
SUMMARY: The American Cancer Society estimates that about 22,440 women will be diagnosed with ovarian cancer in the United States for 2017 and about 14,080 will die of the disease. Ovarian cancer ranks fifth in cancer deaths among women, accounting for more deaths than any other cancer of the female reproductive system. Women who have reached menopause, women who have a family history of ovarian cancer, and women with the BRCA1 or BRCA2 genetic mutations have the highest risk for developing ovarian cancer. Over 75% of patients with ovarian cancer have advanced disease at the time of diagnosis. The FDA Safety Communication noted that despite extensive research and published studies there are currently no screening tests for ovarian cancer that are sensitive enough to reliably screen for ovarian cancer without a high number of inaccurate results.
The 2 tests used most often to screen for ovarian cancer are TransVaginal UltraSound (TVUS) and serum marker CA-125. TVUS is unable to differentiate benign from malignant ovarian mass. Serum marker CA-125 is usually associated with high-grade serous ovarian cancer, but is also expressed in normal tissues of the body such as the lungs and other reproductive organs. An increase in the serum marker CA-125 can be seen in non-malignant conditions such as endometriosis, peritonitis and in women with uterine fibroids. Even though serum marker CA-125 when elevated in patients, with an established diagnosis of ovarian cancer, is often used to follow the course of the disease, it has never been proven as an effective screening test for the early detection of ovarian cancer.
Nonetheless, numerous companies continue to claim that their commercially available diagnostic tests can effectively screen and detect ovarian cancer, with no data to support their claims. The FDA is concerned that women and their health care providers may rely on these inaccurate test results to make treatment decisions. Women with a false-positive result may undergo additional medical tests and/or unnecessary surgery, and may experience complications related to both. Conversely, women with a false-negative test may delay or not seek surgery or other treatment interventions for ovarian cancer. The later is particularly relevant for patients with BRCA mutations. Approximately 40% of BRCA1-mutation carriers and 18% of BRCA2-mutation carriers will develop ovarian cancer by age 70. It is recommended that patients who have BRCA1 mutations consider risk-reduction surgery (hysterectomy and bilateral bilateral salpingo-oophorectomy) by age 40 and those with BRCA2-mutations consider risk-reduction surgery no later than age 50.
Even though screenings for breast, colon and cervical cancers are successfully used for early detection and prevention of cancer-related deaths, a screening test for ovarian cancer with valid scientific data presently does not exist, and the FDA recommends against using currently offered tests to screen for ovarian cancer.
Recommendations:
For women, including those at increased risk of developing ovarian cancer
• Be aware that there is currently no safe and effective ovarian cancer screening test
• Do not rely on ovarian cancer screening test results to make health or treatment decisions
• Talk to your doctor about ways to reduce your risk of developing ovarian cancer, especially if you have a family history of ovarian cancer, or have the BRCA1 or BRCA2 genetic mutations
For physicians
• Do not recommend or use tests that claim to screen for ovarian cancer in the general population of women
• Be aware that testing higher risk asymptomatic patients for ovarian cancer has no proven benefit and is not a substitute for preventive actions that may reduce their risk
• Consider referring women at high risk of developing ovarian cancer, including those with BRCA mutations, to a genetic counselor or gynecologic oncologist, or other appropriate health care provider for more specialized care
U.S. Food and Drug Administration: The FDA recommends against using screening tests for ovarian cancer screening: FDA Safety Communication. Issued September 7, 2016. Available at http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm519413.htm
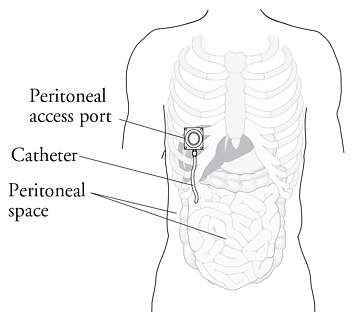 IP chemotherapy for ovarian cancer facilitates the exposure of tumors in the peritoneal cavity to 10-20 fold greater concentration of Cisplatin and Carboplatin and 1000 fold greater concentration of Paclitaxel, compared to IV administration, thus allowing continuous and prolonged exposure of the tumor to high drug concentrations, without systemic toxicities. Even though three Intergroup Phase III trials demonstrated the superiority of IP therapy over IV therapy, it has not been widely accepted in the US and abroad. Barriers to IP therapy have included inconvenience, IP catheter related complications, higher toxicities, lack of knowledge regarding patient selection for IP therapy as well as minimum number of cycles of IP therapy to administer and uncertain long term benefit.
