
SUMMARY:The FDA recently approved AVASTIN® (Bevacizumab) in combination with chemotherapy for the treatment of patients with platinum-resistant, recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer. It is estimated that in the United States, approximately 22,000 women will be diagnosed with ovarian cancer in 2014 and a little over 14,000 women will die of the disease. In spite of significantly improved median survival following aggressive surgical debulking and platinum plus taxane based therapy, long term cure rate is approximately 20-30%. Majority of the patients relapse in 18-24 months and 25% of these patients are Platinum Resistant. These platinum resistant patients are usually treated with single agent chemotherapy drugs such as DOXIL® (Pegylated Liposomal Doxorubicin-PLD), TAXOL® (Paclitaxel) and HYCAMTIN® (Topotecan), with an expected response rate of 10-15%, median response duration of about 3-4 months and median Overall Survival of approximately 12 months. AURELIA (Avastin Use in Platinum-Resistant Epithelial Ovarian Cancer) is a multicenter, randomized, open-label, Phase III study in which 361 women with platinum resistant recurrent epithelial ovarian, primary peritoneal or fallopian tube cancer were enrolled. These patients had disease progression within six months of their platinum based chemotherapy (Platinum Resistant) and were randomly assigned to receive AVASTIN® (Bevacizumab) 10 mg/kg every 2 weeks or 15 mg/kg every 3 weeks in combination with investigators choice of single agent chemotherapy agent (N=179) or single agent chemotherapy alone (N=182). Chemotherapy included one of the following agents – TAXOL® 80 mg/m2 on days 1, 8, 15 and 22 every 4 weeks, DOXIL® 40 mg/m2 on day 1 every 4 weeks or HYCAMTIN® either 4 mg/m2 on days 1, 8 and 15 every 4 weeks or 1.25 mg/m2 on days 1-5 every 3 weeks. Patients with refractory disease, history of bowel obstruction, or those who had received two or more prior anticancer regimens were excluded. Treatment was given until disease progression. Patients who had progressed on single agent chemotherapy were allowed to cross over to AVASTIN® group. 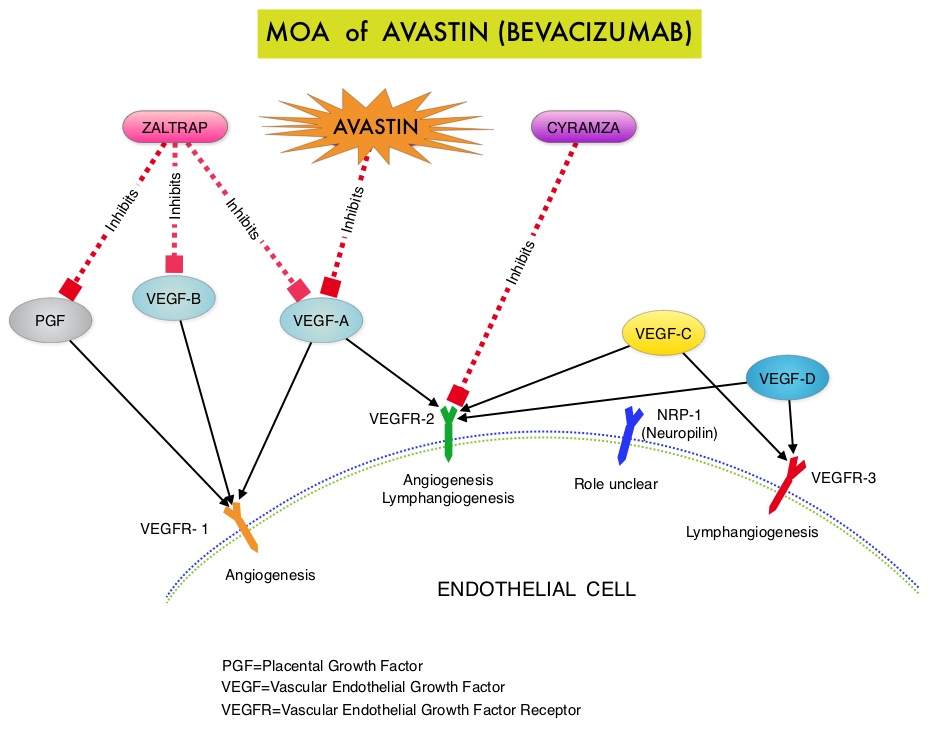 The primary end point was Progression Free Survival (PFS) and secondary end points included Objective Response Rate (ORR), Overall Survival (OS), safety, and patient reported outcomes. The combination of AVASTIN® plus chemotherapy resulted in a 62% reduction in the risk of progression compared to those who received chemotherapy alone, with a median PFS of 6.8 months for the AVASTIN® plus chemotherapy group versus 3.4 months for the single agent chemotherapy group (HR=0.38, P<0.0001) and thus met the primary endpoint of this clinical trial. This PFS benefit was seen consistently across all subgroups including the subgroup of patients with ascites. The ORR was 27.3% with the AVASTIN® combination versus 11.8% with single agent chemotherapy (P =0.001). The median OS was 16.6 months for the AVASTIN® combination versus 13.3 months for the single agent chemotherapy group (HR=0.85; P < .17). The lack of statistical significance in the OS has been attributed to cross over of 40% of patients, initially randomized to the chemotherapy alone group, who upon progression received AVASTIN®. There was a 15% improvement in abdominal and GI symptoms as reported by patients, with the AVASTIN® combination, compared to chemotherapy alone. On exploratory analyses it was noted that the addition of AVASTIN® to TAXOL® resulted in the most benefit, with a 5.7 month improvement in median PFS (9.6 versus 3.9 months), a 23% improvement in the overall response rate (53% versus 30%) and a 9.2 month improvement in median OS (22.4 versus 13.2 months) compared to single agent TAXOL®. This benefit was seen in spite of the fact that 97% of the patients in