
The FDA on February 7, 2018, approved ZYTIGA® (Abiraterone acetate) in combination with Prednisone for metastatic high-risk Castration Sensitive Prostate Cancer (CSPC). The FDA initially approved ZYTIGA® with prednisone in 2011 for patients with metastatic Castration Resistant Prostate Cancer (CRPC), who had received prior chemotherapy, and the FDA expanded the indication in 2012, for patients with chemo naïve metastatic CRPC. The addition of ZYTIGA® along with Prednisone, to Androgen Deprivation Therapy, significantly increased Overall Survival and radiographic Progression Free Survival, in men with newly diagnosed, metastatic, Castration Sensitive Prostate Cancer. The new approval will change the treatment landscape for patients with metastatic CSPC.
Tag: Prostate Cancer
ERLEADA® (Apalutamide)
The FDA on February 14, 2018 approved ERLEADA® for patients with Non-Metastatic Castration Resistant Prostate Cancer (NM-CRPC). ERLEADA® is a product of Janssen Biotech Inc.
FDA Approves ZYTIGA® for High-Risk Metastatic Castration-Sensitive Prostate Cancer
SUMMARY: The FDA on February 7, 2018, approved ZYTIGA® (Abiraterone acetate) in combination with Prednisone for metastatic high-risk Castration Sensitive Prostate Cancer (CSPC). The FDA initially approved ZYTIGA® with prednisone in 2011 for patients with metastatic Castration Resistant Prostate Cancer (CRPC), who had received prior chemotherapy, and the FDA expanded the indication in 2012, for patients with chemo naïve metastatic CRPC. Prostate cancer is the most common cancer in American men with the exclusion of skin cancer and 1 in 9 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, about 164,690 new cases of Prostate cancer will be diagnosed in 2018 and 29,430 men will die of the disease. The development and progression of prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) has therefore been the cornerstone of treatment of advanced prostate cancer and is the first treatment intervention for Castration Sensitive Prostate Cancer (CSPC). Androgen Deprivation Therapies have included bilateral orchiectomy or Gonadotropin Releasing Hormone (GnRH) analogues, with or without first generation androgen receptor inhibitors such as CASODEX®: (Bicalutamide), NILANDRON® (Nilutamide) and EULEXIN® (Flutamide). The median duration of response is approximately 1 year and majority of these patients progress to Castration Resistant Prostate Cancer (CRPC). The mechanism of resistance to Androgen Deprivation Therapy (ADT) include reactivation of Androgen Receptor signaling through persistent adrenal androgen production, modification of the biologic characteristics of Androgen Receptors, intratumoral testosterone production and parallel steroidogenic pathways.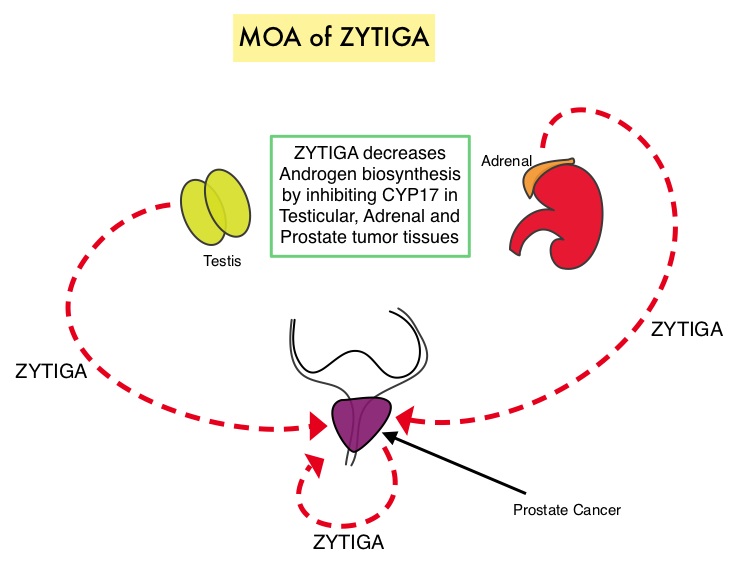
Two previously published trials, STAMPEDE and CHAARTED have shown that the addition of TAXOTERE® (Docetaxel) to Androgen Deprivaton Therapy as first line systemic therapy, significantly improved Overall Survival, among men with locally advanced or metastatic Castration Sensitive Prostate Cancer. This is presently the standard of care for appropriate patients with prostate cancer, who had not received prior hormone therapy. The barriers to chemo-hormonal therapy with TAXOTERE® include advanced patient age, poor Performance Status, comorbidities, patient preferences, as well as potential life threatening toxicities associated with TAXOTERE®.
