
The FDA on August 20, 2020, approved KYPROLIS® (Carfilzomib) and DARZALEX® (Daratumumab) in combination with Dexamethasone for adult patients with Relapsed or Refractory multiple myeloma who have received one to three lines of therapy. KYPROLIS® is a product of Onyx Pharmaceuticals, Inc. DARZALEX® is a product of Janssen Biotech, Inc.
Tag: Multiple Myeloma
BLENREP® (Belantamab mafodotin-blmf)
The FDA on August 5, 2020 approved BLENREP® for adult patients with Relapsed or Refractory Multiple Myeloma who have received at least 4 prior therapies, including an anti-CD38 monoclonal antibody, a Proteasome Inhibitor, and an Immunomodulatory agent. BLENREP® is a product of GlaxoSmithKline.
FDA Approves Subcutaneous DARZALEX® in Multiple Myeloma
SUMMARY: The FDA on May 1, 2020 approved DARZALEX® (Daratumumab) and Hyaluronidase-fihj (DARZALEX FASPRO®), for adult patients with newly diagnosed or Relapsed/Refractory multiple myeloma. This new product allows for subcutaneous dosing of DARZALEX®.
DARZALEX FASPRO® is now approved for these previously approved indications for IV DARZALEX®
1) In combination with VELCADE® (Bortezomib), Melphalan and Prednisone in newly diagnosed patients who are ineligible for Autologous Stem Cell Transplant (ASCT)
2) In combination with REVLIMID® (Lenalidomide) and Dexamethasone in newly diagnosed patients, who are ineligible for ASCT and in patients with Relapsed or Refractory multiple myeloma who have received at least one prior therapy
3) In combination with VELCADE® and Dexamethasone in patients who have received at least one prior therapy
4) As monotherapy, in patients who have received at least three prior lines of therapy including a Proteasome Inhibitor (PI) and an Immunomodulatory agent or who are double-refractory to a PI and an immunomodulatory agent.
DARZALEX® is a human IgG1 antibody that targets CD38, a transmembrane glycoprotein abundantly expressed on malignant plasma cells and with low levels of expression on normal lymphoid and myeloid cells. DARZALEX® exerts its cytotoxic effect on myeloma cells by multiple mechanisms, including Antibody Dependent Cellular Cytotoxicity (ADCC), Complement Dependent Cytotoxicity (CDC) and direct Apoptosis. Additionally, DARZALEX® may play a role in immunomodulation, by depleting CD38-positive regulator immune suppressor cells, and thereby expanding T cells, in patients responding to therapy.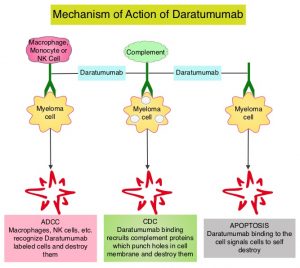
This FDA approval is based on COLUMBA Trial, which is a randomized, open-label, multicenter Phase III study, which included 522 patients with multiple myeloma, who had received at least three prior lines of therapy including a Proteasome Inhibitor (PI) and an immunomodulatory drug (IMiD), or whose disease was refractory to both a PI and an IMiD. Patients were randomly assigned to receive a fixed dose of subcutaneously (SC) administered formulation of DARZALEX® 1800 mg weekly for cycles 1-2, every two weeks for cycles 3-6 and every four weeks for cycle 7 and thereafter (N=263), with the subcutaneous preparation given over 3-5 minutes at alternating left and right abdominal sites. In the intravenous group, patients received DARZALEX® 16 mg/kg IV weekly for cycles 1-2, every two weeks for cycles 3-6 and every four weeks for cycle 7 and thereafter (N=259). Each cycle was 28 days. Treatment in both patient groups was continued until disease progression or unacceptable toxicity. The median age was 67 years and the median number of prior therapies was four in each treatment group. Patient characteristics were similar between the two arms except that more patients in the subcutaneous arm had high-risk cytogenetics (26%) compared with the intravenous group (17%). The median duration of treatment was approximately 5 months, with a median of 6 completed cycles of treatment. The median duration of infusion was consistently 5 minutes at each visit in the subcutaneous group. However, in the IV arm, the first infusion lasted 7 hours, the second infusion was 4.3 hours, and subsequent infusions lasted a median of 3.4 hours. The study co-Primary endpoints were Overall Response Rate (ORR) and pharmacokinetic endpoint of the maximum C-trough on cycle 3, day 1 pre-dose.
