
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer and 1 in 7 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, about 180,890 new cases of prostate cancer will be diagnosed in 2016 and over 26,000 men will die of the disease. The widespread use of PSA testing in the recent years has resulted in a dramatic increase in the diagnosis and treatment of prostate cancer. The management of clinically localized prostate cancer that is detected based on Prostate Specific Antigen (PSA) levels remains controversial and management strategies for these patients have included Surgery, Radiotherapy or Active Monitoring. However, it has been proposed that given the indolent nature of prostate cancer in general, majority of the patients do not benefit from treatment intervention and many patients die of competing causes. Further, treatment intervention can result in adverse effects on sexual, urinary, or bowel function. The U.S. Preventive Services Task Force (USPSTF) has recommended that population screening for prostate cancer should not be adopted as a public health policy, because the risks appeared to outweigh benefits, from detecting and treating PSA-detected prostate cancer. Previously published trials evaluated the effectiveness of treatment, but they did not compare Surgery, Radiotherapy and Active Monitoring.
Prostate Testing for Cancer and Treatment (ProtecT) study is a prospective, randomized trial, which compared Active Monitoring, Radical Prostatectomy, and External Beam Radiotherapy, for the treatment of PSA-detected clinically localized prostate cancer. A total of 1,643 patients were randomly assigned to Radical Prostatectomy (N=553), Radiotherapy (N=545) or Active Monitoring (N=545). Patients in the Active Monitoring group were evaluated every 3 months for the first year, then every 6-12 months thereafter and radical treatment with curative intent was offered, based on changes in PSA levels. This is different from “watchful waiting”, which has no planned curative radical treatment on disease progression. The median age in this study was 62 yrs, the median PSA level was 4.6 ng/ml, 77% had tumors with a Gleason score of 6 and 76% had Stage T1c disease. The primary end point was prostate cancer mortality at a median of 10 years of follow-up, with prostate cancer-related deaths defined as deaths that were definitely or probably due to prostate cancer or its treatment. Secondary end points included all-cause mortality and the rates of metastases, clinical progression, primary treatment failure, and treatment complications.
At a median follow up of 10 years, prostate cancer-specific mortality was low at approximately 1% irrespective of treatment and all-cause mortality was also low at approximately 10%. However, higher rates of disease progression were seen in the Active Monitoring group (22.9 events per 1000 person-years) compared to the Surgery group (8.9 events per 1000 person-years) or the Radiotherapy group (9.0 events per 1000 person-years). This meant that patients assigned to Active Monitoring were significantly more likely to have metastatic disease than those assigned to treatment (P<0.001 for the overall comparison).
The authors in a companion article (N Engl J Med. DOI: 10.1056/NEJMoa1606221) focused on the patient-reported outcomes after Monitoring, Surgery and Radiotherapy over 6 years of follow up. Prostatectomy had the greatest negative effect on urinary continence and sexual function, whereas Radiotherapy plus neoadjuvant androgen-deprivation therapy had more of a negative effect on bowel function, urinary voiding and nocturia, although patients recovered some function over time. Approximately 44% of the patient’s who were assigned to Active Monitoring, did not receive radical curative treatment and were able to avoid these toxicities.