ZYTIGA® is a selective, irreversible inhibitor of CYP 17A1 enzyme and decreases androgen biosynthesis in the testes, adrenal glands, and prostate-tumor tissue. Combining a CYP17A1 inhibitor such as ZYTIGA® with Androgen Deprivation Therapy is a more effective way of androgen depletion than with Orchiectomy or GnRH analogues alone. ZYTIGA® in combination with prednisone has been shown to significantly increase Overall Survival in patients with metastatic CRPC who had not received chemotherapy as well as those who had received previous chemotherapy with TAXOTERE®. Further, ZYTIGA® along with Prednisone has been shown to reduce tumor burden in men with high-risk, localized prostate cancer, receiving neoadjuvant therapy.
The current FDA approval was based on LATITUDE, a multinational, randomized, double-blind, placebo-controlled, phase III trial, in which the authors evaluated the clinical benefit of adding ZYTIGA® along with Prednisone to Androgen Deprivation Therapy (ADT), as compared with Androgen Deprivation Therapy and placebo, in patients with newly diagnosed, metastatic Castration Sensitive Prostate Cancer. In this study, 1199 newly diagnosed patients with high-risk metastatic prostate cancer were randomized to receive either ZYTIGA® along with Prednisone and ADT (N=597) or placebo and ADT (N=602). ZYTIGA® was administered at 1000 mg and Prednisone at 5 mg, both drugs given orally daily, and ADT consisted of a GnRH (Gonadotropin Releasing Hormone) analog. Eligible patients should not have received prior ADT and had at least 2 of 3 risk factors which included Gleason score 8 or greater, measurable visceral metastases or 3 or more bone lesions, all of which are associated with poor survival. The median age was 68 years and 98% of the enrolled patients had a Gleason score of 8 or more and had 3 or more sites of bone metastases. Both treatment groups were well balanced. The two Primary end points were Overall Survival and radiographic Progression Free Survival.
After a median follow-up of 30.4 months, at a planned interim analysis, the median Overall Survival was significantly longer in the ZYTIGA® group compared to the placebo group (Not Reached versus 34.7 months, HR=0.62; P<0.001). This meant a 38% reduction in the risk of death with the addition of ZYTIGA® and Prednisone to ADT compared with placebo and ADT. The median radiographic Progression Free Survival was 33 months in the ZYTIGA® group and 14.8 months in the placebo group (HR=0.47; P<0.001). This meant a 53% reduction in the risk of progression or death, with the addition of ZYTIGA® and Prednisone to ADT, compared with placebo and ADT. Further in the ZYTIGA® group, significantly better outcomes were observed in all Secondary end points and they included Time to pain progression, Time to next subsequent therapy for prostate cancer, Time to initiation of chemotherapy, and PSA progression (P<0.001 for all comparisons), along with Time to next symptomatic skeletal events (P=0.009). Based on these promising findings, the Independent Data and Safety Monitoring Committee recommended that the trial be unblinded and crossover be allowed for patients in the placebo group to receive ZYTIGA® and Prednisone along with ADT.
The authors concluded that the addition of ZYTIGA® along with Prednisone, to Androgen Deprivation Therapy, significantly increased Overall Survival and radiographic Progression Free Survival, in men with newly diagnosed, metastatic, Castration Sensitive Prostate Cancer. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. Fizazi K, Tran N, Fein L, et al. for the LATITUDE Investigators. N Engl J Med 2017; 377:352-360
ZYTIGA® (Abiraterone acetate)
The FDA on February 7, 2018 approved ZYTIGA® tablets in combination with Prednisone for metastatic high-risk Castration-Sensitive Prostate Cancer (CSPC). The FDA initially approved ZYTIGA® with prednisone in 2011 for patients with metastatic Castration-Resistant Prostate Cancer (CRPC), who had received prior chemotherapy, and expanded the indication in 2012 for patients with metastatic CRPC. ZYTIGA® is a product of Janssen Biotech Inc.