the TAXOL® group had received this agent with previous chemotherapy regimens. These findings suggest that patients who have received prior treatment with TAXOL® may benefit from AVASTIN® plus weekly TAXOL®. The most common adverse reactions (greater than or equal to 15%) in patients treated with AVASTIN® plus chemotherapy were neutropenia, peripheral neuropathy, hypertension and GI perforation occurred in 1.7% of these patients. This low perforation rate has been attributed to the exclusion of patients with rectosigmoid involvement by pelvic examination or bowel involvement on CT scan as well as those with clinical symptoms of bowel obstruction. The authors concluded that AVASTIN® in combination with chemotherapy significantly improved Progression Free Survival and Objective Response Rates in patients with Platinum Resistant Recurrent Ovarian Cancer. Pujade-Lauraine E, Hilpert F, Weber B, et al. J Clin Oncol 2014;32:1302-1308
The primary end point was Progression Free Survival (PFS) and secondary end points included Objective Response Rate (ORR), Overall Survival (OS), safety, and patient reported outcomes. The combination of AVASTIN® plus chemotherapy resulted in a 62% reduction in the risk of progression compared to those who received chemotherapy alone, with a median PFS of 6.8 months for the AVASTIN® plus chemotherapy group versus 3.4 months for the single agent chemotherapy group (HR=0.38, P<0.0001) and thus met the primary endpoint of this clinical trial. This PFS benefit was seen consistently across all subgroups including the subgroup of patients with ascites. The ORR was 27.3% with the AVASTIN® combination versus 11.8% with single agent chemotherapy (P =0.001). The median OS was 16.6 months for the AVASTIN® combination versus 13.3 months for the single agent chemotherapy group (HR=0.85; P < .17). The lack of statistical significance in the OS has been attributed to cross over of 40% of patients, initially randomized to the chemotherapy alone group, who upon progression received AVASTIN®. There was a 15% improvement in abdominal and GI symptoms as reported by patients, with the AVASTIN® combination, compared to chemotherapy alone. On exploratory analyses it was noted that the addition of AVASTIN® to TAXOL® resulted in the most benefit, with a 5.7 month improvement in median PFS (9.6 versus 3.9 months), a 23% improvement in the overall response rate (53% versus 30%) and a 9.2 month improvement in median OS (22.4 versus 13.2 months) compared to single agent TAXOL®. This benefit was seen in spite of the fact that 97% of the patients in the TAXOL® group had received this agent with previous chemotherapy regimens. These findings suggest that patients who have received prior treatment with TAXOL® may benefit from AVASTIN® plus weekly TAXOL®. The most common adverse reactions (greater than or equal to 15%) in patients treated with AVASTIN® plus chemotherapy were neutropenia, peripheral neuropathy, hypertension and GI perforation occurred in 1.7% of these patients. This low perforation rate has been attributed to the exclusion of patients with rectosigmoid involvement by pelvic examination or bowel involvement on CT scan as well as those with clinical symptoms of bowel obstruction. The authors concluded that AVASTIN® in combination with chemotherapy significantly improved Progression Free Survival and Objective Response Rates in patients with Platinum Resistant Recurrent Ovarian Cancer. Pujade-Lauraine E, Hilpert F, Weber B, et al. J Clin Oncol 2014;32:1302-1308
Tag: Ovarian Cancer
AVASTIN® (Bevacizumab)
The FDA on August 14, 2014 approved AVASTIN® for the treatment of patients with persistent, recurrent or metastatic Cervical Cancer, in combination with TAXOL® (Paclitaxel) and Cisplatin or TAXOL® and Topotecan (HYCAMTIN®). AVASTIN® is a product of Genentech, Inc.