It was concluded that at a median follow up of 10 yrs, prostate cancer-specific mortality was low, irrespective of the treatment given, with similar efficacy outcomes but with a variable impact on quality of life. However, it should be noted that patients assigned to Active Monitoring were significantly more likely to have metastatic disease than those assigned to treatment. This in turn would warrant salvage treatment, which could result in toxicities as well. Further follow up, evaluating long term survival and the accompanying risk/benefits, will allow patients to make informed decisions, with regards to the treatment options, for clinically localized prostate cancer. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. Hamdy FC, Donovan JL, Lane JA, et al. for the ProtecT Study Group. September 14, 2016DOI: 10.1056/NEJMoa1606220
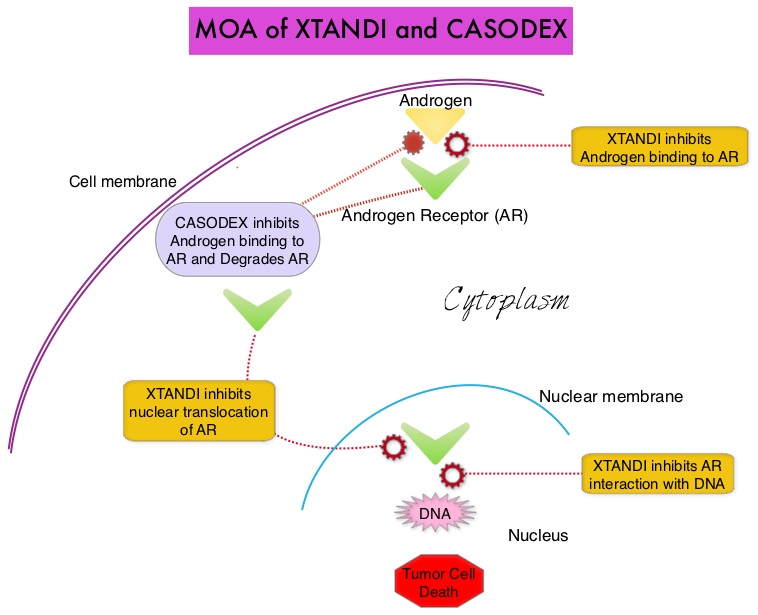
 They include ZYTIGA® (Abiraterone) and XTANDI® (Enzalutamide). ZYTIGA® inhibits CYP 17A1 enzyme thus decreasing androgen biosynthesis and depletes adrenal and intratumoral androgens. XTANDI® competes with Testosterone and Dihydrotestosterone and avidly binds to the Androgen Receptor (AR), thereby inhibiting AR signaling and in addition inhibits translocation of the AR into the nucleus and thus inhibits the transcriptional activities of the AR. There is presently very little guidance with regards to the sequencing of these two oral agents after progression on TAXOTERE®, in patients with metastatic CRPC. ZYTIGA® was approved initially by the FDA in April 2011, for use in combination with prednisone for the treatment of patients with metastatic CRPC, who had received prior chemotherapy containing TAXOTERE®. Treatment with ZYTIGA® resulted in a 35% reduction in the risk of death and a 36% increase in median Overall Survival (OS) compared with placebo. Subsequently, XTANDI® was approved by the FDA on August 31, 2012 for the treatment of patients with metastatic CRPC who had previously received TAXOTERE®. XTANDI® improved median OS and reduced the risk of death by 37% when compared to placebo. Even though these two anti-androgen therapies improved OS in metastatic CRPC patients previously treated with TAXOTERE®, the proper sequence of administration of these two agents after TAXOTERE® failure, has remained unclear. At least 2 published studies have shown that the use of ZYTIGA® as third line therapy after progression on TAXOTERE® and XTANDI® resulted in inferior outcomes.
They include ZYTIGA® (Abiraterone) and XTANDI® (Enzalutamide). ZYTIGA® inhibits CYP 17A1 enzyme thus decreasing androgen biosynthesis and depletes adrenal and intratumoral androgens. XTANDI® competes with Testosterone and Dihydrotestosterone and avidly binds to the Androgen Receptor (AR), thereby inhibiting AR signaling and in addition inhibits translocation of the AR into the nucleus and thus inhibits the transcriptional activities of the AR. There is presently very little guidance with regards to the sequencing of these two oral agents after progression on TAXOTERE®, in patients with metastatic CRPC. ZYTIGA® was approved initially by the FDA in April 2011, for use in combination with prednisone for the treatment of patients with metastatic CRPC, who had received prior chemotherapy containing TAXOTERE®. Treatment with ZYTIGA® resulted in a 35% reduction in the risk of death and a 36% increase in median Overall Survival (OS) compared with placebo. Subsequently, XTANDI® was approved by the FDA on August 31, 2012 for the treatment of patients with metastatic CRPC who had previously received TAXOTERE®. XTANDI® improved median OS and reduced the risk of death by 37% when compared to placebo. Even though these two anti-androgen therapies improved OS in metastatic CRPC patients previously treated with TAXOTERE®, the proper sequence of administration of these two agents after TAXOTERE® failure, has remained unclear. At least 2 published studies have shown that the use of ZYTIGA® as third line therapy after progression on TAXOTERE® and XTANDI® resulted in inferior outcomes.