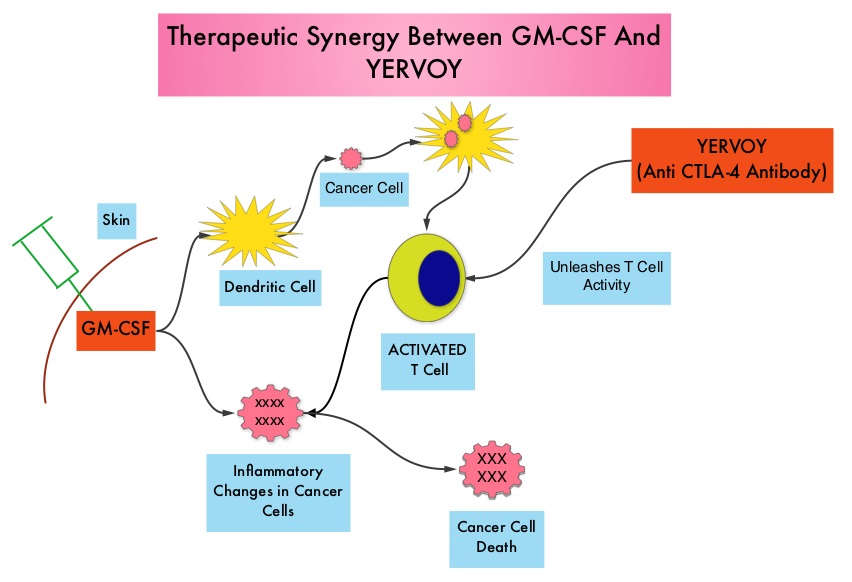 In this phase II randomized clinical trial conducted by the Eastern Cooperative Oncology Group (ECOG), patients with unresectable stage III or IV melanoma (N = 245), who had received at least 1 prior therapy and with no central nervous system metastases were randomized to receive either YERVOY® along with Sargramostim (N=123) or YERVOY® alone (N=122). Patients in the combination group (Group A) received YERVOY®10 mg/kg, IV on day 1 along with Sargramostim 250 μg given subcutaneously, on days 1 thru 14 of a 21day cycle, every 3 weeks for four cycles followed by YERVOY® maintenance every 12 weeks. Patients in Group B received YERVOY® alone. Treatment was continued until disease progression or uncontrolled toxicities. The primary endpoint was comparison of length of Overall Survival (OS). Secondary end points included Progression Free Survival (PFS), response rate, safety, and tolerability. With a median follow up of 13.3 months, the median OS for the combination of YERVOY® plus Sargramostim was 17.5 months vs 12.7 months for YERVOY® alone. The one year survival rate for YERVOY® plus Sargramostim was 68.9% compared to 52.9% for YERVOY® alone (HR=0.64; P=0.01). The median PFS was similar and was 3.1 months in both study groups. The explanation for similar PFS in both treatment groups may be due to both YERVOY® and Sargramostim bringing about inflammatory changes at the tumor sites, which in turn could be misinterpreted as disease progression, on radiological studies. The authors commented that PFS may not be an appropriate endpoint in immunotherapy trials. Grade 3 to 5 adverse events were less in the combination group (44.9%) compared to 58% for single agent YERVOY® (P=0.04). The authors concluded that treatment of unresectable stage III or IV melanoma patients with YERVOY® plus Sargramostim resulted in significantly longer overall survival with lower toxicities, compared to YERVOY® alone. Hodi SF, Lee S, McDermott DF, et al. JAMA 2014;312:1744-1753
In this phase II randomized clinical trial conducted by the Eastern Cooperative Oncology Group (ECOG), patients with unresectable stage III or IV melanoma (N = 245), who had received at least 1 prior therapy and with no central nervous system metastases were randomized to receive either YERVOY® along with Sargramostim (N=123) or YERVOY® alone (N=122). Patients in the combination group (Group A) received YERVOY®10 mg/kg, IV on day 1 along with Sargramostim 250 μg given subcutaneously, on days 1 thru 14 of a 21day cycle, every 3 weeks for four cycles followed by YERVOY® maintenance every 12 weeks. Patients in Group B received YERVOY® alone. Treatment was continued until disease progression or uncontrolled toxicities. The primary endpoint was comparison of length of Overall Survival (OS). Secondary end points included Progression Free Survival (PFS), response rate, safety, and tolerability. With a median follow up of 13.3 months, the median OS for the combination of YERVOY® plus Sargramostim was 17.5 months vs 12.7 months for YERVOY® alone. The one year survival rate for YERVOY® plus Sargramostim was 68.9% compared to 52.9% for YERVOY® alone (HR=0.64; P=0.01). The median PFS was similar and was 3.1 months in both study groups. The explanation for similar PFS in both treatment groups may be due to both YERVOY® and Sargramostim bringing about inflammatory changes at the tumor sites, which in turn could be misinterpreted as disease progression, on radiological studies. The authors commented that PFS may not be an appropriate endpoint in immunotherapy trials. Grade 3 to 5 adverse events were less in the combination group (44.9%) compared to 58% for single agent YERVOY® (P=0.04). The authors concluded that treatment of unresectable stage III or IV melanoma patients with YERVOY® plus Sargramostim resulted in significantly longer overall survival with lower toxicities, compared to YERVOY® alone. Hodi SF, Lee S, McDermott DF, et al. JAMA 2014;312:1744-1753