Bevacizumab Combined With Chemotherapy for Platinum-Resistant Recurrent Ovarian Cancer The AURELIA Open-Label Randomized Phase III Trial
SUMMARY: It is estimated that in the United States, approximately 22,000 women will be diagnosed with ovarian cancer in 2014 and a little over 14,000 women will die of the disease. In spite of significantly improved median survival following aggressive surgical debulking and platinum plus taxane based therapy, long term cure rate is approximately 20-30%. Majority of the patients relapse in 18-24 months and 25% of these patients are Platinum Resistant. These platinum resistant patients are usually treated with single agent chemotherapy drugs such as DOXIL® (Pegylated Liposomal Doxorubicin-PLD), TAXOL® (Paclitaxel) and HYCAMTIN® (Topotecan), with an expected response rate of 10-15%, median response duration of about 3-4 months and median Overall Survival of approximately 12 months. AURELIA (Avastin Use in Platinum-Resistant Epithelial Ovarian Cancer) is a multicenter, randomized, open-label, Phase III study in which 361 women with platinum resistant recurrent epithelial ovarian, primary peritoneal or fallopian tube cancer were enrolled. These patients had disease progression within six months of their platinum based chemotherapy (Platinum Resistant) and were randomly assigned to receive AVASTIN® (Bevacizumab) 10 mg/kg every 2 weeks or 15 mg/kg every 3 weeks in combination with investigators choice of single agent chemotherapy agent such as weekly TAXOL®, HYCAMTIN®, DOXIL® (N=179) or single agent chemotherapy alone (N=182). Patients with refractory disease, history of bowel obstruction, or those who had received two or more prior anticancer regimens were excluded. Treatment was given until disease progression. Patients who had progressed on single agent chemotherapy were allowed to cross over to single agent AVASTIN®. The primary end point was Progression Free Survival (PFS) and secondary end points included Objective Response Rate (ORR), Overall Survival (OS), safety, and patient reported outcomes. The combination of AVASTIN® plus chemotherapy resulted in a 52% reduction in the risk of progression compared to those who received chemotherapy alone, with a median PFS of 6.7 months for the AVASTIN® plus chemotherapy group vs 3.4 months for the single agent chemotherapy group (HR=0.48, P<0.001) and thus met the primary endpoint of this clinical trial. This PFS benefit was seen consistently across all subgroups including the subgroup of patients with ascites. The ORR was 27.3% with the AVASTIN® combination vs 11.8% with single agent chemotherapy (P =0.001). The median OS was 16.6 months for the AVASTIN® combination vs 13.3 months for the single agent chemotherapy group (HR=0.85; P < .17). The lack of statistical significance in the OS has been attributed to cross over of 40% of patients, initially randomized to the chemotherapy alone group, who upon progression, received single agent AVASTIN®. As expected, grade 2 or more hypertension and proteinuria were common in the AVASTIN® group and GI perforation occurred in 2.2% of these patients. There was a 15% improvement in abdominal and GI symptoms as reported by patients, with the AVASTIN® combination, compared to chemotherapy alone. The authors concluded that AVASTIN® in combination with chemotherapy significantly improved Progression Free Survival and Objective Response Rates in patients with Platinum Resistant recurrent Ovarian Cancer. Pujade-Lauraine E, Hilpert F, Weber B, et al. J Clin Oncol 2014;32:1302-1308