At a median follow up of 7.5 months, the ORR was 41% for the subcutaneous administered formulation of DARZALEX® compared to 37% for IV DARZALEX® (P<0.0001). The ORR was similar across all clinically relevant subgroups, including body weight. The ratio of geometric means of C-trough for the SC administered formulation of DARZALEX® over IV DARZALEX® was 108%. The Progression Free Survival was comparable between the SC administered formulation of DARZALEX and the current IV formulation of DARZALEX (HR=0.99; P<0.9258). A lower rate of infusion-related reactions was observed in the group that received the SC DARZALEX® compared to IV DARZALEX® (13% vs. 35%, respectively).
It was concluded that the subcutaneous formulation of DARZALEX® resulted in non-inferior pharmacokinetics and efficacy compared to the current IV formulation, and also importantly offers the potential for a fixed-dose administration, shorter administration times and a lower rate of infusion-related reactions with improved safety profile, in patients with Relapsed or Refractory multiple myeloma.
Subcutaneous versus intravenous daratumumab in patients with relapsed or refractory multiple myeloma (COLUMBA): a multicentre, open-label, non-inferiority, randomised, phase 3 trial. Mateos M-V, Nahi H, Legiec W, et al. The Lancet Haematology. Published: March 23, 2020. DOI: https://doi.org/10.1016/S2352-3026(20)30070-3.
DARZALEX FASPRO® (Daratumumab and Hyaluronidase-fihj)
The FDA on May 1, 2020 approved DARZALEX FASPRO® for adult patients with newly diagnosed or Relapsed/Refractory Multiple Myeloma. This new product allows for subcutaneous dosing of Daratumumab. DARZALEX FASPRO® is a product of Janssen Biotech, Inc.
SARCLISA® (Isatuximab-irfc)
The FDA on March 2, 2020 approved SARCLISA® in combination with POMALYST® (Pomalidomide) and Dexamethasone for adult patients with Multiple Myeloma, who have received at least two prior therapies including REVLIMID® (Lenalidomide) and a Proteasome Inhibitor. SARCLISA® is a product of Sanofi-Aventis U.S. LLC.
FDA Approves SARCLISA® for Relapsed Refractory Multiple Myeloma
SUMMARY: The FDA on March 2, 2020 approved SARCLISA® (Isatuximab-irfc) in combination with POMALYST® (Pomalidomide) and Dexamethasone for adult patients with multiple myeloma who have received at least two prior therapies including REVLIMID® (Lenalidomide) and a Proteasome Inhibitor. Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, 32,270 new cases will be diagnosed in 2020 and 12,830 patients are expected to die of the disease. Multiple Myeloma (MM) in 2020 remains an incurable disease. The therapeutic goal therefore is to improve Progression Free Survival (PFS) and Overall Survival (OS). Multiple Myeloma is a disease of the elderly, with a median age at diagnosis of 69 years and characterized by intrinsic clonal heterogeneity. Almost all patients eventually will relapse, and patients with a high-risk cytogenetic profile or refractory disease have the worst outcomes. The median survival for patients with myeloma is over 10 years.
CD38, a transmembrane glycoprotein abundantly expressed on malignant plasma cells and with low levels of expression on normal lymphoid and myeloid cells. DARZALEX® (Daratumumab) is a human IgG1 antibody that targets CD38, and was approved for use in combination with POMALYST® (Pomalidomide) and Dexamethasone in 2017, for the treatment of patients with multiple myeloma, who have received at least two prior therapies including REVLIMID® and a Proteasome Inhibitor. DARZALEX® exerts its cytotoxic effect on myeloma cells by multiple mechanisms, including Antibody Dependent Cellular Cytotoxicity (ADCC), Complement Mediated Cytotoxicity and direct apoptosis. Additionally, DARZALEX® may have a role in immunomodulation by depleting CD38-positive regulator Immune suppressor cells, and thereby expanding T cells, in patients responding to therapy.
SARCLISA® (Isatuximab) is a CD38-targeting monoclonal antibody, similar to DARZALEX®, but unlike DARZALEX®, is not associated with complement activation, and can therefore be more readily given to patients with asthma or Chronic Obstructive Pulmonary Disease. Further, SARCLISA® targets a specific epitope on the CD38 receptor, and this distinction from DARZALEX® allows use of SARCLISA® in cases when DARZALEX® fails. Additionally, SARCLISA® infusions are less cumbersome.