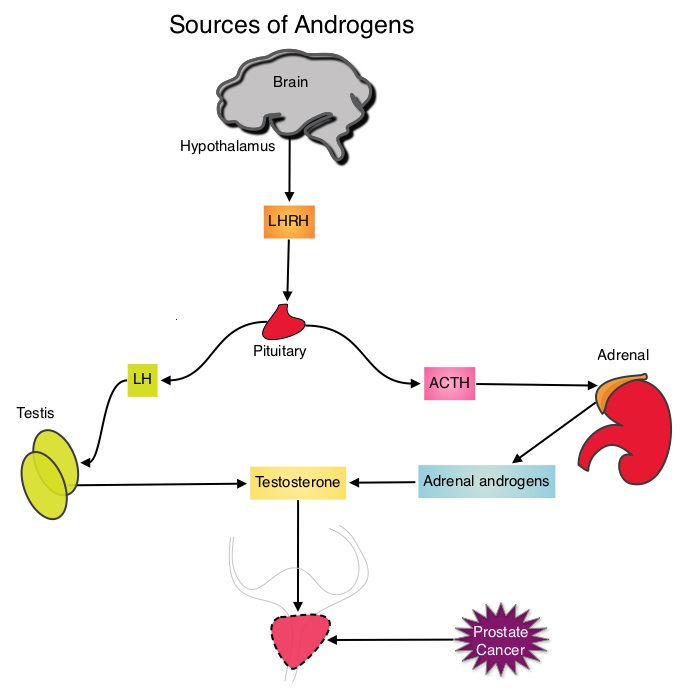 This is accomplished by either surgical castration (bilateral orchiectomy) or medical castration using LHRH (GnRH- Gonadotropin-Releasing Hormone) agonists given along with 2 weeks of first generation anti-androgen agents such as EULEXIN® (Flutamide), CASODEX® (Bicalutamide) or NILANDRON® (Nilutamide), with the anti-androgen agents given to prevent testosterone flare. This large intergroup trial which was developed by the NCIC Clinical Trials Group in collaboration with the Medical Research Council and the National Cancer Institute US Cancer Therapy Evaluation Program, evaluated the benefits of adding Radiation Therapy (RT) to ADT, when compared to ADT alone, in patients with locally advanced prostate cancer. In this study, 1205 patients were randomly assigned to receive either ADT alone (N=602) or ADT plus RT (N=603). Eligible patients included those with T1-2 disease with either Prostate Specific Antigen (PSA) of more than 40 μg/L or PSA of 20-40 μg/L plus Gleason score of 8-10 or patients with T3-4, N0/NX, M0 prostate cancer. ADT consisted of either bilateral orchiectomy or LHRH agonists (plus 2 weeks of oral anti-androgen therapy to prevent testosterone flare), based on patient and physician preference, and ADT was continued for life. RT consisted of a dose of 64-69 Gy given in 35-39 fractions to the prostate gland and pelvis or prostate gland alone. The median age was 70 years and the median follow up was 8 years. Eighty seven percent of patients had T3-4 disease, 63% of patients had a PSA more than 20 μg/L and 18% had a Gleason score of more than 8. The Primary Endpoint was Overall Survival (OS), defined as the time from randomization to death from any cause. Secondary Endpoints included Time To Progression (TTP), improvement in Disease Specific Survival, quality of life and toxicity. The authors had previously reported the interim analysis findings of this intergroup trial and they noted that the addition of RT to ADT significantly improved overall survival, at a median follow up of 6 years (HR= 0.77; P=0.033). In this final analysis, at a median follow up of 8 years, the interim analysis findings were confirmed and the patients assigned to ADT plus RT had significantly improved Overall Survival compared to those who received ADT alone (HR=0.70; P<0.001), with a 30% reduction in the risk of death. Disease Specific Survival was also superior with ADT plus RT compared to ADT alone, with a 54% reduction in deaths from prostate cancer (HR=0.46; P <0 .001). There was a higher incidence of grade 1 and 2 bowel toxicities in patients who received ADT plus RT, but grade 3 bowel toxicities were rare and short term. The authors concluded that this long term follow up data suggests that the addition of Radiation Therapy to Androgen Deprivation Therapy significantly prolongs Overall and Disease Specific Survival, in patients with locally advanced prostate cancer. Final Report of the Intergroup Randomized Study of Combined Androgen-Deprivation Therapy Plus Radiotherapy Versus Androgen-Deprivation Therapy Alone in Locally Advanced Prostate Cancer. Mason MD, Parulekar WR, Sydes MR, et al. J Clin Oncol 2015; 33:2143-2150