AURELIA (Avastin Use in Platinum-Resistant Epithelial Ovarian Cancer) is a multicenter, randomized, open-label, Phase III study in which 361 women with platinum resistant recurrent epithelial ovarian, primary peritoneal or fallopian tube cancer were enrolled. These patients had disease progression within six months of their platinum based chemotherapy (Platinum Resistant) and were randomly assigned to receive AVASTIN® (Bevacizumab) 10 mg/kg every 2 weeks or 15 mg/kg every 3 weeks in combination with investigators choice of single agent chemotherapy agent such as weekly TAXOL®, HYCAMTIN®, DOXIL® (N=179) or single agent chemotherapy alone (N=182). Patients with refractory disease, history of bowel obstruction, or those who had received two or more prior anticancer regimens were excluded. Treatment was given until disease progression. Patients who had progressed on single agent chemotherapy were allowed to cross over to single agent AVASTIN®. The primary end point was Progression Free Survival (PFS) and secondary end points included Objective Response Rate (ORR), Overall Survival (OS), safety, and patient reported outcomes. The combination of AVASTIN® plus chemotherapy resulted in a 52% reduction in the risk of progression compared to those who received chemotherapy alone, with a median PFS of 6.7 months for the AVASTIN® plus chemotherapy group vs 3.4 months for the single agent chemotherapy group (HR=0.48, P<0.001) and thus met the primary endpoint of this clinical trial. This PFS benefit was seen consistently across all subgroups including the subgroup of patients with ascites. The ORR was 27.3% with the AVASTIN® combination vs 11.8% with single agent chemotherapy (P =0.001). The median OS was 16.6 months for the AVASTIN® combination vs 13.3 months for the single agent chemotherapy group (HR=0.85; P < .17). The lack of statistical significance in the OS has been attributed to cross over of 40% of patients, initially randomized to the chemotherapy alone group, who upon progression, received single agent AVASTIN®. As expected, grade 2 or more hypertension and proteinuria were common in the AVASTIN® group and GI perforation occurred in 2.2% of these patients. There was a 15% improvement in abdominal and GI symptoms as reported by patients, with the AVASTIN® combination, compared to chemotherapy alone. The authors concluded that AVASTIN® in combination with chemotherapy significantly improved Progression Free Survival and Objective Response Rates in patients with Platinum Resistant recurrent Ovarian Cancer. Pujade-Lauraine E, Hilpert F, Weber B, et al. J Clin Oncol 2014;32:1302-1308
ICON7 Final overall survival results in the GCIG phase III randomized trial of bevacizumab in women with newly diagnosed ovarian cancer
SUMMARY: ICON7 is a randomized phase III trial in which the safety and efficacy of combining AVASTIN® (Bevacizumab) with standard chemotherapy was evaluated in patients with Newly Diagnosed Ovarian Cancer. One thousand five hundred and twenty eight (n=1528) patients with high-risk (grade 3 or clear cell histology) stage I-IIa or stage IIb-IV epithelial ovarian, primary peritoneal or fallopian tube cancer, were randomized to receive either 6 cycles of combination chemotherapy with PARAPLATIN® (Carboplatin) AUC of 5 or 6 and TAXOL® (Paclitaxel) 175mg/m2 given every 3 weeks or the same chemotherapy regimen given concurrently with AVASTIN® (Bevacizumab) 7.5mg/kg, every 3 weeks for 5 or 6 cycles followed maintenance AVASTIN® for 12 additional cycles or until disease progression, whichever was the earlier. The median age was 57 years. Approximately 33% of the patients randomized were considered poor prognosis group, at high risk for progression. At the first interim analysis, the addition of AVASTIN® to standard chemotherapy, followed by maintenance AVASTIN® demonstrated improved Progression Free Survival (PFS) compared to standard chemotherapy alone (19 vs17.3 months, P=0.0041). In the planned Final analysis, at a median follow up of 49 months, the PFS superiority in the AVASTIN® group was maintained, similar to the first analysis but there was no improvement in the median Overall Survival (OS) between the two treatment groups. However, in the predefined high-risk, poor prognostic subgroup of patients, AVASTIN® improved OS by 4.8 months, without any major adverse events. The authors concluded that the addition of AVASTIN® to standard chemotherapy can translate into clinically meaningful survival benefit, for patients with high risk disease. Oza AM, Perren TJ, Swart AM, et al. European Cancer Congress. Abstract 6. Presented on September 29, 2013.