The present FDA approval of SARCLISA® was based on ICARIA-MM trial, which is an open-label, randomized, multicentre Phase III study in which 307 adult patients with Relapsed and Refractory multiple myeloma who had received at least two previous lines of treatment, including REVLIMID® and a Proteasome Inhibitor were eligible. Patients were excluded if they were refractory to previous treatment with an anti-CD38 monoclonal antibody. Patients were randomly assigned 1:1 to receive either SARCLISA® along with POMALYST® and low-dose Dexamethasone (N =154) or POMALYST® and low-dose Dexamethasone alone (N = 153). Treatment consisted of 28-day cycles of SARCLISA® 10 mg/kg given IV on days 1, 8, 15, and 22 in the first cycle and days 1 and 15 in subsequent cycles. Both groups received POMALYST® 4 mg orally on days 1 to 21 of each cycle and Dexamethasone 40 mg (20 mg for patients aged 75 years or older) oral or IV on days 1, 8, 15, and 22 of each cycle. Treatment was continued until disease progression or unacceptable toxicity. The Primary endpoint was Progression Free Survival (PFS), determined by an Independent Response Committee, and assessed in the intent-to-treat population.
At a median follow up of 11.6 months, the median PFS was 11.5 months in the SARCLISA® group versus 6.5 months in the control group (HR= 0.596; P=0.001). This PFS improvement represented a 40% reduction in the risk of disease progression or death in the SARCLISA® group. In a prespecified subgroup analyses, which included patients with poor prognostic features, and those refractory to REVLIMID®, a Proteasome Inhibitor, or both, the Hazard Ratios were consistently in favor of SARCLISA®.(HR=0.58). The most common adverse events of any grade in the SARCLISA® vs control groups were infusion reactions (38% versus 0%, of which 3% were Grade 3 or 4), upper respiratory tract infection (28% versus 17%), and diarrhea (26% versus 20%).
It was concluded that the addition of SARCLISA® to POMALYST® and Dexamethasone significantly improves Progression Free Survival in patients with Relapsed and Refractory multiple myeloma, and is an important new treatment option for the management of patients who become refractory to REVLIMID® and a Proteasome Inhibitor. Multiple Myeloma patients will soon have the opportunity to choose between two equally effective treatment options with various modes of administration. Isatuximab plus pomalidomide and low-dose dexamethasone versus pomalidomide and low-dose dexamethasone in patients with relapsed and refractory multiple myeloma (ICARIA-MM): a randomised, multicentre, open-label, phase 3 study. Attal M, Richardson PG, Rajkumar SV, et al. The Lancet. November 14, 2019 DOI:https://doi.org/10.1016/S0140-6736(19)32556-5
Late Breaking Abstract – ASH 2019: DARZALEX®, KYPROLIS® and Dexamethasone Combination Improves PFS in Relapsed or Refractory Multiple Myeloma
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, 32, 270 new cases will be diagnosed in 2020 and 12,830 patients are expected to die of the disease. Multiple Myeloma (MM) in 2020 remains an incurable disease. The therapeutic goal therefore is to improve Progression Free Survival (PFS) and Overall Survival (OS). Multiple Myeloma is a disease of the elderly, with a median age at diagnosis of 69 years and characterized by intrinsic clonal heterogeneity. Almost all patients eventually will relapse, and patients with a high-risk cytogenetic profile or refractory disease have the worst outcomes. The median survival for patients with Myeloma is over 10 years.
REVLIMID® (Lenalidomide) in combination with VELCADE® (Bortezomib) and Dexamethasone is the preferred regimen according to the NCCN guidelines, for both transplant and non-transplant candidates with newly diagnosed Multiple Myeloma, and when given continuously or with maintenance therapy, has improved survival outcomes. Nonetheless, a significant number of patients progress while on these agents or discontinue therapy due to toxicities. There is therefore a need for effective and tolerable regimens for patients who are exposed or refractory to REVLIMID® or VELCADE®.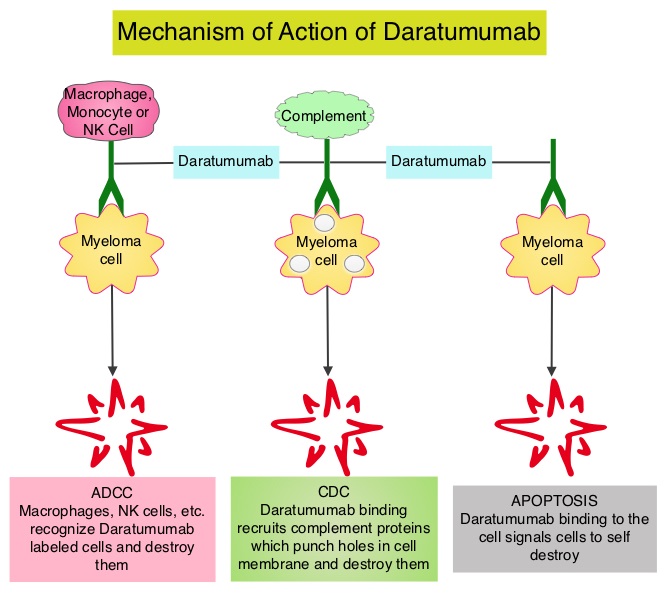