 The International Agency for Research on Cancer has classified Indoor tanning as a Class I carcinogen based on its significant association with malignant melanoma. Indoor tanning with resulting exposure to ultraviolet radiation is a potentially modifiable behavior and several studies to date have shown a relationship between indoor tanning and skin cancer. With this background, the authors reviewed the literature on indoor tanning and gathered data from 31 studies published in peer-reviewed journals that provided risk estimates. These studies included 14,956 cases with malignant melanoma and 233,106 controls. The main focus was to determine the risk of melanoma based on the frequency of use and exposure to the newer indoor tanning beds. They noted that among North Americans, there was a 34% increased risk of developing melanoma in individuals attending more than 10 tanning sessions. Further, those who started indoor tanning before age 25 years, had a 35% risk of developing melanoma and those who ever used indoor tanning were at a 23% increased risk of developing melanoma. It is hypothesized that the newer tanning bed bulb technology, which emits larger doses of long wave UVA rays, has resulted in a 22% increase in the risk of melanoma in individuals who ever used indoor tanning after the year 2000, compared to only 12% in the same population group before the year 2000. The authors concluded that the newer tanning technology is not safer than older techniques and patients should be educated and informed that using tanning beds can be associated with a subsequent diagnosis of malignant melanoma and therefore, cessation of indoor tanning should be strongly encouraged. Colantonio S, Bracken MB, Beecker J. J Am Acad Dermatol. 2014;70:847-857
The International Agency for Research on Cancer has classified Indoor tanning as a Class I carcinogen based on its significant association with malignant melanoma. Indoor tanning with resulting exposure to ultraviolet radiation is a potentially modifiable behavior and several studies to date have shown a relationship between indoor tanning and skin cancer. With this background, the authors reviewed the literature on indoor tanning and gathered data from 31 studies published in peer-reviewed journals that provided risk estimates. These studies included 14,956 cases with malignant melanoma and 233,106 controls. The main focus was to determine the risk of melanoma based on the frequency of use and exposure to the newer indoor tanning beds. They noted that among North Americans, there was a 34% increased risk of developing melanoma in individuals attending more than 10 tanning sessions. Further, those who started indoor tanning before age 25 years, had a 35% risk of developing melanoma and those who ever used indoor tanning were at a 23% increased risk of developing melanoma. It is hypothesized that the newer tanning bed bulb technology, which emits larger doses of long wave UVA rays, has resulted in a 22% increase in the risk of melanoma in individuals who ever used indoor tanning after the year 2000, compared to only 12% in the same population group before the year 2000. The authors concluded that the newer tanning technology is not safer than older techniques and patients should be educated and informed that using tanning beds can be associated with a subsequent diagnosis of malignant melanoma and therefore, cessation of indoor tanning should be strongly encouraged. Colantonio S, Bracken MB, Beecker J. J Am Acad Dermatol. 2014;70:847-857