This is accomplished by either surgical castration (bilateral orchiectomy) or medical castration using LHRH (GnRH- Gonadotropin-Releasing Hormone) agonists given along with 2 weeks of first generation anti-androgen agents such as EULEXIN® (Flutamide), CASODEX® (Bicalutamide) or NILANDRON® (Nilutamide), with the anti-androgen agents given to prevent testosterone flare. This large intergroup trial which was developed by the NCIC Clinical Trials Group in collaboration with the Medical Research Council and the National Cancer Institute US Cancer Therapy Evaluation Program, evaluated the benefits of adding Radiation Therapy (RT) to ADT, when compared to ADT alone, in patients with locally advanced prostate cancer. In this study, 1205 patients were randomly assigned to receive either ADT alone (N=602) or ADT plus RT (N=603). Eligible patients included those with T1-2 disease with either Prostate Specific Antigen (PSA) of more than 40 μg/L or PSA of 20-40 μg/L plus Gleason score of 8-10 or patients with T3-4, N0/NX, M0 prostate cancer. ADT consisted of either bilateral orchiectomy or LHRH agonists (plus 2 weeks of oral anti-androgen therapy to prevent testosterone flare), based on patient and physician preference, and ADT was continued for life. RT consisted of a dose of 64-69 Gy given in 35-39 fractions to the prostate gland and pelvis or prostate gland alone. The median age was 70 years and the median follow up was 8 years. Eighty seven percent of patients had T3-4 disease, 63% of patients had a PSA more than 20 μg/L and 18% had a Gleason score of more than 8. The Primary Endpoint was Overall Survival (OS), defined as the time from randomization to death from any cause. Secondary Endpoints included Time To Progression (TTP), improvement in Disease Specific Survival, quality of life and toxicity. The authors had previously reported the interim analysis findings of this intergroup trial and they noted that the addition of RT to ADT significantly improved overall survival, at a median follow up of 6 years (HR= 0.77; P=0.033). In this final analysis, at a median follow up of 8 years, the interim analysis findings were confirmed and the patients assigned to ADT plus RT had significantly improved Overall Survival compared to those who received ADT alone (HR=0.70; P<0.001), with a 30% reduction in the risk of death. Disease Specific Survival was also superior with ADT plus RT compared to ADT alone, with a 54% reduction in deaths from prostate cancer (HR=0.46; P <0 .001). There was a higher incidence of grade 1 and 2 bowel toxicities in patients who received ADT plus RT, but grade 3 bowel toxicities were rare and short term. The authors concluded that this long term follow up data suggests that the addition of Radiation Therapy to Androgen Deprivation Therapy significantly prolongs Overall and Disease Specific Survival, in patients with locally advanced prostate cancer. Final Report of the Intergroup Randomized Study of Combined Androgen-Deprivation Therapy Plus Radiotherapy Versus Androgen-Deprivation Therapy Alone in Locally Advanced Prostate Cancer. Mason MD, Parulekar WR, Sydes MR, et al. J Clin Oncol 2015; 33:2143-2150
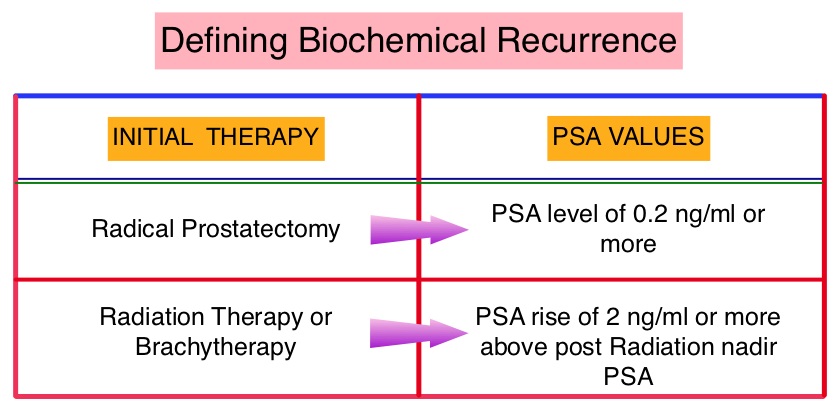
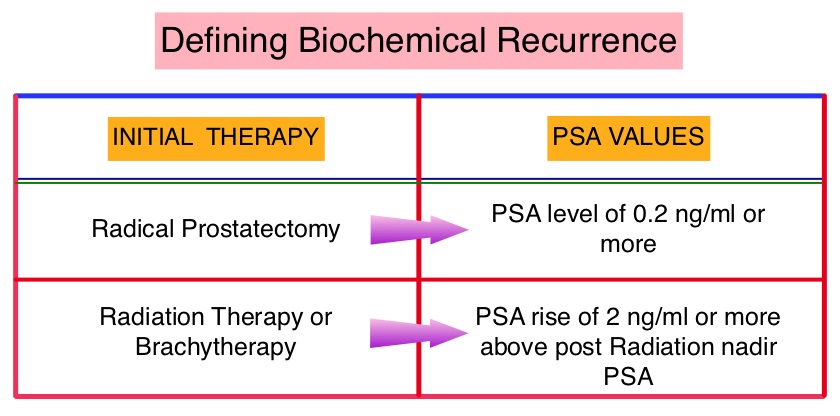 The American Urological Association suggested that a PSA of 0.2 ng/mL or higher after Radical Prostatectomy, defines PSA failure or relapse. A PSA rise of 2 ng/ml or more above post Radiation Therapy nadir is considered PSA failure or relapse. Approximately 35% of the patients with prostate cancer will experience PSA only relapse within 10 years of their primary treatment and a third of these patients will develop documented metastatic disease within 8 years following PSA only relapse. The development and progression of prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) has therefore been the cornerstone of treatment of advanced prostate cancer and is the first treatment intervention for hormone sensitive prostate cancer. The appropriate time (immediate versus delayed) to start Androgen Deprivation Therapy (ADT) in patients with prostate cancer with rising Prostate-Specific Antigen (PSA), as the only sign of relapse, has remained unclear. This has been partly due to lack of patient accruals and patient reluctance to be randomized, in these clinical trials.