KYPROLIS® (Carfilzomib) is a second generation selective, epoxyketone Proteasome Inhibitor and unlike VELCADE®, proteasome inhibition with KYPROLIS® is irreversible. DARZALEX® (Daratumumab) is a human IgG1 antibody that targets CD38, a transmembrane glycoprotein abundantly expressed on malignant plasma cells and with low levels of expression on normal lymphoid and myeloid cells. DARZALEX® exerts its cytotoxic effect on myeloma cells by multiple mechanisms, including Antibody Dependent Cellular Cytotoxicity (ADCC), Complement Dependent Cytotoxicity (CDC) and direct Apoptosis. Additionally, DARZALEX® may play a role in immunomodulation, by depleting CD38-positive regulator immune suppressor cells, and thereby expanding T cells, in patients responding to therapy. Both KYPROLIS® and DARZALEX® are approved as single agents, as well as in combination with other drugs, for the treatment of patients with Relapsed/Refractory Multiple Myeloma. In a Phase I study, KYPROLIS® in combination with Dexamethasone and DARZALEX® demonstrated safety and efficacy in patients Relapsed/Refractory Multiple Myeloma.
CANDOR is a multicenter, open-label, Phase III trial, which included Relapsed/Refractory Multiple Myeloma patients with measurable disease who had received 1-3 prior lines of therapy, with Partial Response or better to one or more lines of therapy. A total of 466 patients were randomly assigned 2:1 to receive triplet of KYPROLIS®, Dexamethasone, and DARZALEX® (KdD)- N=312 or KYPROLIS® and Dexamethasone (Kd) alone- N=154. All patients received KYPROLIS® as a 30 minute IV infusion on days 1, 2, 8, 9, 15, and 16 of each 28-day cycle (20 mg/m2 on days 1 and 2 during cycle 1 and 56 mg/m2 thereafter). DARZALEX® 8 mg/kg was administered IV on days 1 and 2 of cycle 1 and at 16 mg/kg once weekly for the remaining doses of the first 2 cycles, then every 2 weeks for 4 cycles (cycles 3-6), and every 4 weeks thereafter. All patients received Dexamethasone 40 mg oral or IV weekly (20 mg for patients over 75 years of age). The median age was 64 years, 42% and 90% received prior REVLIMID® and VELCADE® (Bortezomib) containing regimens respectively, and a third of patients were refractory to REVLIMID®. The Primary endpoint was Progression Free Survival (PFS) and Secondary endpoints including Overall Response Rate (ORR), Minimal Residual Disease (MRD)-negative status, Complete Response (CR) rate at 12 months, Overall Survival (OS), Duration of Response, and Safety.
After a median follow up of 17 months, the study met its Primary endpoint and the median PFS was not reached for the KdD arm and was 15.8 months for the Kd arm (HR=0.63; P=0014). This represented a 37% reduction in the risk of progression or death in the KdD group. The PFS benefit of KdD was maintained across prespecified subgroups, particularly among REVLIMID®-exposed and REVLIMID®-refractory patients. The ORR was 84.3% in the KdD group versus 74.7% in the Kd group (P=0.004), with a CR rate or better of 28.5% versus 10.4% respectively. The median time to first response was one month in both treatment groups. Patients treated with KdD achieved deeper responses which was nearly 10 times higher, with a MRD-negative Complete Response rate at 12 months of 12.5% for KdD versus 1.3% for Kd (P<0.0001). The median treatment duration was longer in the KdD group compared to the Kd group (70.1 versus 40.3 wks). The median OS was not reached in either groups, at a median follow up time of 17 months. Toxicities were generally manageable and the incidence of Adverse Events leading to treatment discontinuation was similar in both treatment groups.
It was concluded that a combination of KYPROLIS® along with Dexamethasone and DARZALEX® resulted in a significant PFS benefit over KYPROLIS® and Dexamethasone alone, with deeper responses, and the PFS benefit of KdD was maintained across prespecified, clinically important subgroups, particularly REVLIMID®-exposed and REVLIMID®-refractory patients. The authors added that KdD regimen should be considered as a novel, efficacious, and tolerable immunomodulatory-free treatment option for Relapsed/Refractory Multiple Myeloma patients. Carfilzomib, Dexamethasone, and Daratumumab Versus Carfilzomib and Dexamethasone for the Treatment of Patients with Relapsed or Refractory Multiple Myeloma (RRMM): Primary Analysis Results from the Randomized, Open-Label, Phase 3 Study Candor (NCT03158688). Usmani SZ, Quach H, Mateos M-V, et al. Presented at the 61st American Society of Hematology Annual Meeting and Exposition; Orlando, Florida; December 7-10, 2019; Abstract LBA-6.
