SUMMARY: The FDA on March 23, 2022, approved PLUVICTO® (Lutetium Lu 177 vipivotide tetraxetan) for the treatment of adult patients with Prostate-Specific Membrane Antigen (PSMA)-positive metastatic Castration-Resistant Prostate Cancer (mCRPC), who had been treated with Androgen Receptor (AR) pathway inhibition and Taxane-based chemotherapy. The FDA also approved LOCAMETZ® (Gallium Ga 68 gozetotide), a radioactive diagnostic agent for Positron Emission Tomography (PET) of PSMA-positive lesions, including selection of patients with metastatic prostate cancer for whom PLUVICTO® PSMA-directed therapy is indicated. LOCAMETZ® is the first radioactive diagnostic agent approved for patient selection in the use of a radioligand therapeutic agent.
The development and progression of prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) or testosterone suppression has therefore been the cornerstone of treatment of advanced prostate cancer, and is the first treatment intervention. Approximately 10-20% of patients with advanced Prostate cancer will progress to Castration Resistant Prostate Cancer (CRPC) within five years during ADT, and over 80% of these patients will have metastatic disease at the time of CRPC diagnosis. Among those patients without metastases at CRPC diagnosis, 33% are likely to develop metastases within two years. Progression to Castration Resistant Prostate Cancer (CRPC) often manifests itself with a rising PSA (Prostate Specific Antigen) and the estimated mean survival of patients with CRPC is 9-36 months, and there is therefore an unmet need for new effective therapies.
Prostate-Specific Membrane Antigen (PSMA) is a Type II cell membrane glycoprotein that is selectively expressed in prostate cells, with high levels of expression in prostatic adenocarcinoma. PSMA is a therefore an excellent target for molecular imaging and therapeutics, due to its high specificity for prostate cancer.
PLUVICTO® is a radiopharmaceutical that targets PSMA. It is comprised of Lutetium-177, a cytotoxic radionuclide , linked to the ligand PSMA-617, a small molecule designed to bind with high affinity to PSMA. Radioligand therapy with PLUVICTO® targets PSMA and releases its payload of lethal beta radiation into the prostate cancer cell. The antitumor activity and safety PLUVICTO® have been established previously in a Phase II study (Lancet Oncol. 2018;19:825-833).
VISION is an international, randomized, open-label Phase III study in which the benefit of PLUVICTO® was evaluated in men with PSMA-positive mCRPC, previously treated with second generation Androgen Receptor signaling pathway inhibitor (XTANDI® -Enzalutamide or ZYTIGA®-Abiraterone acetate), and 1 or 2 taxane chemotherapy regimens. In this trial, 831 patients were randomized 2:1 to receive PLUVICTO® 7.4 GBq (200 mCi) every 6 weeks for up to a total of 6 cycles plus Standard of Care as determined by the treating physician (N=551), or Standard of Care only (N=280). Both treatment groups were well balanced and this trial excluded patients treated with XOFIGO® (Radium-223). All enrolled patients received a GnRH analog or had prior bilateral orchiectomy and had a castrate level or serum/plasma testosterone of lower than 50ng/dL. PET imaging with LOCAMETZ® was used to determine PSMA positivity by central review. PSMA-positive mCRPC was defined as having at least one tumor lesion with LOCAMETZ® uptake greater than normal liver. Patients were excluded from enrollment if any lesions exceeding certain size criteria in the short axis had uptake less than or equal to uptake in normal liver. The Primary endpoints were radiographic Progression Free Survival (rPFS) by Independent Central Review (ICR) and Overall Survival (OS). Secondary endpoints included Objective Response Rate (ORR), Disease Control Rate (DCR), and time to first Symptomatic Skeletal Event (SSE). The median study follow up was 20.9 months.
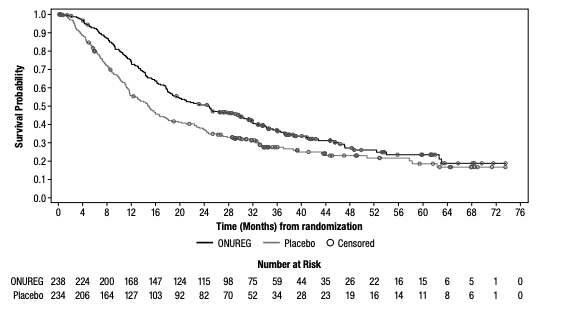
Treatment with the combination of PLUVICTO® plus Standard of Care resulted in a statistically significant improvement in the Primary endpoints of Overall Survival and radiographic Progression Free Survival. PLUVICTO® plus Standard of Care significantly improved rPFS by 60%, compared to Standard of Care alone (median rPFS 8.7 versus 3.4 months, HR=0.40; P<0.001). The median OS was also significantly improved by 38% in the study group (median OS 15.3 versus 11.3 months, HR=0.62; P<0.001). All key secondary endpoints including Objective Response Rate, Disease Control Rate, and time to first Symptomatic Skeletal Event were statistically significant, and in favor of PLUVICTO® plus Standard of Care. The most common adverse reactions in patients receiving PLUVICTO® were fatigue, dry mouth, nausea, decreased appetite, constipation, anemia, lymphopenia, thrombocytopenia, hypocalcemia and hyponatremia.
It was concluded that radioligand therapy with PLUVICTO® significantly improved radiographic Progression Free Survival and Overall Survival when added to Standard of Care, compared with Standard of Care alone, in men with PSMA-positive metastatic Castration Resistant Prostate Cancer.
Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. Sartor O, de Bono J, Chi KN, et al. N Engl J Med 2021; 385:1091-1103.