JEVTANA® (Cabazitaxel)
The FDA on September 14, 2017 approved a lower dose of JEVTANA® (20 mg/m2 every 3 weeks) in combination with Prednisone for the treatment of patients with metastatic Castration-Resistant Prostate Cancer, previously treated with a Docetaxel-containing treatment regimen. JEVTANA® (25 mg/m2 every 3 weeks) was approved for this indication in 2010. JEVTANA® is a product of Sanofi-Aventis.
Brachytherapy for Patients With Prostate Cancer American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update Summary
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer and 1 in 7 men will be diagnosed with Prostate cancer during their lifetime. It is estimated that in the United States, about 161,360 new cases of Prostate cancer will be diagnosed in 2017 and 26,730 men will die of the disease. Brachytherapy for prostate cancer is a type of Internal radiation treatment in which radioactive material sealed inside a seed, pellet, wire, or capsule is implanted in the prostate gland using a needle or catheter. Brachytherapy allows the delivery of higher doses of radiation to the intended site, compared with the conventional form of radiation therapy (External Beam Radiation Therapy).
Types of Brachytherapy
1) Low-dose rate (LDR) implants that stay in the prostate gland for 1 to 7 days and then are taken out.
2) High-dose rate (HDR) implants that stay in the prostate gland for a few minutes at a time and are then taken out.
3) Permanent implants that stay in the prostate gland and are not removed.
Prostate Cancer Risk Categories
Very Low Risk: T1c, Gleason score 6 or less, PSA less than 10 ng/ml, Fewer than 3 prostate biopsy cores positive with 50% or less cancer in each core
Low Risk: T1-T2a, Gleason score 6 or less, PSA less than 10 ng/ml
Intermediate Risk: T2b-T2c and/or Gleason score =7 and/or PSA 10-20 ng/ml
High Risk: T3a or Gleason score 8-10 or PSA more than 20 ng/ml
Very High Risk: T3b-T4
With the gathering of new evidence from randomized trials since the original publication in 2013, a guidelines update became necessary. The scope of this guideline covers Brachytherapy boost and monotherapy. The relevant evidence was evaluated for inclusion in this updated clinical practice guideline after a systematic review of the literature and five randomized controlled trials provided the evidence for this update.
Guideline Questions
1) In patients with newly diagnosed Prostate cancer, what is the efficacy of Brachytherapy alone for clinical outcomes compared with External Beam Radiation Therapy (EBRT) alone, or Radical Prostatectomy (RP) alone?
2) In patients with newly diagnosed Prostate cancer, what is the efficacy of Brachytherapy combined with EBRT for clinical outcomes compared with Brachytherapy alone, EBRT alone, or RP alone?
3) Among the isotopes used for low-dose-rate (LDR) Brachytherapy (eg, Iodine-125 [125I], Palladium-103 [103Pd], and Cesium-131 [131Cs]), which isotope maximizes clinical outcomes when used in patients with newly diagnosed Prostate cancer?
Updated recommendations
1) For patients with low-risk Prostate cancer who require or choose active treatment, LDR brachytherapy alone, EBRT alone, or RP should be offered to those who are eligible.
2) For patients with intermediate-risk Prostate cancer choosing EBRT with or without Androgen Deprivation Therapy (ADT), Brachytherapy boost (LDR or high–dose rate [HDR]) should be offered to eligible patients.
3) For low-intermediate risk Prostate cancer (Gleason 7, PSA 10 ng/mL or Gleason 6, PSA 10 to 20 ng/mL) LDR Brachytherapy alone may be offered as monotherapy.
4) For patients with high-risk Prostate cancer receiving EBRT and ADT, Brachytherapy boost (LDR or HDR) should be offered to eligible patients.
5)125I and 103Pd are each reasonable isotope options for patients receiving LDR Brachytherapy; no recommendation can be made for or against using 131Cs or HDR monotherapy.