Late Breaking Abstract – ASH 2019: DARZALEX®, KYPROLIS® and Dexamethasone Combination Improves PFS in Relapsed or Refractory Multiple Myeloma
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, 32, 270 new cases will be diagnosed in 2020 and 12,830 patients are expected to die of the disease. Multiple Myeloma (MM) in 2020 remains an incurable disease. The therapeutic goal therefore is to improve Progression Free Survival (PFS) and Overall Survival (OS). Multiple Myeloma is a disease of the elderly, with a median age at diagnosis of 69 years and characterized by intrinsic clonal heterogeneity. Almost all patients eventually will relapse, and patients with a high-risk cytogenetic profile or refractory disease have the worst outcomes. The median survival for patients with Myeloma is over 10 years.
REVLIMID® (Lenalidomide) in combination with VELCADE® (Bortezomib) and Dexamethasone is the preferred regimen according to the NCCN guidelines, for both transplant and non-transplant candidates with newly diagnosed Multiple Myeloma, and when given continuously or with maintenance therapy, has improved survival outcomes. Nonetheless, a significant number of patients progress while on these agents or discontinue therapy due to toxicities. There is therefore a need for effective and tolerable regimens for patients who are exposed or refractory to REVLIMID® or VELCADE®.
KYPROLIS® (Carfilzomib) is a second generation selective, epoxyketone Proteasome Inhibitor and unlike VELCADE®, proteasome inhibition with KYPROLIS® is irreversible. DARZALEX® (Daratumumab) is a human IgG1 antibody that targets CD38, a transmembrane glycoprotein abundantly expressed on malignant plasma cells and with low levels of expression on normal lymphoid and myeloid cells. DARZALEX® exerts its cytotoxic effect on myeloma cells by multiple mechanisms, including Antibody Dependent Cellular Cytotoxicity (ADCC), Complement Dependent Cytotoxicity (CDC) and direct Apoptosis. Additionally, DARZALEX® may play a role in immunomodulation, by depleting CD38-positive regulator immune suppressor cells, and thereby expanding T cells, in patients responding to therapy. Both KYPROLIS® and DARZALEX® are approved as single agents, as well as in combination with other drugs, for the treatment of patients with Relapsed/Refractory Multiple Myeloma. In a Phase I study, KYPROLIS® in combination with Dexamethasone and DARZALEX® demonstrated safety and efficacy in patients Relapsed/Refractory Multiple Myeloma.
CANDOR is a multicenter, open-label, Phase III trial, which included Relapsed/Refractory Multiple Myeloma patients with measurable disease who had received 1-3 prior lines of therapy, with Partial Response or better to one or more lines of therapy. A total of 466 patients were randomly assigned 2:1 to receive triplet of KYPROLIS®, Dexamethasone, and DARZALEX® (KdD)- N=312 or KYPROLIS® and Dexamethasone (Kd) alone- N=154. All patients received KYPROLIS® as a 30 minute IV infusion on days 1, 2, 8, 9, 15, and 16 of each 28-day cycle (20 mg/m2 on days 1 and 2 during cycle 1 and 56 mg/m2 thereafter). DARZALEX® 8 mg/kg was administered IV on days 1 and 2 of cycle 1 and at 16 mg/kg once weekly for the remaining doses of the first 2 cycles, then every 2 weeks for 4 cycles (cycles 3-6), and every 4 weeks thereafter. All patients received Dexamethasone 40 mg oral or IV weekly (20 mg for patients over 75 years of age). The median age was 64 years, 42% and 90% received prior REVLIMID® and VELCADE® (Bortezomib) containing regimens respectively, and a third of patients were refractory to REVLIMID®. The Primary endpoint was Progression Free Survival (PFS) and Secondary endpoints including Overall Response Rate (ORR), Minimal Residual Disease (MRD)-negative status, Complete Response (CR) rate at 12 months, Overall Survival (OS), Duration of Response, and Safety.