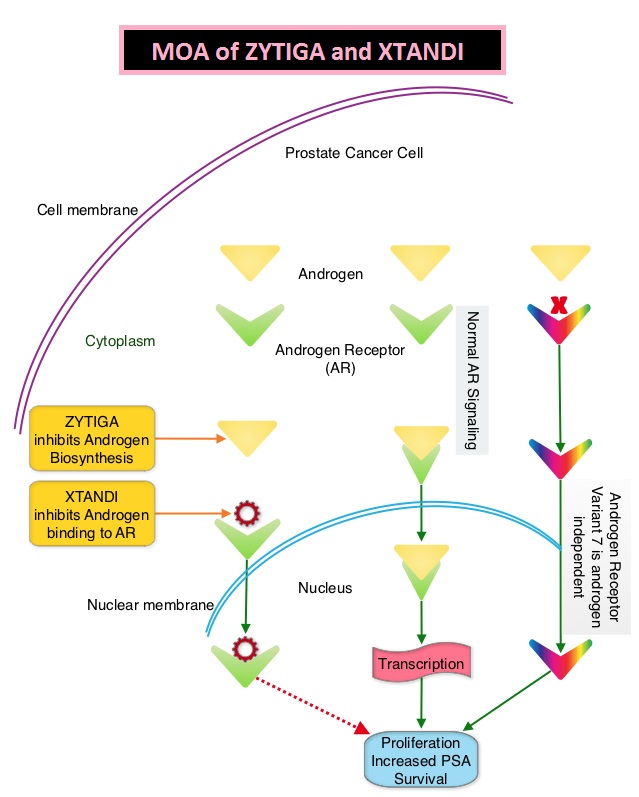
The American Urological Association suggested that a PSA of 0.2 ng/mL or higher after Radical Prostatectomy, defines PSA failure or relapse. A PSA rise of 2 ng/ml or more above post Radiation Therapy nadir is considered PSA failure or relapse. Approximately 35% of the patients with prostate cancer will experience PSA only relapse within 10 years of their primary treatment and a third of these patients will develop documented metastatic disease within 8 years following PSA only relapse. The development and progression of prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) has therefore been the cornerstone of treatment of advanced prostate cancer and is the first treatment intervention for hormone sensitive prostate cancer. The appropriate time (immediate versus delayed) to start Androgen Deprivation Therapy (ADT) in patients with prostate cancer with rising Prostate-Specific Antigen (PSA), as the only sign of relapse, has remained unclear. This has been partly due to lack of patient accruals and patient reluctance to be randomized, in these clinical trials.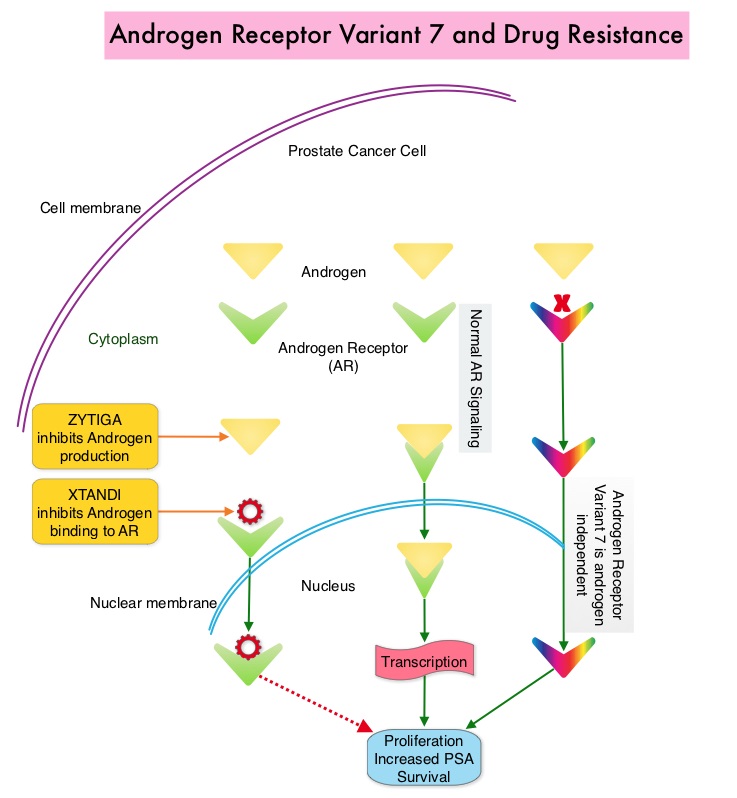 Both these agents have been shown to improve survival in metastatic CRPC. ZYTIGA® inhibits CYP 17A1 enzyme and depletes adrenal and intratumoral androgens, thereby impairing AR signaling. XTANDI® competes with Testosterone and Dihydrotestosterone and avidly binds to the Androgen Receptor, thereby inhibiting AR signaling and in addition inhibits translocation of the AR into the nucleus and thus inhibits the transcriptional activities of the AR. About 20-40% of the patients do not respond to these newer agents and even those who respond will invariably develop resistance to these drugs. This again has been attributed to persistent AR signaling by variant forms of Androgen Receptor, generated through somatic mutation or aberrant RNA splicing. Androgen Receptor Variant AR-V7 can be detected in the CTCs (Circulating Tumor Cells). AR-V7 does not have the domain to bind androgens and may be associated with resistance to XTANDI®. Further AR-V7 is constitutively active and can independently activate transcription factors and therefore is not effected by androgen depleting agents including ZYTIGA®. With this background, the authors hypothesized that detection of Androgen Receptor variant AR-V7 in circulating tumor cells from men with metastatic prostate cancer would be associated with resistance to both ZYTIGA® and XTANDI®. In a previously published prospective study, data involving 62 patients showed that detection of AR-V7 in Circulating Tumor Cells (CTCs) in men with mCRPC was indeed associated with primary resistance to both ZYTIGA® and XTANDI®. AR-V7–positive patients had inferior overall survival with both XTANDI® (HR = 6.9; P =0.002) and ZYTIGA® (HR = 12.7; P =0.006). AR-V7 was therefore shown to have a prognostic value for outcomes in mCRPC with ZYTIGA® and XTANDI®. In this present publication, the authors studied to determine if AR-V7-positive patients would retain sensitivity to Taxane chemotherapy. The researchers in this small prospective study enrolled 37 patients with metastatic CRPC who were starting Taxane chemotherapy with Cabazitaxel (JEVTANA®) or