IP chemotherapy for ovarian cancer facilitates the exposure of tumors in the peritoneal cavity to 10-20 fold greater concentration of Cisplatin and Carboplatin and 1000 fold greater concentration of Paclitaxel, compared to IV administration, thus allowing continuous and prolonged exposure of the tumor to high drug concentrations, without systemic toxicities. Even though three Intergroup Phase III trials demonstrated the superiority of IP therapy over IV therapy, it has not been widely accepted in the US and abroad. Barriers to IP therapy have included inconvenience, IP catheter related complications, higher toxicities, lack of knowledge regarding patient selection for IP therapy as well as minimum number of cycles of IP therapy to administer and uncertain long term benefit.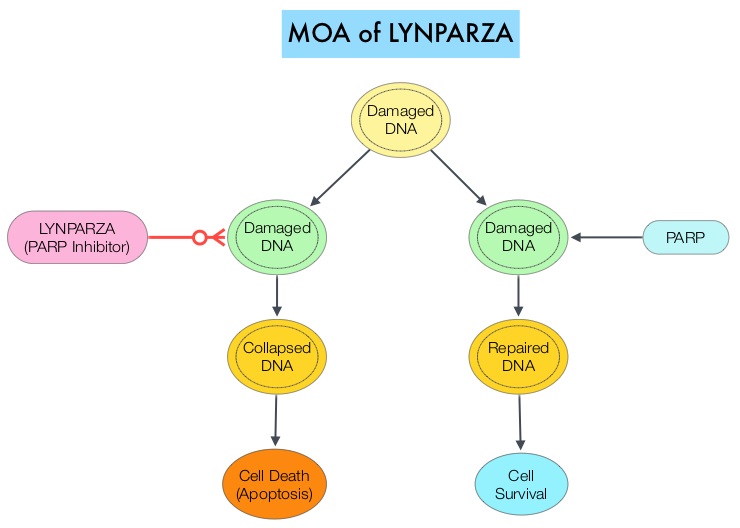 The PARP (Poly ADP Ribose Polymerase) family of enzymes which include PARP1 and PARP2, repair damaged DNA. LYNPARZA® is a PARP enzyme inhibitor that causes cell death in tumors that already have a DNA repair defect, such as those with BRCA1 and BRCA2 mutations. The approval of LYNPARZA® was based on a single arm phase II trial in which 137 platinum resistant ovarian cancer patients with measurable germline BRCA mutations were enrolled. The BRCA mutation status was verified retrospectively in 97% of the patients with available blood samples from the phase II study, using the BRACAnalysis CDx® test. These patients had received three or more lines of prior chemotherapy. Treatment consisted of LYNPARZA® administered orally twice a day and was continued until disease progression or unacceptable toxicity. The primary endpoint was Objective Response Rate (ORR). The Overall Response Rate was 34% and the median response duration was 7.9 months. In a larger cohort of patients reported by the authors (ovarian cancer cohort, N=193) the median Progression Free Survival was 7 months, 55% of patients were progression free at 6 months, the median Overall Survival was 16.6 months and 64.4% of patients were alive at 12 months. The most common adverse reactions associated with LYNPARZA® were anemia, nausea, fatigue (including asthenia), vomiting, diarrhea, dysgeusia, dyspepsia, headache, decreased appetite, nasopharyngitis/pharyngitis/URI, cough, arthralgia/musculoskeletal pain, myalgia, back pain, dermatitis/rash and abdominal pain/discomfort. This ground breaking therapy with LYNPARZA® is first of a new class of drugs, for treating ovarian cancer and along with the BRACAnalysis CDx® companion diagnostic test, is a significant milestone for patients with difficult-to-treat advanced ovarian cancer, with germline BRCA mutations. Kaufman B, Shapira-Frommer R, Schmutzler RK, et al. [published online November 3, 2014]. J Clin Oncol. doi:10.1200/JCO.2014.56.2728.
The PARP (Poly ADP Ribose Polymerase) family of enzymes which include PARP1 and PARP2, repair damaged DNA. LYNPARZA® is a PARP enzyme inhibitor that causes cell death in tumors that already have a DNA repair defect, such as those with BRCA1 and BRCA2 mutations. The approval of LYNPARZA® was based on a single arm phase II trial in which 137 platinum resistant ovarian cancer patients with measurable germline BRCA mutations were enrolled. The BRCA mutation status was verified retrospectively in 97% of the patients with available blood samples from the phase II study, using the BRACAnalysis CDx® test. These patients had received three or more lines of prior chemotherapy. Treatment consisted of LYNPARZA® administered orally twice a day and was continued until disease progression or unacceptable toxicity. The primary endpoint was Objective Response Rate (ORR). The Overall Response Rate was 34% and the median response duration was 7.9 months. In a larger cohort of patients reported by the authors (ovarian cancer cohort, N=193) the median Progression Free Survival was 7 months, 55% of patients were progression free at 6 months, the median Overall Survival was 16.6 months and 64.4% of patients were alive at 12 months. The most common adverse reactions associated with LYNPARZA® were anemia, nausea, fatigue (including asthenia), vomiting, diarrhea, dysgeusia, dyspepsia, headache, decreased appetite, nasopharyngitis/pharyngitis/URI, cough, arthralgia/musculoskeletal pain, myalgia, back pain, dermatitis/rash and abdominal pain/discomfort. This ground breaking therapy with LYNPARZA® is first of a new class of drugs, for treating ovarian cancer and along with the BRACAnalysis CDx® companion diagnostic test, is a significant milestone for patients with difficult-to-treat advanced ovarian cancer, with germline BRCA mutations. Kaufman B, Shapira-Frommer R, Schmutzler RK, et al. [published online November 3, 2014]. J Clin Oncol. doi:10.1200/JCO.2014.56.2728.