After a median follow up of 17 months, the study met its Primary endpoint and the median PFS was not reached for the KdD arm and was 15.8 months for the Kd arm (HR=0.63; P=0014). This represented a 37% reduction in the risk of progression or death in the KdD group. The PFS benefit of KdD was maintained across prespecified subgroups, particularly among REVLIMID®-exposed and REVLIMID®-refractory patients. The ORR was 84.3% in the KdD group versus 74.7% in the Kd group (P=0.004), with a CR rate or better of 28.5% versus 10.4% respectively. The median time to first response was one month in both treatment groups. Patients treated with KdD achieved deeper responses which was nearly 10 times higher, with a MRD-negative Complete Response rate at 12 months of 12.5% for KdD versus 1.3% for Kd (P<0.0001). The median treatment duration was longer in the KdD group compared to the Kd group (70.1 versus 40.3 wks). The median OS was not reached in either groups, at a median follow up time of 17 months. Toxicities were generally manageable and the incidence of Adverse Events leading to treatment discontinuation was similar in both treatment groups.
It was concluded that a combination of KYPROLIS® along with Dexamethasone and DARZALEX® resulted in a significant PFS benefit over KYPROLIS® and Dexamethasone alone, with deeper responses, and the PFS benefit of KdD was maintained across prespecified, clinically important subgroups, particularly REVLIMID®-exposed and REVLIMID®-refractory patients. The authors added that KdD regimen should be considered as a novel, efficacious, and tolerable immunomodulatory-free treatment option for Relapsed/Refractory Multiple Myeloma patients. Carfilzomib, Dexamethasone, and Daratumumab Versus Carfilzomib and Dexamethasone for the Treatment of Patients with Relapsed or Refractory Multiple Myeloma (RRMM): Primary Analysis Results from the Randomized, Open-Label, Phase 3 Study Candor (NCT03158688). Usmani SZ, Quach H, Mateos M-V, et al. Presented at the 61st American Society of Hematology Annual Meeting and Exposition; Orlando, Florida; December 7-10, 2019; Abstract LBA-6.
DARZALEX® Combination Improves Overall Survival in Transplant-Ineligible Myeloma Patients
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, 32,110 new cases will be diagnosed in 2019 and 12,960 patients are expected to die of the disease. Multiple Myeloma (MM) in 2019 remains an incurable disease. The therapeutic goal therefore is to improve Progression Free Survival (PFS) and Overall Survival (OS). Multiple Myeloma is a disease of the elderly, with a median age at diagnosis of 69 years and characterized by intrinsic clonal heterogeneity. Almost all patients eventually will relapse, and patients with a high-risk cytogenetic profile or refractory disease have the worst outcomes. The median survival for patients with myeloma is over 10 years.
Elderly patients with myeloma in the US are often treated with a combination of REVLIMID® (Lenalidomide) and Dexamethasone, whereas Melphalan, Prednisone, and Thalidomide (MPT) and VELCADE® (Bortezomib), Melphalan and Prednisone (VMP) are the most widely used regimens outside the US. These regimens are associated with a PFS of 18-24 months and an OS of 4-5 years. For patients with newly diagnosed multiple myeloma who are ineligible for ASCT, treatment with VMP regimen has been a standard effective regimen, based on the VISTA (Velcade as Initial Standard Therapy in Multiple Myeloma: Assessment with Melphalan and Prednisone) trial.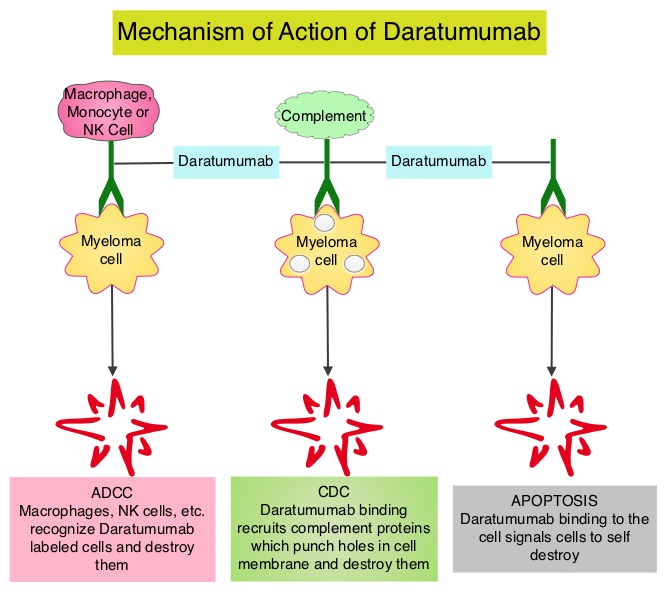
DARZALEX® (Daratumumab) is a human IgG1 antibody that targets CD38, a transmembrane glycoprotein abundantly expressed on malignant plasma cells and with low levels of expression on normal lymphoid and myeloid cells. DARZALEX® exerts its cytotoxic effect on myeloma cells by multiple mechanisms, including Antibody Dependent Cellular Cytotoxicity (ADCC), Complement Dependent Cytotoxicity (CDC) and direct Apoptosis. Additionally, DARZALEX® may have a role in immunomodulation, by depleting CD38-positive regulator immune suppressor cells, and thereby expanding T cells, in patients responding to therapy.