Docetaxel (TAXOTERE®). Presence or lack of AR-V7 in circulating tumor cells (CTCs), was determined by the qRT-PCR assay. Of the enrolled patients, 46% had detectable AR-V7 in CTCs. The primary endpoint was associations between AR-V7 status and PSA response rates and secondary endpoints included Progression Free Survival (PFS). They noted that the PSA responses were achieved in both AR-V7- positive and AR-V7-negative men and the difference was non-significant (41% versus 65%, P=0.19). Likewise there was no significant difference in the median PFS in AR-V7-positive and AR-V7-negative men (5.1 versus 6.9 months (HR= 2.65; P=0.11). The researchers then combined the data from their previously published study with 62 patients and they noted that, in AR-V7-positive men, PSA responses were higher in Taxane treated versus ZYTIGA®/XTANDI® treated men (41% versus 0%, P<0.001) and PFS were longer in the Taxane treated men as well (HR for PFS = 0.21, P=0.003). The outcomes however did not differ by treatment type in AR-V7-negative men and were comparable. The authors concluded that detection of AR-V7 in CTCs from men with mCRPC is not associated with primary resistance to Taxane chemotherapy, and such patients may retain sensitivity to Taxanes. In AR-V7-positive men however, Taxanes appear to be more efficacious than ZYTIGA® or XTANDI®. AR-V7 once available commercially, may become a biomarker for treatment selection, in metastatic Castrate Resistant Prostate Cancer. AR splice variant 7 (AR-V7) and response to taxanes in men with metastatic castration-resistant prostate cancer (mCRPC). Antonarakis ES, Lu C, Chen Y, et al. J Clin Oncol 33, 2015 (suppl 7; abstr 138)
Both these agents have been shown to improve survival in metastatic CRPC. ZYTIGA® inhibits CYP 17A1 enzyme and depletes adrenal and intratumoral androgens, thereby impairing AR signaling. XTANDI® competes with Testosterone and Dihydrotestosterone and avidly binds to the Androgen Receptor, thereby inhibiting AR signaling and in addition inhibits translocation of the AR into the nucleus and thus inhibits the transcriptional activities of the AR. About 20-40% of the patients do not respond to these newer agents and even those who respond will invariably develop resistance to these drugs. This again has been attributed to persistent AR signaling by variant forms of Androgen Receptor, generated through somatic mutation or aberrant RNA splicing. Androgen Receptor Variant AR-V7 can be detected in the CTCs (Circulating Tumor Cells). AR-V7 does not have the domain to bind androgens and may be associated with resistance to XTANDI®. Further AR-V7 is constitutively active and can independently activate transcription factors and therefore is not effected by androgen depleting agents including ZYTIGA®. With this background, the authors hypothesized that detection of Androgen Receptor variant AR-V7 in circulating tumor cells from men with metastatic prostate cancer would be associated with resistance to both ZYTIGA® and XTANDI®. In a previously published prospective study, data involving 62 patients showed that detection of AR-V7 in Circulating Tumor Cells (CTCs) in men with mCRPC was indeed associated with primary resistance to both ZYTIGA® and