6) Patients should be encouraged to participate in clinical trials
Qualifying Statements
1) Patients should be counseled about all of their management options (surgery, EBRT, Brachytherapy, or active surveillance, as applicable) in a balanced, objective manner, preferably by practitioners from multiple disciplines.
2) Recommendations for patients with low-risk disease are unchanged from the initial guideline because no new data from randomized studies informing this question have been presented or published since 2013.
3) Patients ineligible for Brachytherapy may include those with moderate to severe baseline urinary symptoms, large prostate volume, or prior transurethral resection of the prostate, those who are medically unfit, and those with contraindications to radiation treatment.
4) ADT may be given in neoadjuvant, concurrent, and/or adjuvant settings at the physician’s discretion. Note that neoadjuvant ADT may cytoreduce the prostate volume sufficiently to allow Brachytherapy.
5) There may be increased genitourinary toxicity with Brachytherapy compared with use of EBRT alone.
6) Brachytherapy should be performed at a center that has strict quality assurance standards.
7) It cannot be determined whether there is an overall or cause-specific survival advantage for Brachytherapy compared with EBRT alone because none of the trials were designed or powered to detect a meaningful difference in survival outcomes.
Brachytherapy for Patients With Prostate Cancer: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update. Chin J, Rumble RB, Kollmeier M, et al. Journal of Clinical Oncology 2017;35:1737-1743.
Late Breaking Abstract – ASCO 2017 Adding ZYTIGA® to Androgen Deprivation Therapy Improves Overall Survival in Newly Diagnosed Advanced Prostate Cancer
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer and 1 in 7 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, about 161,360 new cases of Prostate cancer will be diagnosed in 2017 and 26,730 men will die of the disease. The development and progression of prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) has therefore been the cornerstone of treatment of advanced prostate cancer and is the first treatment intervention for hormone sensitive prostate cancer. For patients with Castrate Resistant Prostate Carcinoma (CRPC), several agents have been proven to improve Overall Survival and they include, TAXOTERE® (Docetaxel), JEVTANA® (Cabazitaxel), ZYTIGA® (Abiraterone acetate), XTANDI® (Enzalutamide), XOFIGO® (Radium-223), and PROVENGE® (Sipuleucel-T).
The Systemic Therapy in Advancing or Metastatic Prostate Cancer: Evaluation of Drug Efficacy (STAMPEDE) trial is an ongoing study and uses a novel multiarm, multistage (MAMS) platform design, to test whether the addition of further treatments to ADT improves Overall Survival, when used in first-line setting, for patients with hormone sensitive, locally advanced or metastatic prostate cancer. This group previously reported that there was a significantly improved Overall Survival with the addition of TAXOTERE® to initial ADT. This is presently the standard of care for appropriate patients with prostate cancer, who had not received prior hormone therapy. The barriers to chemo-hormonal therapy with TAXOTERE® include advanced patient age, poor Performance Status, comorbidities, patient preferences, as well as potential life threatening toxicities associated with TAXOTERE®.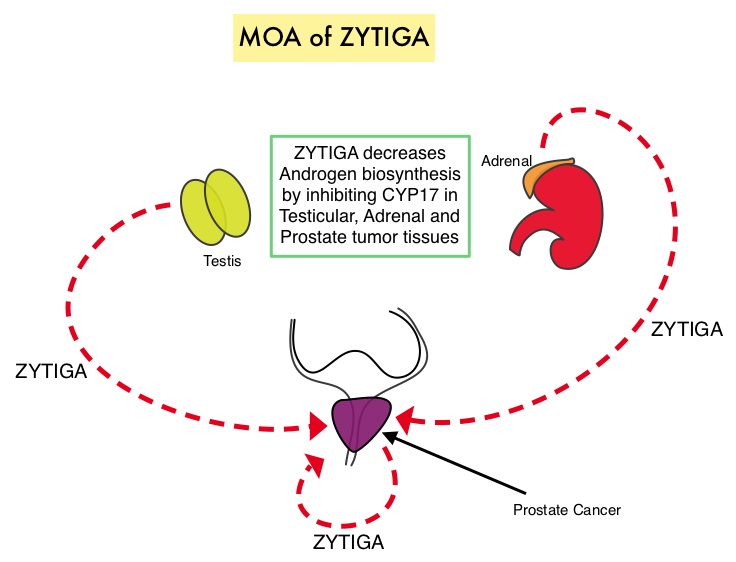
ZYTIGA® is a selective, irreversible inhibitor of CYP 17A1 enzyme and decreases androgen biosynthesis in the testes, adrenal glands, and prostate-tumor tissue. Combining a CYP17A1 inhibitor such as ZYTIGA® with Androgen Deprivation Therapy is a more effective way of androgen depletion than with Orchiectomy or GnRH analogues alone. In this analysis, the STAMPEDE trial evaluated Overall Survival outcomes, with the earlier use of ZYTIGA®, in men with high risk, hormone sensitive prostate cancer, who were initiating long-term Androgen Deprivation Therapy.