ALCYONE is a multicenter, randomized, open-label, active-controlled, Phase III trial in which DARZALEX® given along with VELCADE®, Melphalan and Prednisone (D-VMP regimen) was compared with VMP alone (control group), in patients with newly diagnosed multiple myeloma, who were ineligible for Autologous Stem Cell Transplantation (ASCT). Of the 706 enrolled patients, 350 were assigned to the DARZALEX® group and 356 to the control group. The median age was 71 yrs. All the patients received up to nine 6 week cycles of VELCADE® 1.3 mg/m2 SQ, twice weekly on weeks 1, 2, 4, and 5 of cycle 1 and once weekly on weeks 1, 2, 4, and 5 of cycles 2-9), Melphalan 9 mg/m2 orally, once daily on days 1-4 of each cycle, and Prednisone 60 mg/m2 once daily on days 1-4 of each cycle. In the study group, patients received DARZALEX® 16 mg/kg IV administered with Dexamethasone 20 mg oral or IV (to manage infusion reactions), once weekly for a total of 6 doses, every 3 weeks for a total of 16 doses and every 4 weeks thereafter until disease progression or unacceptable toxicity. The Primary end point was Progression Free Survival (PFS). Secondary end points included Overall Response Rate (ORR), rates of Very Good Partial Response (VGPR), Complete Response (CR) rate, Minimal Residual Disease (MRD) negativity and Overall Survival (OS). The FDA in 2018 approved DARZALEX® in combination with VELCADE® (Bortezomib), a proteasome inhibitor, Melphalan, an alkylating agent and Prednisone VMP regimen), for the treatment of patients with newly diagnosed multiple myeloma who are ineligible for Autologous Stem Cell Transplant (ASCT), based on the Progression Free Survival (PFS) benefit at 16.5 months, noted during the primary analysis of the ALCYONE study. The authors herein presented outcomes after more than 36 months of follow-up from the ALCYONE study, including analysis of Overall Survival (OS) from a prespecified interim analysis.
In this updated analysis, treatment with D-VMP continued to demonstrate a twofold greater median PFS at 36.4 months versus 19.3 months with VMP, after a median follow-up of 41months (HR=0.42; P<0.0001). Patients assigned to D-VMP also had significantly prolonged PFS on subsequent therapy (PFS-2). Median PFS-2 was not reached with D-VMP versus 42.3 months with VMP (HR=0.55; P<0.0001), representing a 45% reduction in the risk for progression or death. The median time to subsequent therapy had yet to be reached in the D-VMP group versus 25.9 months for the VMP group. The Overall Response Rate was 91% in the D-VMP group as compared with 74% in the control group and the rate of Complete Response or better (including stringent CR) was 46%, versus 24.4% in the control group. The MRD-negative rate (at a threshold of 1 tumor cell per 105 white cells) was 28% with D-VMP and 7% with VMP and D-VMP also led to higher rates of sustained MRD negativity. MRD negativity for 12 or more months was associated with improved PFS. The estimated 36 month OS rate was 78% with D-VMP versus 68% with VMP, with a significant benefit for OS observed for D-VMP versus VMP alone (HR=0.60; P=0.0003). This represented a 40% reduction in the risk of death, in favor of D-VMP.
The authors concluded that for the first time, this study demonstrated that the addition of DARZALEX® to VMP significantly prolonged Overall Survival in patients with transplant-ineligible newly diagnosed Multiple Myeloma, with a 40% reduction in the risk of death, when compared with VMP alone. They added that these findings, together with the Phase 3 MAIA study (DARZALEX® plus Lenalidomide and Dexamethasone versus Lenalidomide plus Dexamethasone), continue to support the addition of DARZALEX® to frontline treatment regimens for patients with Multiple Myeloma. Daratumumab Plus Bortezomib, Melphalan, and Prednisone Versus Bortezomib, Melphalan, and Prednisone in Patients with Transplant-Ineligible Newly Diagnosed Multiple Myeloma: Overall Survival in Alcyone. Mateos MV, Cavo M, Bladé J, et al. Presented at: 2019 ASH Annual Meeting; December 7-10, 2019; Orlando, FL. Abstract 859.