AURELIA A randomized phase III trial evaluating bevacizumab (BEV) plus chemotherapy (CT) for platinum (PT)-resistant recurrent ovarian cancer (OC)
SUMMARY: AURELIA is a multicenter, randomized, open-label, two-arm Phase III study in which 361 women with platinum-resistant recurrent epithelial ovarian, primary peritoneal or fallopian tube cancer were enrolled. These patients had disease progression within six months of their platinum based chemotherapy. Patients were randomly assigned to receive AVASTIN® (Bevacizumab) in combination with chemotherapy which included weekly paclitaxel, topotecan or pegylated liposomal doxorubicin or chemotherapy alone. The primary end point was Progression Free Survival. There was a 52% reduction in the risk of progression in those who received AVASTIN® plus chemotherapy compared to those who received chemotherapy alone (HR=0.48, P<0.001). Further, there was a significantly higher objective response rate in the AVASTIN® group compared to those who received chemotherapy alone (30.9 percent vs. 12.6 percent, p=0.001). Pujade-Lauraine E, Hilpert F, Weber B, et al. J Clin Oncol 30, 2012 (suppl; abstr LBA5002)
Phase III trial of bevacizumab (BEV) in the primary treatment of advanced epithelial ovarian cancer (EOC), primary peritoneal cancer (PPC), or fallopian tube cancer (FTC) A Gynecologic Oncology Group study
SUMMARY: The role of Bevacizumab (AVASTIN®) in the treatment of advanced ovarian cancer was evaluated in a large randomized double blind phase III trial. One thousand eight hundred and seventy three (1873) patients with stage III or IV disease, who were treatment naïve, were randomly assigned to one of three treatment groups – standard chemotherapy with paclitaxel and carboplatin given along with a placebo followed maintenance treatment with a placebo, standard chemotherapy given along with AVASTIN® followed by maintenance treatment with a placebo or standard chemotherapy given along with AVASTIN® followed by maintenance treatment with AVASTIN®. Patients receiving standard chemotherapy along with AVASTIN® followed by maintenance AVASTIN® had a median Progression Free Survival of 14.1 months compared to 10.3 months for those who received standard chemotherapy alone. Interestingly, outcomes in patients receiving standard chemotherapy along with AVASTIN® followed by placebo maintenance did no better than those who received standard chemotherapy alone. To date, addition of AVASTIN® to standard chemotherapy followed by AVASTIN® maintenance has not resulted in significant improvement in overall survival. J Clin Oncol 28:18s, 2010 (suppl; abstr LBA1)
Oncoprescribe Blog Ovarian Cancer Screening
Ovarian cancer is potentially curable if diagnosed at an early stage. Unfortunately only 20-25% of the patients are diagnosed with early stage disease, ie. Stage I and Stage II. Majority of the patients with ovarian cancer are diagnosed with Stage III or Stage IV disease. Screening postmenopausal women or those considered to be at high risk therefore makes perfect sense. A British study presented at ASCO 2010, screened postmenopausal women, considered not to be at high risk,with a combination of pelvic ultrasound and CA-125. Preliminary data is very promising and screening techniques were able to diagnose ovarian cancer at an earlier stage.
It is possible that we may have an algorithm to screen for ovarian cancer, in the very near future.
Oncoprescribe Blog Improving Progression Free Survival with Bevacizumab in Ovarian Cancer patients
Taxanes were first introduced in the mid 1990’s for the first line treatment of ovarian cancer. There has since been no real progress made. However recent data presented at ESMO (European Society for Medical Oncology) 2010, shed light on the benefit of adding Bevacizumab to standard chemotherapy. In the ICON 7 trial, 1,528 women with high risk, early or advanced stage ovarian cancer were randomized to receive either 6 cycles of standard chemotherapy with Carboplatin and Paclitaxel or Carboplatin and Paclitaxel given along with Bevacizumab, followed by maintenance Bevacizumab for an additional 12 cycles.
There was a significant improvement in the median progression free survival in the Bevacizumab group. Patients with poor risk features benefited the most. So, after over 15 years of drought, we are now seeing progress made, in the treatment of ovarian cancer. It is not clear at this time however, if this three drug combination will improve Overall Survival.