A total of 1917 patients were randomly assigned patients in a 1:1 ratio to receive Androgen Deprivation Therapy (ADT) alone (N=957) or ADT plus ZYTIGA® (N=960), administered at 1000 mg PO daily and prednisolone 5 mg PO daily (combination therapy). ADT was given for at least 2 years. Eligible patients had prostate cancer that was newly diagnosed and metastatic, node-positive, or high-risk locally advanced disease or prostate cancer that was previously treated with radical surgery or radiotherapy and was now relapsing with high-risk features. Patients with locally advanced disease could also receive radiation therapy in addition to ADT. Radiotherapy was mandated for patients with N0M0 disease and encouraged for those with stage N+M0 disease. The median age was 67 years, and the median PSA level was 53 ng/ml. Approximately 52% of the patients had metastatic disease, 20% had node-positive or node-indeterminate, non-metastatic disease, and 28% had node-negative, non-metastatic disease. Majority of the patients (95%) had newly diagnosed disease. The median follow up was 40 months.
There was a significant survival advantage with combination therapy with a 3-year Overall Survival of 83% with ADT plus ZYTIGA® compared with 76% with ADT alone group (HR=0.63; P<0.001). This meant a 37% reduction in the risk of death with the ZYTIGA® combination treatment. Further, the combination treatment reduced the risk of relapse by 71% (HR=0.29; P<0.001), and also reduced the risk of symptomatic skeletal events by 54% (HR=0.46; P<0.001), compared with ADT alone. Treatment overall was well tolerated.
It was concluded that ADT plus ZYTIGA® and prednisolone results in significantly higher rates of Overall Survival as well as Failure-Free Survival, compared with ADT alone, among men with hormone sensitive, locally advanced or metastatic prostate cancer. Interestingly, the LATITUDE trial showed similar findings in newly diagnosed, metastatic, hormone sensitive prostate cancer patients (June 4, 2017DOI: 10.1056/NEJMoa1704174). The results of both STAMPEDE and LATITUDE trials will very likely change practice patterns and will become the new standard of care for this patient group. Abiraterone for Prostate Cancer Not Previously Treated with Hormone Therapy. James ND, de Bono JS, Spears MR, et al. for the STAMPEDE Investigators. June 3, 2017DOI: 10.1056/NEJMoa1702900
Genomic Prostate Score® (GPS) can Predict Prostate Cancer Mortality and Risk of Metastases in Early Stage Prostate Cancer
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer and 1 in 7 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, about 161,360 new cases of Prostate cancer will be diagnosed in 2017 and 26,730 men will die of the disease. Traditionally, clinical risk assessment has been based on Tumor stage, Gleason score and PSA level, in patients who had Radical Prostatectomy for Prostate cancer. However, new validated biomarkers can improve risk stratification for men with Prostate cancer.
The Oncotype DX® Prostate Cancer Assay is a multi-gene RT-PCR expression assay that was developed for use with Fixed Paraffin-Embedded (FPE) Prostate needle biopsy specimens. This 17 gene assay measures expression of 12 cancer related genes representing four biological pathways with a known role in Prostate cancer development (androgen pathway, cellular organization, proliferation and stromal response), and 5 reference genes used to control for sources of pre-analytical and analytical variability. Combined together algorithmically, the Genomic Prostate Score (GPS, scale 0-100) is calculated, with a higher GPS score representing a more aggressive tumor phenotype. Genomic Prostate Score has been shown to predict unfavorable outcomes beyond conventional clinical and pathologic factors and has been validated as an independent predictor of adverse surgical pathology and BioChemical Recurence after Radical Prostatectomy, in men with low-risk and low-volume intermediate-risk Prostate cancer.