XTANDI®. AR-V7–positive patients had inferior overall survival with both XTANDI® (HR = 6.9; P =0.002) and ZYTIGA® (HR = 12.7; P =0.006). AR-V7 was therefore shown to have a prognostic value for outcomes in mCRPC with ZYTIGA® and XTANDI®. In this present publication, the authors studied to determine if AR-V7-positive patients would retain sensitivity to Taxane chemotherapy. The researchers in this small prospective study enrolled 37 patients with metastatic CRPC who were starting Taxane chemotherapy with Cabazitaxel (JEVTANA®) or Docetaxel (TAXOTERE®). Presence or lack of AR-V7 in circulating tumor cells (CTCs), was determined by the qRT-PCR assay. Of the enrolled patients, 46% had detectable AR-V7 in CTCs. The primary endpoint was associations between AR-V7 status and PSA response rates and secondary endpoints included Progression Free Survival (PFS). They noted that the PSA responses were achieved in both AR-V7- positive and AR-V7-negative men and the difference was non-significant (41% versus 65%, P=0.19). Likewise there was no significant difference in the median PFS in AR-V7-positive and AR-V7-negative men (5.1 versus 6.9 months (HR= 2.65; P=0.11). The researchers then combined the data from their previously published study with 62 patients and they noted that, in AR-V7-positive men, PSA responses were higher in Taxane treated versus ZYTIGA®/XTANDI® treated men (41% versus 0%, P<0.001) and PFS were longer in the Taxane treated men as well (HR for PFS = 0.21, P=0.003). The outcomes however did not differ by treatment type in AR-V7-negative men and were comparable. The authors concluded that detection of AR-V7 in CTCs from men with mCRPC is not associated with primary resistance to Taxane chemotherapy, and such patients may retain sensitivity to Taxanes. In AR-V7-positive men however, Taxanes appear to be more efficacious than ZYTIGA® or XTANDI®. AR-V7 once available commercially, may become a biomarker for treatment selection, in metastatic Castrate Resistant Prostate Cancer. AR splice variant 7 (AR-V7) and response to taxanes in men with metastatic castration-resistant prostate cancer (mCRPC). Antonarakis ES, Lu C, Chen Y, et al. J Clin Oncol 33, 2015 (suppl 7; abstr 138)
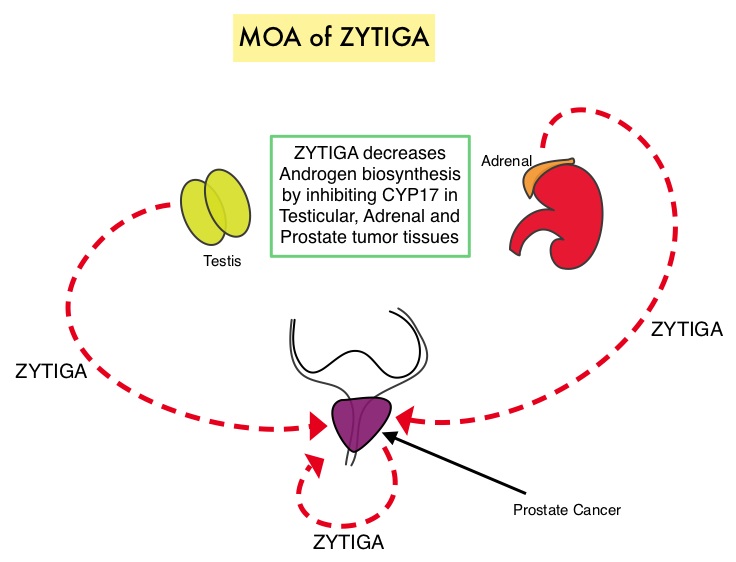 Abiraterone acetate (ZYTIGA®) is a novel, targeted, oral androgen biosynthesis inhibitor that decreases androgen production in the adrenal glands, testes and prostate cancer cells by inhibiting a steroidal enzyme CYP17A. COU-AA-302 trial is a placebo controlled, double-blind, randomized, phase III study and at the interim analyses showed that ZYTIGA® plus Prednisone significantly improved radiographic Progression Free Survival compared with placebo plus Prednisone, in men with chemotherapy-naive CRPC. The authors in this publication provided additional data on the pre-specified final analysis of the trial, which included the effect of ZYTIGA® plus Prednisone on Overall Survival, time to opiate use, and use of other subsequent therapies. In this study which included 1088 chemotherapy-naïve, asymptomatic or mildly symptomatic CRPC patients, 546 patients received ZYTIGA® 1000 mg PO plus Prednisone 5 mg PO twice daily and 542 patients received placebo plus Prednisone. The co-primary endpoints