Isatuximab Combination Significantly Improves Progression Free Survival in Relapsed/Refractory Myeloma
SUMMARY: Multiple Myeloma is a clonal disorder of plasma cells in the bone marrow and the American Cancer Society estimates that in the United States, 32,110 new cases will be diagnosed in 2019 and 12,960 patients are expected to die of the disease. Multiple Myeloma (MM) in 2019 remains an incurable disease. The therapeutic goal therefore is to improve Progression Free Survival (PFS) and Overall Survival (OS). Almost all patients eventually will relapse, and patients with a high-risk cytogenetic profile or refractory disease have the worst outcomes. Multiple Myeloma is a disease of the elderly, with a median age at diagnosis of 69 years and characterized by intrinsic clonal heterogeneity.
CD38, a transmembrane glycoprotein abundantly expressed on malignant plasma cells and with low levels of expression on normal lymphoid and myeloid cells. DARZALEX® (Daratumumab) is a human IgG1 antibody that targets CD38 and was approved for use in combination with POMALYST® (Pomalidomide) and Dexamethasone in 2017, for the treatment of patients with multiple myeloma who have received at least two prior therapies including REVLIMID® (Lenalidomide) and a Proteasome Inhibitor. DARZALEX® exerts its cytotoxic effect on myeloma cells by multiple mechanisms, including Antibody Dependent Cellular Cytotoxicity (ADCC), Complement Mediated Cytotoxicity and direct apoptosis. Additionally, DARZALEX® may have a role in immunomodulation by depleting CD38-positive regulator Immune suppressor cells, and thereby expanding T cells, in patients responding to therapy.
Isatuximab is a CD38-targeting monoclonal antibody, similar to DARZALEX®, but unlike DARZALEX®, is not associated with complement activation, and can therefore be more readily given to patients with asthma or Chronic Obstructive Pulmonary Disease. Further, Isatuximab targets a specific epitope on the CD38 receptor, and this distinction from DARZALEX® could position Isatuximab for use in cases when DARZALEX® fails. Additionally, Isatuximab infusions are less cumbersome.
ICARIA-MM trial is an open-label, randomized, multicentre Phase III study in which 307 adult patients with Relapsed and Refractory multiple myeloma who had received at least two previous lines of treatment, including REVLIMID® and a Proteasome Inhibitor were eligible. Patients were excluded if they were refractory to previous treatment with an anti-CD38 monoclonal antibody. Patients were randomly assigned 1:1 to receive either Isatuximab along with POMALYST® and low-dose Dexamethasone (N =154) or POMALYST® and low-dose Dexamethasone (N = 153). Treatment consisted of 28-day cycles of Isatuximab 10 mg/kg given IV on days 1, 8, 15, and 22 in the first cycle and days 1 and 15 in subsequent cycles. Both groups received POMALYST® 4 mg orally on days 1 to 21 of each cycle and Dexamethasone 40 mg (20 mg for patients aged 75 years or older) oral or IV on days 1, 8, 15, and 22 of each cycle. Treatment was continued until disease progression or unacceptable toxicity. The Primary endpoint was Progression Free Survival, determined by an Independent Response Committee, and assessed in the intent-to-treat population.
At a median follow-up of 11.6 months, the median PFS was 11.5 months in the Isatuximab group versus 6.5 months in the control group (HR= 0.596; P=0.001). In prespecified subgroup analyses, which included patients with poor prognostic features, and those refractory to REVLIMID®, a Proteasome Inhibitor, or both, the Hazard Ratios were consistently in favor of Isatuximab.(HR=0.58). The most common adverse events of any grade in the Isatuximab vs control groups were infusion reactions (38% versus 0%, of which 3% were Grade 3 or 4), upper respiratory tract infection (28% versus 17%), and diarrhea (26% versus 20%).
It was concluded that the addition of Isatuximab to POMALYST® and Dexamethasone significantly improves Progression Free Survival in patients with Relapsed and Refractory multiple myeloma, and is an important new treatment option for the management of patients who become refractory to REVLIMID® and a Proteasome Inhibitor. Multiple myeloma patients will soon have the opportunity to choose between two equally effective treatment options with various modes of administration. Isatuximab plus pomalidomide and low-dose dexamethasone versus pomalidomide and low-dose dexamethasone in patients with relapsed and refractory multiple myeloma (ICARIA-MM): a randomised, multicentre, open-label, phase 3 study. Attal M, Richardson PG, Rajkumar SV, et al. The Lancet. November 14, 2019 DOI:https://doi.org/10.1016/S0140-6736(19)32556-5