The authors conducted a large community based study, to confirm that Genomic Prostate Score (GPS) is a predictor of BioChemical Recurrence in all clinical risk groups (low, intermediate and high), in a large cohort of Prostate cancer patients, followed up at Kaiser Permanente medical groups in Northern California. A retrospective study was performed from the Kaiser Permanente clinical database of 6,184 Prostate cancer patients, between 1995- 2010, with NCCN very low, low, intermediate and high-risk disease, who were treated with Radical Prostatectomy. BioChemical Recurrence was defined as either 2 successive post-Radical Prostatectomy PSAs of 0.2 ng/mL or more, or initiation of salvage therapy after a rising PSA of 0.1 ng/mL or more. Genomic Prostate Score was derived from the archival biopsy tissue. The researchers were able to retrieve the biopsy tissue of 334 patients of whom 279 patients met all eligibility criteria and a valid GPS score was available in 259 (93%) patients.
It was noted that Genomic Prostate Score was strongly associated with BioChemical Recurrence after adjusting for PSA, clinical T stage and tumor Gleason Score (P=0.002). Genomic Prostate Score was a strong independent predictor of Prostate cancer-specific death and disease progression (metastases) at 10 years, across all NCCN clinical risk groups. Further, the association between GPS and BioChemical Recurrence was similar within the different racial groups.
It was concluded that for patients with Prostate cancer treated with Radical Prostatectomy, a higher Genomic Prostate Score was associated with BioChemical Recurrence, independent of other clinical factors. Genomic Prostate Score can hence improve risk stratification beyond clinical risk assessment, by predicting both near term adverse pathology and long term clinical outcomes Validation of a 17-Gene Genomic Prostate Score (GPS) as a predictor of biochemical recurrence (BCR) in men with prostate cancer treated with radical prostatectomy (RP) in a community setting. VanDenEeden SK, Zhang N, Quesenberry CP, et al. J Clin Oncol 35, 2017 (suppl 6S; abstract 41)
Sequencing Therapies in Metastatic Castrate Resistant Prostate Cancer
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer and 1 in 7 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, about 161,360 new cases of prostate cancer will be diagnosed in 2017 and 26,730 men will die of the disease. The development and progression of prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) has therefore been the cornerstone of treatment of advanced prostate cancer and is the first treatment intervention for hormone sensitive prostate cancer. Chemotherapy is usually considered for patients who progress on hormone therapy (Castrate Resistant Prostate Cancer-CRPC) and TAXOTERE® (Docetaxel) has been shown to improve Overall Survival (OS) of metastatic prostate cancer patients, who had progressed on Androgen Deprivation Therapy. Tumors in patients with CRPC are not androgen independent and continue to rely on Androgen Receptor signaling. Two oral Androgen Receptor Targeted Agents (ARTA) are presently available