were radiographic Progression Free Survival and Overall Survival. In the final analysis, at a median follow up of 49•2 months, the median Overall Survival was 34.7 months in the ZYTIGA® group vs 30.3 months in the placebo control group (HR = 0.81, P = 0.0033). This benefit was seen across all prespecified subgroups, as well as adjusting for crossover from placebo to ZYTIGA® (HR = 0.79, P = 0.0013). The median time to opiate use for cancer-related pain was significantly prolonged in the ZYTIGA® group compared to the placebo group (33.4 vs 23.4 months, HR = 0.72, P < 0.0001). The most common grade 3 or 4 adverse events of special interest in the ZYTIGA® vs placebo group were cardiac disorders (8% vs 4%), increased ALT (6% vs < 1%), and hypertension (5% vs 3%). The authors concluded that with a median follow up of more than 4 years, treatment with ZYTIGA® in patients with chemotherapy-naive metastatic CRPC, significantly improved Overall Survival compared with Prednisone alone, with favorable toxicities. Ryan CJ, Smith MR, Fizazi K, et al. for the COU-AA-302 Investigators .The Lancet Oncology 2015; 16:152-160
Abiraterone acetate (ZYTIGA®) is a novel, targeted, oral androgen biosynthesis inhibitor that decreases androgen production in the adrenal glands, testes and prostate cancer cells by inhibiting a steroidal enzyme CYP17A. COU-AA-302 trial is a placebo controlled, double-blind, randomized, phase III study and at the interim analyses showed that ZYTIGA® plus Prednisone significantly improved radiographic Progression Free Survival compared with placebo plus Prednisone, in men with chemotherapy-naive CRPC. The authors in this publication provided additional data on the pre-specified final analysis of the trial, which included the effect of ZYTIGA® plus Prednisone on Overall Survival, time to opiate use, and use of other subsequent therapies. In this study which included 1088 chemotherapy-naïve, asymptomatic or mildly symptomatic CRPC patients, 546 patients received ZYTIGA® 1000 mg PO plus Prednisone 5 mg PO twice daily and 542 patients received placebo plus Prednisone. The co-primary endpoints were radiographic Progression Free Survival and Overall Survival. In the final analysis, at a median follow up of 49•2 months, the median Overall Survival was 34.7 months in the ZYTIGA® group vs 30.3 months in the placebo control group (HR = 0.81, P = 0.0033). This benefit was seen across all prespecified subgroups, as well as adjusting for crossover from placebo to ZYTIGA® (HR = 0.79, P = 0.0013). The median time to opiate use for cancer-related pain was significantly prolonged in the ZYTIGA® group compared to the placebo group (33.4 vs 23.4 months, HR = 0.72, P < 0.0001). The most common grade 3 or 4 adverse events of special interest in the ZYTIGA® vs placebo group were cardiac disorders (8% vs 4%), increased ALT (6% vs < 1%), and hypertension (5% vs 3%). The authors concluded that with a median follow up of more than 4 years, treatment with ZYTIGA® in patients with chemotherapy-naive metastatic CRPC, significantly improved Overall Survival compared with Prednisone alone, with favorable toxicities. Ryan CJ, Smith MR, Fizazi K, et al. for the COU-AA-302 Investigators .The Lancet Oncology 2015; 16:152-160