for metastatic CRPC. They include ZYTIGA® (Abiraterone) and XTANDI® (Enzalutamide). ZYTIGA® inhibits CYP 17A1 enzyme thus decreasing androgen biosynthesis and depletes adrenal and intratumoral androgens. XTANDI® competes with Testosterone and Dihydrotestosterone and avidly binds to the Androgen Receptor (AR), thereby inhibiting AR signaling and in addition inhibits translocation of the AR into the nucleus and thus inhibits the transcriptional activities of the AR. There is presently very little guidance with regards to the sequencing of these two oral agents.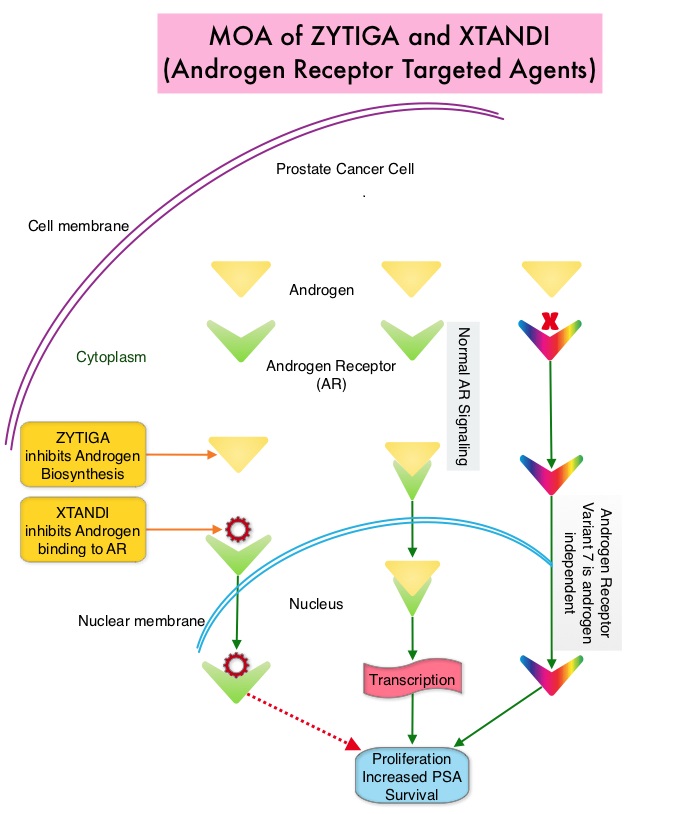
It has remained unclear when a patient should receive chemotherapy following progression on AR-targeted therapies. To determine the ideal second line therapy in this patient population, the authors conducted a retrospective study, to assess if second line chemotherapy was associated with improved outcomes, compared with second line alternative AR Targeted Agents, in patients with a very short duration of response to first line Androgen Receptor Targeted Agents, in the US community oncology setting.
Using Altos electronic medical records, the authors identified 345 patients with metastatic CRPC who did not respond to first-line AR Targeted Agents (ZYTIGA® or XTANDI®) who then went on to receive second-line TAXOTERE® – Docetaxel or JEVTANA® – Cabazitaxel (chemotherapy cohort, N=147), or an alternative AR Targeted Agent (ARTA cohort, N=198), from May 2011 to Oct 2014. Patients receiving chemotherapy as second-line treatment, compared to those receiving second-line ARTA, were younger (median age, 74 vs 79 years) and had several poor prognostic factors including a higher mean PSA, LDH and Alkaline Phosphatase, as well as lower mean hemoglobin and increased opioid use. Treatment outcomes were evaluated from start of second-line treatment and second-line chemotherapy was compared to second-line ARTA. The primary endpoints included Prostate Specific Antigen (PSA) response (50% or more reduction) and Overall Survival (OS).
It was noted that more patients in the chemotherapy group had a PSA response compared to the AR Targeted Agent group (P=0.005), and there was a non-statistically significant trend toward improved Overall Survival for second-line chemotherapy versus AR Targeted Agent (adjusted HR=0.81; P=0.15). Among patients with poor prognostic features, those in the chemotherapy cohort had significantly improved Overall Survival (adjusted HR=0.55; P=0.009) compared with those in the AR Targeted Agent cohort.
The authors concluded that patients who do not respond well to first-line Androgen Receptor Targeted Agent and have poor prognostic features, should not receive a second AR-targeted agent but instead receive second-line chemotherapy, as this may confer a survival benefit. Real-world outcomes in patients with metastatic castration-resistant prostate cancer receiving second-line chemotherapy vs alternative androgen receptor-target agents (ARTA) after lack of response to first-line ARTA in US community oncology practices. Oh WK, Cheng WY, Miao R, et al. J Clin Oncol. 2017;35 (suppl 6S; abstr 214).
Immediate Androgen Deprivation Therapy Confers Survival Benefit in Prostate Cancer Patients with Biochemical Recurrence
SUMMARY: Prostate cancer is the most common cancer in American men with the exclusion of skin cancer and 1 in 7 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, about 180,890 new cases of prostate cancer will be diagnosed in 2016 and over 26,000 men will die of the disease. The major source of PSA (Prostate Specific Antigen) is the prostate gland and the PSA levels are therefore undetectable within 6 weeks after Radical Prostatectomy. Similarly, following Radiation Therapy, there is a gradual decline in PSA before reaching a post treatment nadir. A detectable PSA level after Radical Prostatectomy, or a rising PSA level following Radiation Therapy, is considered PSA failure or biochemical recurrence. The American Urological Association suggested that a PSA of 0.2 ng/mL or higher after Radical Prostatectomy, defines PSA failure or relapse. A PSA rise 2 ng/ml or more above post Radiation Therapy nadir is considered PSA failure or relapse. Approximately 35% of the patients with prostate cancer will experience PSA only relapse within 10 years of their primary treatment and a third of these patients will develop documented metastatic disease within 8 years following PSA only relapse. Rising PSA is therefore a sign of recurrent disease. The development and progression of prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) has therefore been the cornerstone of treatment of advanced prostate cancer and is the first treatment intervention for Hormone Sensitive Prostate Cancer. The appropriate time (immediate versus delayed) to start Androgen Deprivation Therapy in patients with prostate cancer with rising PSA, as the only sign of relapse, has remained unclear. This has been partly due to lack of patient accruals and patient reluctance to be randomized, in these clinical trials.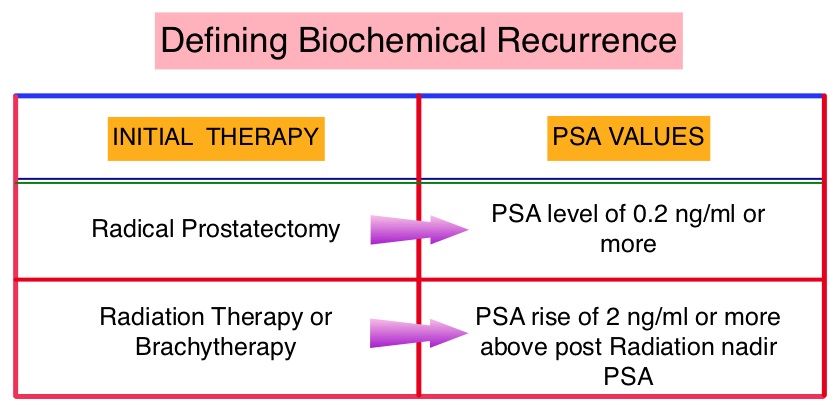
The authors conducted a randomized, prospective, phase III trial, to determine if immediate intervention with Androgen Deprivation Therapy (ADT) would improve Overall Survival (OS), compared with delayed ADT, in prostate cancer patients with PSA relapse, following previous attempted curative therapy (radiotherapy or surgery with or without postoperative radiotherapy) or in those considered not suitable for curative treatment (because of age, comorbidity or locally advanced disease). This analysis combined prostate cancer patients with PSA relapse enrolled in two separate studies. Two hundred and ninety three (N=293) eligible patients were randomly assigned 1:1 to immediate Androgen Deprivation Therapy (N= 142) or delayed ADT (N=151). The primary endpoint was Overall Survival. Secondary endpoints included Cancer-Specific Survival and Time to Clinical Progression. The median follow up was 5 years.
There was a statistically significant improvement in the Overall Survival, with a 45% reduction in the risk for death, for those receiving immediate ADT compared with the delayed treatment group (HR=0.55; P=0.05). Further, with immediate ADT, there was a statistically significant delay in the time to first local progression (HR= 0.51; P=0.001).
The authors concluded that immediate Androgen Deprivation Therapy significantly improved Overall Survival and Time to Clinical Progression for prostate cancer patients with PSA relapse, following immediate intervention with Androgen Deprivation Therapy. This benefit however must be weighed against the risks associated with long term Androgen Deprivation Therapy. Immediate ADT may be appropriate for patients with high risk features at the time of initial diagnosis, who present with early biochemical relapse after initial treatment and have a rapid PSA doubling time (less than 6 months). Timing of androgen-deprivation therapy in patients with prostate cancer with a rising PSA (TROG 03.06 and VCOG PR 01-03 [TOAD]): a randomised, multicentre, non-blinded, phase 3 trial. Duchesne GM, Woo HH, Bassett JK, et al. Lancet Oncol 2016;17:727-737